


Recognition of Community Pharmacists’ Behaviors Related to Information Sharing: A Cross-Sectional Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Sample Size
2.3. Survey Contents
2.4. Statistical Analyses
3. Results
3.1. Respondent Attributes
3.2. Differences between Patients and Pharmacists Regarding the Recognition of Pharmacists’ Behaviors Related to Information Sharing
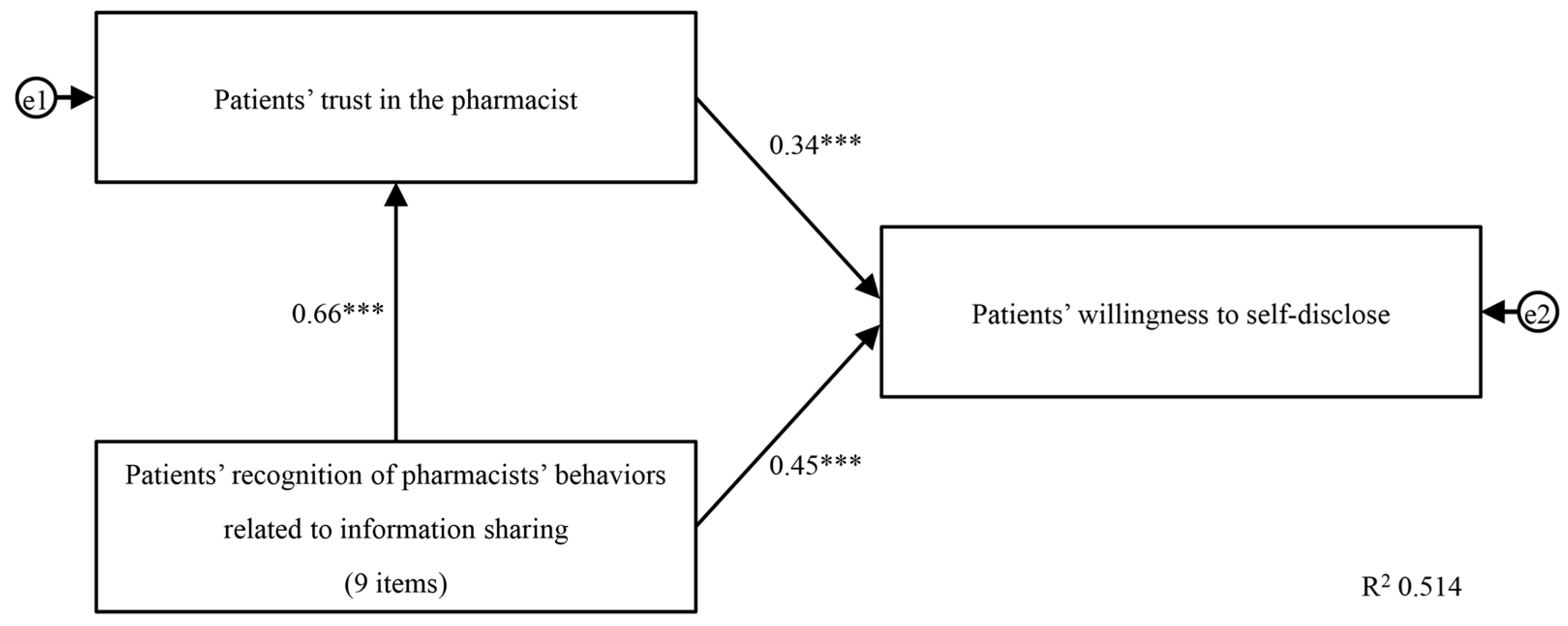
3.3. Patients’ Recognition of Pharmacists’ Behaviors Related to Information Sharing and Its Association with Patients’ Trust in Community Pharmacists and Willingness to Self-Disclose
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hastert, J.D. Medicare Prescription Drug, Improvement, and Modernization Act of 2003. 2023. Available online: https://www.congress.gov/bill/108th-congress/house-bill/1 (accessed on 15 August 2023).
