
Redesigning Medication Management in the Emergency Department: The Impact of Partnered Pharmacist Medication Charting on the Time to Administer Pre-Admission Time-Critical Medicines, Medication Order Completeness, and Venous Thromboembolism Risk Assessment

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
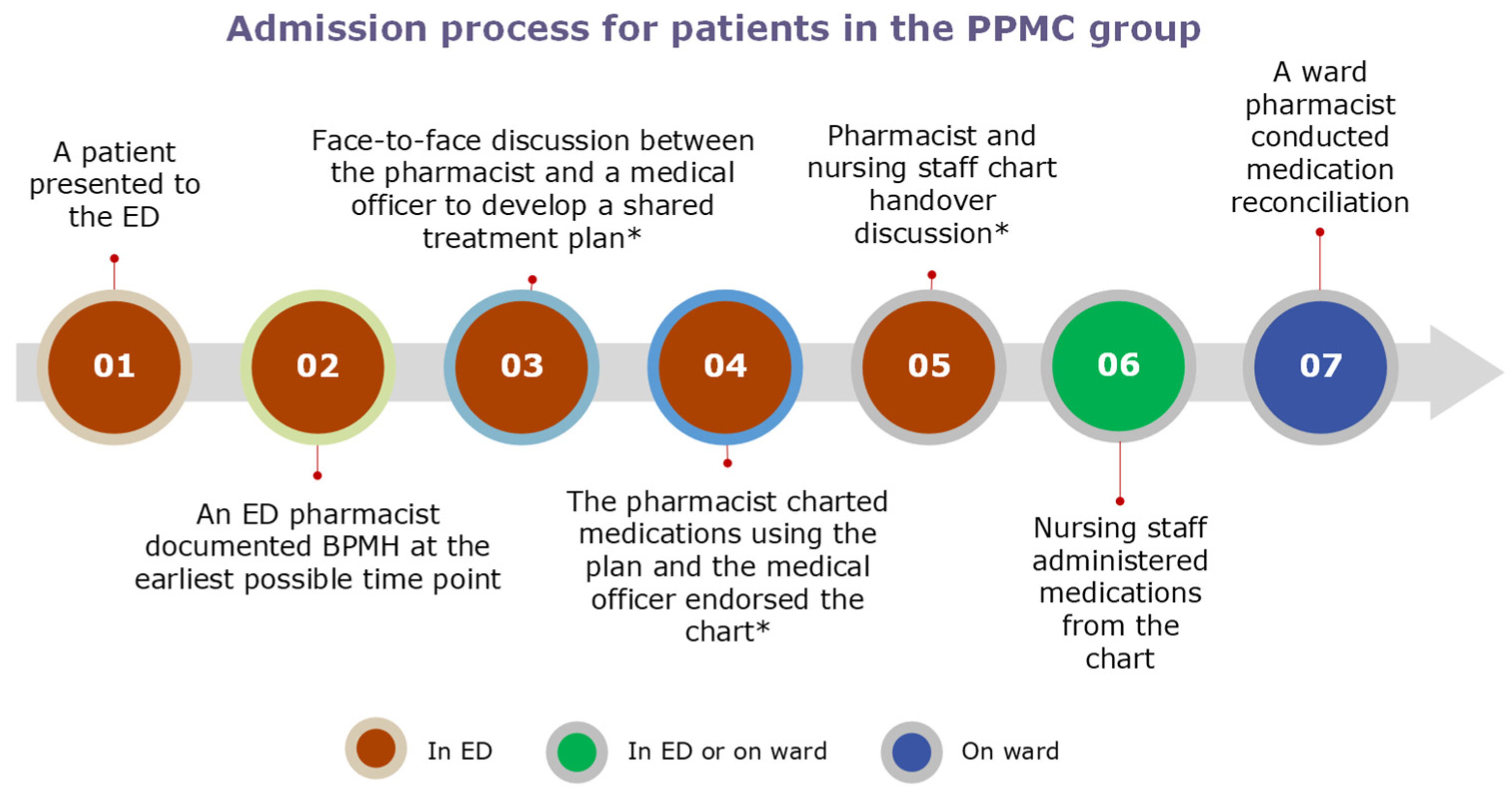
2.2. Study Arms
2.3. Ethics and Site Authorisation Approvals
2.4. Data Collection
2.5. Outcome Measures
2.5.1. Time to Time-Critical Medicines
2.5.2. Completeness of Medication Orders
- Incomplete order: A dose and/or frequency was omitted in the medication order. An example of a pharmacy note: “Currently charted hydrochlorothiazide 12.5 mg with no frequency. Please add frequency to order”.
