
Insights from a National Survey on Controlled Substance Diversion Practices in U.S. Hospital Pharmacies: Opportunities for Enhanced Surveillance and Compliance

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics
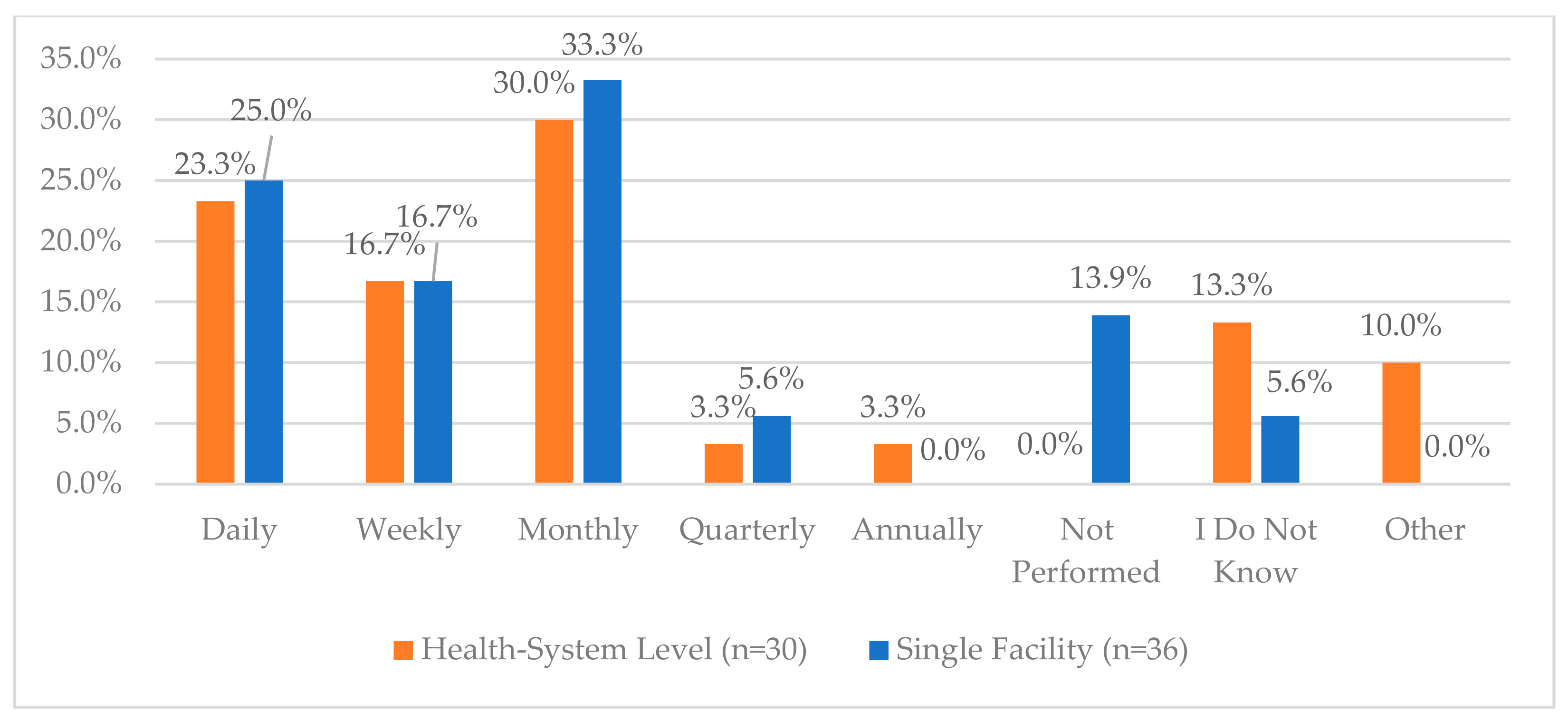
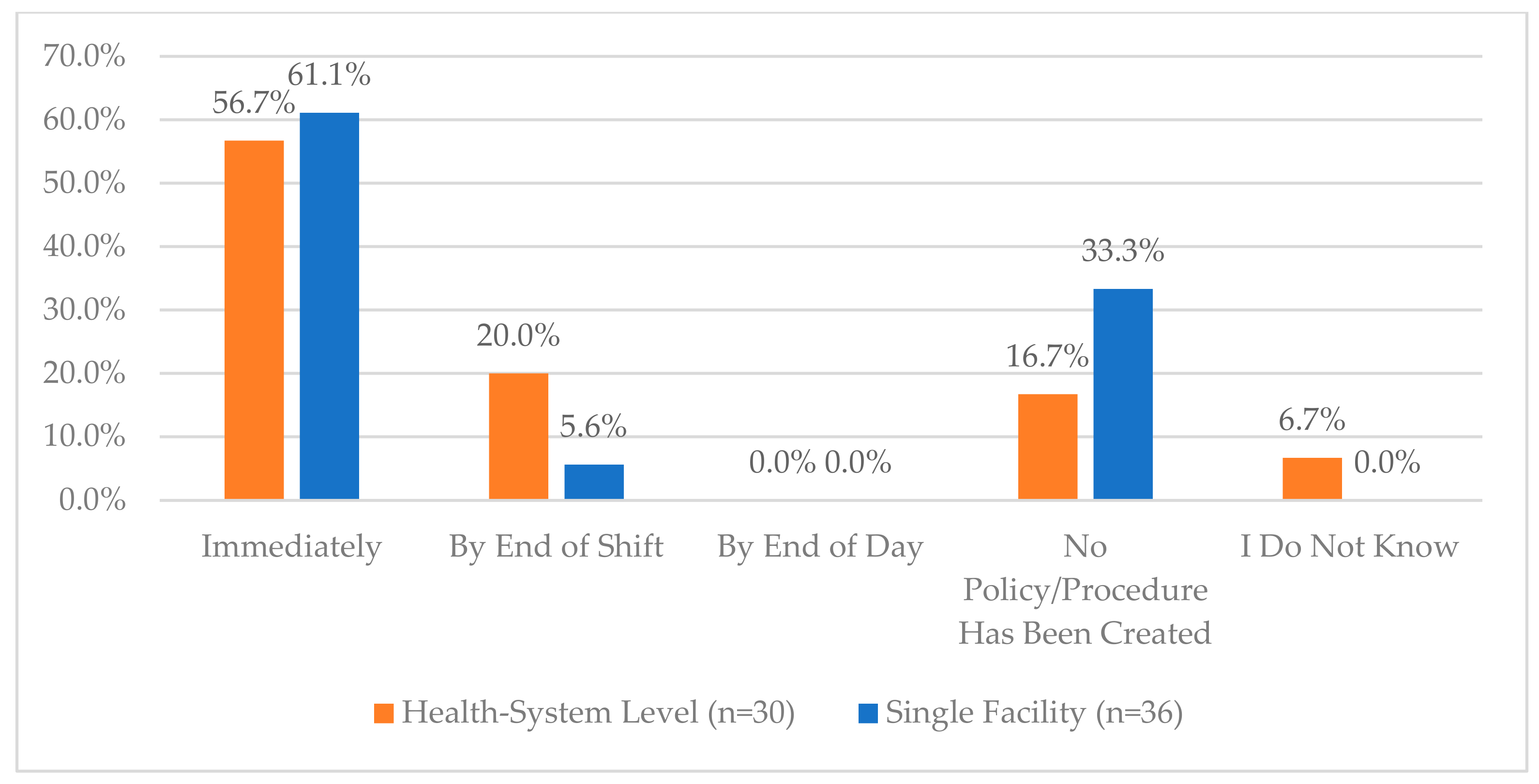
3.2. Controlled Substance Procurement and Receiving
3.3. Controlled Substance Storage, Packaging and Compounding
3.4. Controlled Substance Dispensing
3.5. Controlled Substance Waste, Return and Disposal
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Survey Questions
- Which most closely matches your role (select more than one if necessary):
- ▯
- Staff/operations pharmacist
- ▯
- Clinical pharmacist
- ▯
- Pharmacy manager/supervisor
- ▯
- Director of Pharmacy
- ▯
- CPO/VP of Pharmacy
- ▯
- Drug Diversion Team Member
- ▯
- Drug Diversion Lead/Director
- ▯
- Safety, Quality, or Compliance Officer
- ▯
- Pharmacy Informaticist/Analyst
- ▯
- Other:
- Do you perform any drug diversion surveillance activities as part of your role?