- AARP; Academy of Managed Care Pharmacy; American College of Clinical Pharmacy; American Geriatrics Society; American Pharmacists Association; American Society of Consultant Pharmacists; Case Management Society of America; College of Psychiatric and Neurologic Pharmacists; Department of Veterans Affairs. Sound medication therapy management programs. Case Manag. 2006, 17, 47–50. [Google Scholar]
- American Society of Health System Pharmacists; Academy of Managed Care Pharmacy. Summary of the executive sessions on medication therapy management programs: Bethesda, Maryland, June 14 and August 18. Am. J. Health Syst. Pharm. 2004, 62, 585–592. [Google Scholar]
- American Pharmacists Association; National Association of Chain Drug Stores Foundation. Medication therapy management in pharmacy practice: Core elements of an MTM service model (version 2.0). J. Am. Pharm. Assoc. 2008, 48, 341–353. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Vision of “Pharmacy for Patients”. In Front-Door Pharmacy to “Family-Care Pharmacy” and “Community”—Has Been Formulated. 2015. Available online: https://www.mhlw.go.jp/file/04-Houdouhappyou-11121000-Iyakushokuhinkyoku-Soumuka/vision_1.pdf (accessed on 25 August 2023).
- Ministry of Health, Labour and Welfare. Explanation of the 2022 Revision of Medical Reimbursement. 2022. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000196352_00008.html (accessed on 15 August 2023).
- Kawachi, A.; Tomishige, E.; Shibata, Y.; Narumi, K.; Sonoda, J.; Takeda, Y.; Motoya, T. Implementation of a lecture on “dispensing fee” for the local residents and its effects. Off. J. Jpn. Prim. Care Assoc. 2013, 36, 99–105. (In Japanese) [Google Scholar] [CrossRef]
- Katsuki, M.; Toriyama, A.; Tajima, F.; Kubota, T.; Moriuchi, H.; Irikura, M. Survey of patients’ criteria to choose a proper insurance pharmacy to become a pharmacy chosen by patients. J. Community Pharm. Pharm. Sci. 2020, 12, 129–134. [Google Scholar]
- Sakurai, T.; Fukuoka, K.; Yamada, T.; Hatakeyama, T.; Yamazaki, S.; Hashimoto, N.; Ihara, S.; Yuge, S. What patients expect from insurance pharmacies: National Pharmacy Satisfaction Survey. Med. Cons. New Remed. 2020, 57, 601–608. (In Japanese) [Google Scholar]
- Gidman, W.; Ward, P.; McGregor, L. Understanding public trust in services provided by community pharmacists relative to those provided by general practitioners: A qualitative study. BMJ Open 2012, 2, e000939. [Google Scholar] [CrossRef] [PubMed]
- Worley, M.M.; Schommer, J.C.; Brown, L.M.; Hadsall, R.S.; Ranelli, P.L.; Stratton, T.P.; Uden, D.L. Pharmacists’ and patients’ roles in the pharmacist-patient relationship: Are pharmacists and patients reading from the same relationship script? Res. Soc. Adm. Pharm. 2007, 3, 47–69. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.G.; Lee, N.E.; Sohn, H.S. Gap between patient expectation and perception during pharmacist-patient communication at community pharmacy. Int. J. Clin. Pharm. 2020, 42, 677–684. [Google Scholar] [CrossRef]
- Inoue, Y.; Saitoh, R.; Kanamoto, I.; Tajima, K.; Tomioka, K.; Taguchi, M. Attitude survey of pharmacists in pharmacies and patients regarding correspondence. J. Pharm. Commun. Soc. Jpn. 2012, 10, 16–23. (In Japanese) [Google Scholar]
- Takeishi, K.; Takase, M.; Takahashi, Y. Expectations of patients toward pharmacy and pharmacists: A questionnaire-based study. Pharmacometrics 2018, 93, 91–95. (In Japanese) [Google Scholar]