- Unclear order: An order was illegible or edited to the original order. Example: “Quetiapine: currently an illegible order (150 mg? 250 mg). Please re-chart it”.
- Unsigned order: An order was not signed by a prescriber. Pharmacy note: “Requires doctor’s signature for oxycodone 5 mg (Endone)”.
2.5.3. VTE Risk Assessment
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
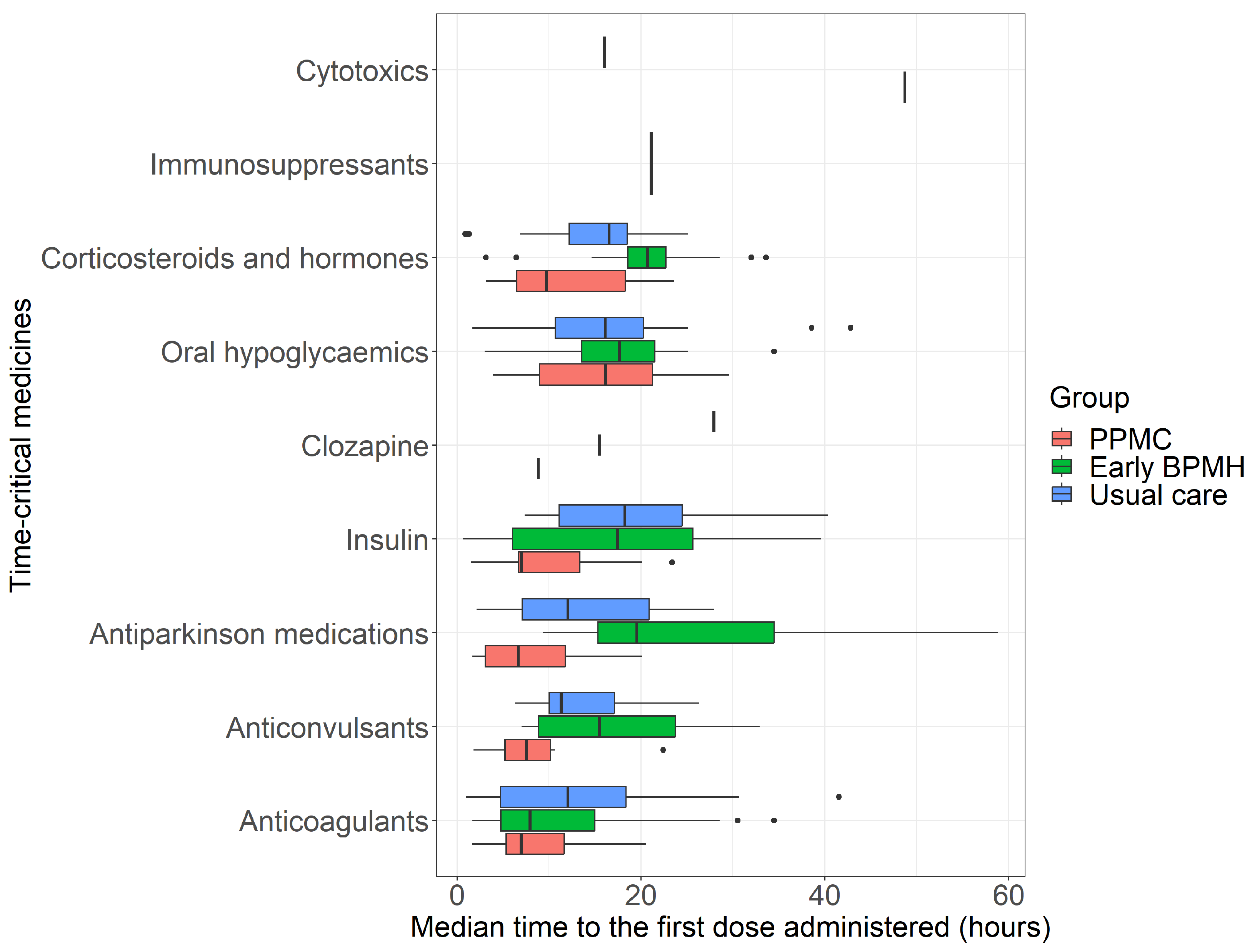
3.2. Time to Time-Critical Medicines
3.3. Completeness of Medication Orders
3.4. Venous Thromboembolism Risk Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meurer, W.J.; Potti, T.A.; Kerber, K.A.; Sasson, C.; Macy, M.L.; West, B.T.; Losman, E.D. Potentially inappropriate medication utilization in the emergency department visits by older adults: Analysis from a nationally representative sample. Acad. Emerg. Med. 2010, 17, 231–237. [Google Scholar] [CrossRef]
- Pines, J.M.; Mullins, P.M.; Cooper, J.K.; Feng, L.B.; Roth, K.E. National trends in emergency department use, care patterns, and quality of care of older adults in the United States. J. Am. Geriatr. Soc. 2013, 61, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Kennebeck, S.S.; Timm, N.L.; Kurowski, E.M.; Byczkowski, T.L.; Reeves, S.D. The association of emergency department crowding and time to antibiotics in febrile neonates. Acad. Emerg. Med. 2011, 18, 1380–1385. [Google Scholar] [CrossRef] [PubMed]
- Morley, C.; Unwin, M.; Peterson, G.M.; Stankovich, J.; Kinsman, L. Emergency department crowding: A systematic review of causes, consequences and solutions. PLoS ONE 2018, 13, e0203316. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, S.L.; Aronsky, D.; Duseja, R.; Epstein, S.; Handel, D.; Hwang, U.; McCarthy, M.; John McConnell, K.; Pines, J.M.; Rathlev, N.; et al. The effect of emergency department crowding on clinically oriented outcomes. Acad. Emerg. Med. 2009, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gregory, H.; Cantley, M.; Calhoun, C.; Hall, G.A.; Matuskowitz, A.J.; Weant, K.A. Incidence of prescription errors in patients discharged from the emergency department. Am. J. Emerg. Med. 2021, 46, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Hale, A.; Lewis, R.; Rowland, J. Collaborative doctor–pharmacist prescribing in the emergency department and admissions unit: A study of accuracy and safety. J. Pharm. Pract. Res. 2019, 49, 176–178. [Google Scholar] [CrossRef]