- Takase, M.; Takeishi, M.; Ohshima, H. Questionnaire survey on attitudes of pharmacist functions to patients recognized by pharmacists—Comparison with expectation of patient’s pharmacies/pharmacists. Pharmacometrics 2019, 96, 21–25. (In Japanese) [Google Scholar]
- Kishimoto, K.; Kumaki, R.; Kiyozuka, C.; Sakurai, H. A study of factors that promote patients’ provision of information to pharmacists and evaluation items for evaluating patients’ willingness to provide information. Jpn. J. Soc. Pharm. 2022, 41, 45–55. (In Japanese) [Google Scholar]
- DRUG Magazine Editorial Department. Dispensing pharmacy chain company ranking. DRUG Mag. 2023, 66, 58–63. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, K.; Hasaka, A.; Yamaura, K.; Fukushima, N. Whether visual information loss of expression by community pharmacist masks to effect a change in feeling of trust among help-seeker? Yakugaku Zasshi 2016, 136, 1401–1413. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Kiyozuka, C.; Kumaki, R.; Sakurai, H.; Kishimoto, K. Study factors affecting patients’ intention to provide information to pharmacist: Publicizing the contribution of pharmacists to pharmacotherapy through animation video. Jpn. J. Soc. Pharm. 2023, 42, 75–88. [Google Scholar]
- Mizumoto, A.; Takeuchi, O. Basics and considerations for reporting effect sizes in research papers. Stud. Eng. Educ. 2008, 31, 57–66. (In Japanese) [Google Scholar]
- Hayes, A.F.; Coutts, J.J. Use omega rather than Cronbach’s alpha for estimating reliability. But…. Commun. Methods Meas. 2020, 14, 1–24. [Google Scholar] [CrossRef]
- Hayes, A.F. SPSS, SAS, and R Macros and Code. 2020. Available online: https://www.afhayes.com/spss-sas-and-r-macros-and-code.html (accessed on 19 August 2023).
- Ministry of Health, Labour and Welfare. Summary of Physician, Dentist, and Pharmacist Statistics. 2020. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/ishi/20/index.html (accessed on 14 August 2023).
- Toyoda, H. (Ed.) Multiple regression analysis. In Covariance Structure Analysis [Amos Ed.]—Structural Equation Modelling; Tokyo Tosho Co., Ltd.: Tokyo, Japan, 2007; pp. 52–53. [Google Scholar]
- Tsushima, E. How multiple regression analysis works. In Medical Multivariate Data Analysis in SPSS; Tsushima, E., Ed.; Tokyo Tosho Co., Ltd.: Tokyo, Japan, 2018; pp. 41–56. [Google Scholar]
- Jamil, N.; Zainal, Z.A.; Alias, S.H.; Chong, L.Y.; Hashim, R. A systematic review of behaviour change techniques in pharmacist-delivered self-management interventions towards patients with chronic obstructive pulmonary disease. Res. Social. Adm. Pharm. 2023, 19, 1131–1145. [Google Scholar] [CrossRef]
- Batten, M.; Kosari, S.; Koerner, J.; Naunton, M.; Cargo, M. Evaluation approaches, tools and aspects of implementation used in pharmacist interventions in residential aged care facilities: A scoping review. Res. Social. Adm. Pharm. 2022, 18, 3714–3723. [Google Scholar] [CrossRef] [PubMed]
- Druică, E.; Ianole-Călin, R.; Băicuș, C.; Dinescu, R. Determinants of satisfaction with services, and trust in the information received in community pharmacies: A comparative analysis to foster pharmaceutical care adoption. Healthcare 2021, 9, 562. [Google Scholar] [CrossRef] [PubMed]
- Kirino, Y.; Masuyama, K. Survey and Research on the Current State of Pharmacy and Pharmacist Operations and How They Should Be Conducted. Grant-in-Aid for Scientific Research by the Ministry of Health, Labour and Welfare (Research Project for Regulatory Science Policy on Drugs and Medical Devices). 2015. Available online: https://mhlw-grants.niph.go.jp/system/files/2015/154041/201523020A_upload/201523020A0003.pdf (accessed on 25 December 2023). (In Japanese).
- Sakurai, H.; Kawahara, S.; Tada, Y.; Nakajima, F.; Igari, T.; Momose, H.; Kondo, H.; Komori, Y.; Hayase, Y. An investigation on patient satisfaction at community pharmacies: Analyzing questionnaire survey by structural equation modeling and multiple regression analysis. Yakugaku Zasshi 2007, 127, 1115–1123. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Ministerial Ordinance to Provide for a System for Conducting the Business of Pharmacies and Over-the-Counter Sales Business and Placement Sales Business. 2023. Available online: https://www.mhlw.go.jp/web/t_doc?dataId=81011000&dataType=0&pageNo=1 (accessed on 25 December 2023).


{kind=link}
| Characteristics | Values | |
|---|---|---|
| Age, years (median (IQR)) | 55.0 | (43.0–67.0) |
| Gender (n, (%)) | ||
| Male | 300 | (50.0) |
| Female | 300 | (50.0) |
| Number of medications (median (IQR)) | 3.0 | (2.0–5.0) |
| Use of more than one pharmacy (n, (%)) | 132 | (22.0) |
| An explanation was provided by the family pharmacist (n, (%)) | 463 | (77.2) |
| Medical condition (n, (%)) | ||
| Hypertension | 200 | (33.3) |
| Dyslipidemia | 122 | (20.3) |
| Psychiatric diseases | 105 | (17.5) |
| Allergic disease | 95 | (15.8) |
| Insomnia | 62 | (10.3) |
| Trust in pharmacist (min 6–max 42, median (IQR)) | 28.0 | (24.0–31.0) |
| Willingness to self-disclose (min 5–max 35, median (IQR)) | 20.0 | (15.0–24.0) |
| Characteristics | Values | |
|---|---|---|
| Years of experience (median (IQR)) | 8 | (4–15) |
| Gender (n, (%)) | ||
| Male | 194 | (32.8) |
| Female | 397 | (67.2) |
| Certifications (n, (%)) | ||
| One or more certifications | 488 | (82.2) |
| Education system-qualified by the Japan Education Pharmacists Center | 479 | (81.0) |
| Primary care-certified pharmacist | 1 | (0.2) |
| Board-Certified Pharmacist in Home Care Pharmacy | 3 | (0.5) |
| JPEC-Certified Pharmacist in Pediatric Pharmacotherapy | 2 | (0.3) |
| Pharmacist certified in Chinese and other herbal medicines | 10 | (1.7) |
| Certified Practical Training Supervisor Pharmacist | 56 | (9.5) |
| Pharmacists’ Behaviors Related to Information Sharing a | Patients | Pharmacists | ||||||
|---|---|---|---|---|---|---|---|---|
| (n = 600) b | (n = 591) b | p Value c | Effect Size r | |||||
| 1 | Talk with patients about how to watch for medication side effects. | 4 | (3–5) | 6 | (5–6) | <0.001 | 0.53 | Large |
| 2 | Talk with patients even if the patients do not have any medication questions. | 5 | (4–5) | 6 | (5–6) | <0.001 | 0.41 | Medium |
| 3 | Talk with patients about whether it is OK to take their medications with over-the-counter products. | 4 | (3–5) | 6 | (5–6) | <0.001 | 0.53 | Large |
| 4 | Show an interest in working with patients to meet their healthcare needs. | 4 | (3–5) | 6 | (5–6) | <0.001 | 0.51 | Large |
| 5 | Communicate a desire to help patients manage their medications. | 4 | (3–5) | 5 | (5–6) | <0.001 | 0.53 | Large |
| 6 | Make sure that patients understand how to use their medications before they leave the pharmacy. | 4 | (4–5) | 6 | (5–6) | <0.001 | 0.48 | Medium |
| 7 | Communicate a desire to help patients with their medication concerns. | 4 | (3–5) | 6 | (5–6) | <0.001 | 0.59 | Large |
| 8 | Listen to patients when they have a medication question. | 5 | (4–6) | 7 | (6–7) | <0.001 | 0.64 | Large |
| 9 | Be easily approachable to discuss a patient’s medication concerns. | 5 | (4–6) | 6 | (5–6) | <0.001 | 0.39 | Medium |
| Total score (9 items) | 39 | (33–45) | 52 | (47–55) | <0.001 | 0.62 | Large | |