- Levine, R.L.; Hergenroeder, G.W.; Miller, C.C., III; Davies, A. Venous thromboembolism prophylaxis in emergency department admissions. J. Hosp. Med. 2007, 2, 79–85. [Google Scholar] [CrossRef]
- Tong, E.Y.; Roman, C.P.; Smit, D.V.; Newnham, H.; Galbraith, K.; Dooley, M.J. Partnered medication review and charting between the pharmacist and medical officer in the Emergency Short Stay and General Medicine Unit. Aust. Emerg. Nurs. J. 2015, 18, 149–155. [Google Scholar] [CrossRef]
- Vasileff, H.M.; Whitten, L.E.; Pink, J.A.; Goldsworthy, S.J.; Angley, M.T. The effect on medication errors of pharmacists charting medication in an emergency department. Pharm. World Sci. 2009, 31, 373–379. [Google Scholar] [CrossRef]
- Atey, T.M.; Peterson, G.M.; Salahudeen, M.S.; Bereznicki, L.R.; Simpson, T.; Boland, C.M.; Anderson, E.; Burgess, J.R.; Huckerby, E.J.; Tran, V.; et al. Impact of Partnered Pharmacist Medication Charting (PPMC) on Medication Discrepancies and Errors: A Pragmatic Evaluation of an Emergency Department-Based Process Redesign. Int. J. Environ. Res. Public Health 2023, 20, 1452. [Google Scholar] [CrossRef] [PubMed]
- Tong, E.Y.; Roman, C.; Mitra, B.; Yip, G.; Gibbs, H.; Newnham, H.; Smit, D.P.; Galbraith, K.; Dooley, M.J. Partnered pharmacist charting on admission in the General Medical and Emergency Short-stay Unit—A cluster-randomised controlled trial in patients with complex medication regimens. J. Clin. Pharm. Ther. 2016, 41, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Atey, T.M.; Peterson, G.M.; Salahudeen, M.S.; Wimmer, B.C. The impact of partnered pharmacist medication charting in the emergency department on the use of potentially inappropriate medications in older people. Front. Pharmacol. 2023, 14, 1273655. [Google Scholar] [CrossRef] [PubMed]
- Atey, T.M.; Peterson, G.M.; Salahudeen, M.S.; Simpson, T.; Boland, C.M.; Anderson, E.; Wimmer, B.C. Clinical and economic impact of partnered pharmacist medication charting in the emergency department. Front. Pharmacol. 2023, 14, 1273657. [Google Scholar] [CrossRef] [PubMed]
- Government of Western Australia Department of Health. Guiding Principles for Timely Administration of Medications; Government of Western Australia Department of Health: East Perth, WA, Australia, 2020. [Google Scholar]
- Department of Health and Human Services Royal Hobart Hospital. Available online: https://www.dhhs.tas.gov.au/hospital/royal-hobart-hospital (accessed on 13 September 2022).
- Ogrinc, G.; Davies, L.; Goodman, D.; Batalden, P.; Davidoff, F.; Stevens, D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised publication guidelines from a detailed consensus process. BMJ Qual. Saf. 2016, 25, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Gosser, R.A.; Arndt, R.F.; Schaafsma, K.; Dang, C.H. Pharmacist impact on ischemic stroke care in the emergency department. J. Emerg. Med. 2016, 50, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Robey-Gavin, E.; Abuakar, L. Impact of clinical pharmacists on initiation of postintubation analgesia in the emergency department. J. Emerg. Med. 2016, 50, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Gawedzki, P.; Celmins, L.; Fischer, D. Pharmacist involvement with antiepileptic therapy for status epilepticus in the emergency department. Acad. Emerg. Med. 2021, 28 (Suppl. 1), 129–132. [Google Scholar] [CrossRef] [PubMed]
- Society of Hospital Pharmacists of Australia. Which Medicines Are “Time-Critical”? Available online: https://onlinecpd.shpa.org.au/pluginfile.php/34951/mod_resource/content/2/2020_1%20Time%20critical%20meds.pdf (accessed on 20 January 2022).
- Australian Commission on Safety and Quality in Health Care. National Inpatient Medication Chart User Guide. Available online: https://www.safetyandquality.gov.au/sites/default/files/2019-08/nimc_user_guide_2019.pdf (accessed on 12 March 2022).
- Australian Commission on Safety and Quality in Health Care. National Standard Medication Chart (NSMC) Audit. Available online: https://www.safetyandquality.gov.au/sites/default/files/2019-05/national-standard-medication-chart-audit-form-v1.0.pdf (accessed on 10 October 2019).
- Khalil, V.; deClifford, J.M.; Lam, S.; Subramaniam, A. Implementation and evaluation of a collaborative clinical pharmacist’s medications reconciliation and charting service for admitted medical inpatients in a metropolitan hospital. J. Clin. Pharm. Ther. 2016, 41, 662–666. [Google Scholar] [CrossRef]
- Clinical Excellence Commission. Safer Systems Better Care—Quality Systems Assessment Statewide Report; Clinical Excellence Commission: Sydney, NSW, Australia, 2013. [Google Scholar]
- Roberts, L.N.; Porter, G.; Barker, R.D.; Yorke, R.; Bonner, L.; Patel, R.K.; Arya, R. Comprehensive VTE prevention program incorporating mandatory risk assessment reduces the incidence of hospital-associated thrombosis. Chest 2013, 144, 1276–1281. [Google Scholar] [CrossRef]
- Heit, J.A.; Melton, L.J., III; Lohse, C.M.; Petterson, T.M.; Silverstein, M.D.; Mohr, D.N.; O’fallon, W.M. Incidence of Venous Thromboembolism in Hospitalized Patients vs Community Residents. Mayo Clin. Proc. 2001, 76, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Access Economics Pty Ltd. The Burden of Venous Thromboembolism in Australia; The Australia and New Zealand Working Party on the Management and Prevention of Venous Thromboembolism; Access Economics Pty Ltd.: Canberra, NSW, Australia, 2008. [Google Scholar]
- Ho, W.K.; Hankey, G.J.; Eikelboom, J.W. The incidence of venous thromboembolism: A prospective, community-based study in Perth, Western Australia. Med. J. Aust. 2008, 189, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Szabo, F.; Marshall, C.; Huynh, D.K. Venous thromboembolism in tropical Australia and in Indigenous Australians. Semin. Thromb. Hemost. 2014, 40, 736–740. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Variables | Before Accounting for a Potential Clustering Effect | After Accounting for a Potential Clustering Effect | ||||||
|---|---|---|---|---|---|---|---|---|