| Age | Number of Medications | Explanation Provided by the Family Pharmacist a | |||||
|---|---|---|---|---|---|---|---|
| Patients’ Recognition of Pharmacists’ Behaviors Related to Information Sharing | Spearman’s Correlation Coefficient ρ | Spearman’s Correlation Coefficient ρ | Effect Size r | ||||
| 1 | Talk with patients about how to watch for medication side effects. | 0.00 | 0.04 | 0.15 | *** | ||
| 2 | Talk with patients even if the patients do not have any medication questions. | 0.04 | 0.04 | 0.18 | *** | ||
| 3 | Talk with patients about whether it is OK to take their medications with over-the-counter products. | −0.05 | 0.00 | 0.17 | *** | ||
| 4 | Show an interest in working with patients to meet their healthcare needs. | 0.11 | ** | 0.08 | 0.17 | *** | |
| 5 | Communicate a desire to help patients manage their medications. | 0.07 | 0.10 | * | 0.20 | *** | |
| 6 | Make sure that patients understand how to use their medications before they leave the pharmacy. | 0.01 | 0.00 | 0.20 | *** | ||
| 7 | Communicate a desire to help patients with their medication concerns. | 0.05 | 0.07 | 0.16 | *** | ||
| 8 | Listen to patients when they have a medication question. | 0.09 | * | 0.09 | * | 0.21 | *** |
| 9 | Be easily approachable to discuss a patient’s medication concerns. | 0.08 | 0.11 | ** | 0.20 | *** | |
| Total score (9 items) | 0.06 | 0.08 | 0.22 | *** | |||
| Years of Experience | Having One or More Certifications a | ||||
|---|---|---|---|---|---|
| Pharmacists’ Recognition of Pharmacists’ Behaviors Related to Information Sharing | Spearman’s Correlation Coefficient ρ | Effect Size r | |||
| 1 | Talk with patients about how to watch for medication side effects. | −0.03 | 0.08 | ||
| 2 | Talk with patients even if the patients do not have any medication questions. | 0.00 | 0.03 | ||
| 3 | Talk with patients about whether it is OK to take their medications with over-the-counter products. | −0.03 | 0.10 | * | |
| 4 | Show an interest in working with patients to meet their healthcare needs. | −0.07 | 0.04 | ||
| 5 | Communicate a desire to help patients manage their medications. | −0.05 | 0.08 | ||
| 6 | Make sure that patients understand how to use their medications before they leave the pharmacy. | −0.01 | 0.03 | ||
| 7 | Communicate a desire to help patients with their medication concerns. | −0.09 | * | 0.04 | |
| 8 | Listen to patients when they have a medication question. | −0.07 | 0.05 | ||
| 9 | Be easily approachable to discuss a patient’s medication concerns. | 0.00 | 0.04 | ||
| Total score (9 items) | −0.05 | 0.07 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumaki, R.; Kiyozuka, C.; Naganuma, M.; Yuge, S.; Tsukioka, R.; Sakurai, H.; Kishimoto, K. Recognition of Community Pharmacists’ Behaviors Related to Information Sharing: A Cross-Sectional Study. Pharmacy 2024, 12, 63. https://doi.org/10.3390/pharmacy12020063
Kumaki R, Kiyozuka C, Naganuma M, Yuge S, Tsukioka R, Sakurai H, Kishimoto K. Recognition of Community Pharmacists’ Behaviors Related to Information Sharing: A Cross-Sectional Study. Pharmacy. 2024; 12(2):63. https://doi.org/10.3390/pharmacy12020063
Chicago/Turabian StyleKumaki, Ryota, Chika Kiyozuka, Mika Naganuma, Satoshi Yuge, Ryota Tsukioka, Hidehiko Sakurai, and Keiko Kishimoto. 2024. "Recognition of Community Pharmacists’ Behaviors Related to Information Sharing: A Cross-Sectional Study" Pharmacy 12, no. 2: 63. https://doi.org/10.3390/pharmacy12020063