| PPMC (n = 107 TCMs) | Early BPMH (n = 107 TCMs) | Usual Care (n = 107 TCMs) | p-Value | PPMC (n = 77 TCMs) | Early BPMH (n = 76 TCMs) | Usual Care (n = 91 TCMs) | p-Value | |
| Group, n (%) | ||||||||
| Anti-coagulants | 24 (22%) | 23 (21%) | 24 (22%) | 0.98 * | 16 (21%) | 21 (28%) | 22 (24%) | 0.61 * |
| Anti-convulsants | 9 (8.4%) | 9 (8.4%) | 8 (7.5%) | 0.96 * | 6 (7.8%) | 7 (9.2%) | 6 (6.6%) | 0.82 * |
| Anti-Parkinson’s medications | 9 (8.4%) | 9 (8.4%) | 10 (9.3%) | 0.96 * | 7 (9.1%) | 7 (9.2%) | 8 (8.8%) | 0.99 * |
| Clozapine | 1 (0.9%) | 1 (0.9%) | 1 (0.9%) | >0.99 † | 1 (1.3%) | 1 (1.3%) | 1 (1.1%) | >0.99 † |
| Corticosteroids and hormones | 14 (13%) | 19 (18%) | 16 (15%) | 0.63 * | 9 (12%) | 13 (17%) | 14 (15%) | 0.63 * |
| Cytotoxic drugs | 0 (0%) | 1 (0.9%) | 1 (0.9%) | >0.99 † | - | - | - | - |
| Immunosuppressants | 0 (0%) | 1 (0.9%) | 0 (0%) | >0.99 † | - | - | - | - |
| Insulin | 17 (16%) | 15 (14%) | 16 (15%) | 0.93 * | 15 (19%) | 11 (14%) | 13 (14%) | 0.60 * |
| Oral hypoglycaemic agents | 33 (31%) | 29 (27%) | 31 (29%) | 0.83 * | 23 (30%) | 16 (21%) | 27 (30%) | 0.37 * |
| Median time, hours (IQR) | 8.8 (6.3, 16.3) | 17.5 (7.8, 22.9) | 15.1 (8.2, 21.1) | <0.001 ‡,§ | 9.0 (6.3, 16.1) | 16.7 (7.1, 22.2) | 14.2 (7.3, 21.2) | 0.007 ‡,¶ |
| Variables, n (%) | Study Group | p-Value * | ||
|---|---|---|---|---|
| PPMC (n = 230 Patients) | Early BPMH (n = 230 Patients) | Usual Care (n = 588 Patients) | ||
| Total incomplete, unclear, and unsigned orders | 1 | 25 † | 62 † | <0.001 |
| Patients with at least one incomplete, unclear, or unsigned order | 1 (0.4%) | 17 (7.4%) | 45 (7.7%) | <0.001 |
| Patients with incomplete orders, n (%) | <0.001 | |||
| No incomplete order | 229 (100%) | 217 (94%) | 552 (94%) | |
| 1 incomplete order | 0 (0%) | 9 (3.9%) | 27 (4.6%) | |
| 2 incomplete orders | 0 (0%) | 2 (0.9%) | 7 (1.2%) | |
| 3 incomplete orders | 0 (0%) | 2 (0.9%) | 2 (0.3%) | |
| Patients with unclear orders, n (%) † | 0.20 | |||
| No unclear order | 230 (100%) | 227 (99%) | 577 (98%) | |
| 1 unclear order | 0 (0%) | 2 (0.9%) | 8 (1.4%) | |
| 2 unclear orders | 0 (0%) | 0 (0%) | 3 (0.5%) | |
| 3 unclear orders | 0 (0%) | 1 (0.4%) | 0 (0%) | |
| Patients with unsigned orders, n (%) | 0.41 | |||
| No unsigned order | 229 (99.6%) | 229 (99.6%) | 587 (99.8%) | |
| 1 unsigned order | 1 (0.4%) | 1 (0.4%) | 1 (0.2%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atey, T.M.; Peterson, G.M.; Salahudeen, M.S.; Simpson, T.; Boland, C.M.; Anderson, E.; Wimmer, B.C. Redesigning Medication Management in the Emergency Department: The Impact of Partnered Pharmacist Medication Charting on the Time to Administer Pre-Admission Time-Critical Medicines, Medication Order Completeness, and Venous Thromboembolism Risk Assessment. Pharmacy 2024, 12, 71. https://doi.org/10.3390/pharmacy12020071
Atey TM, Peterson GM, Salahudeen MS, Simpson T, Boland CM, Anderson E, Wimmer BC. Redesigning Medication Management in the Emergency Department: The Impact of Partnered Pharmacist Medication Charting on the Time to Administer Pre-Admission Time-Critical Medicines, Medication Order Completeness, and Venous Thromboembolism Risk Assessment. Pharmacy. 2024; 12(2):71. https://doi.org/10.3390/pharmacy12020071
Chicago/Turabian StyleAtey, Tesfay Mehari, Gregory M. Peterson, Mohammed S. Salahudeen, Tom Simpson, Camille M. Boland, Ed Anderson, and Barbara C. Wimmer. 2024. "Redesigning Medication Management in the Emergency Department: The Impact of Partnered Pharmacist Medication Charting on the Time to Administer Pre-Admission Time-Critical Medicines, Medication Order Completeness, and Venous Thromboembolism Risk Assessment" Pharmacy 12, no. 2: 71. https://doi.org/10.3390/pharmacy12020071