- ▯
- Yes
- ▯
- No
- In which state do you primarily work?
- Does your specific drug diversion surveillance role cover one facility or a system of facilities?
- ▯
- System of facilities (e.g., IDN, system level role)
- ▯
- Single facility
- Which most closely matches your facility type:
- ▯
- Academic medical center
- ▯
- Community hospital
- ▯
- Government hospital
- ▯
- Long-term care facility
- ▯
- Retail pharmacy
- ▯
- Industry pharmacy
- ▯
- Ambulatory care pharmacy
- ▯
- Other:
- What is your hospital bed size?
- ▯
- <150
- ▯
- 150–300
- ▯
- 300–500
- ▯
- 500
- Procurement
- Do you actively work with your wholesaler to validate controlled substance orders? (CS)
- Do you assess the appropriateness of CS order quantity based on demand (e.g., medication orders and use)?
- Do you assess for significant changes in ordering patterns of CS over time, including changes in quantity or frequency?
- Does your organization have a process for routinely monitoring the effectiveness of PAR levels of CS medications and modifying PARs to meet demand fluctuations?
- Does your organization provide a unique login for each user who can create purchase orders?
- Does your organization have a policy to purchase unit doses (instead of bulk) of controlled substances when available?
- ▯
- Pharmacy Buyer
- ▯
- Pharmacist Manager
- ▯
- Pharmacist Non-Manager
- ▯
- Pharmacy Technician Manager
- ▯
- Pharmacy Technician Non-Manager
- ▯
- Other
- Receiving
- Does your controlled substances ordering and receiving process ensure consistent segregation of duties (e.g., separate team members performing ordering and receiving functions)?
- Do you have a process for auditing your segregation of duties (person ordering against the person receiving)?
- ▯
- Not performed
- ▯
- Daily
- ▯
- Not performed
- ▯
- Daily
- ▯
- Weekly
- ▯
- Monthly
- ▯
- Quarterly
- ▯
- Annually
- ▯
- I do not know
- ▯
- Other (add frequency below)
- ▯
- Not performed
- ▯
- Daily
- ▯
- Weekly
- ▯
- Monthly
- ▯
- Quarterly
- ▯
- Annually
- ▯
- I do not know
- ▯
- Other (add frequency below)
- ▯
- No policy
- ▯
- Immediately
- ▯
- End of shift
- ▯
- End of day
- ▯
- I do not know
- ▯
- Other (add frequency below)
- ▯
- 100%
- ▯
- 75–99%
- ▯
- 50–74%
- ▯
- 25–49%
- ▯
- <25%
- ▯
- I do not know
- ▯
- Other (add frequency below)
- Storage
- ▯
- Yes
- ▯
- No
- ▯
- I do not know
- ▯
- Ordering
- ▯
- Receiving
- ▯
- Storage
- ▯
- Packaging
- ▯
- Compounding
- ▯
- Dispensing
- ▯
- Returning
- ▯
- Wasting
- ▯
- Not Performed
- ▯
- Daily
- ▯
- Weekly
- ▯
- Monthly
- ▯
- Quarterly
- ▯
- Annually
- ▯
- I do not know
- ▯
- Other (enter frequency below)
- ▯
- Yes
- ▯
- No
- ▯
- I do not know
- ▯
- Yes
- ▯
- No
- ▯
- I do not know
- ▯
- CII
- ▯
- CIII
- ▯
- CIV
- ▯
- CV
- ▯
- None of the above
- ▯
- CII
- ▯
- CIII
- ▯
- CIV
- ▯
- CV
- ▯
- None of the above
- ▯
- Yes, vials only
- ▯
- Yes, bulk bottles only
- ▯
- Yes, vials and bulk bottles
- ▯
- No
- ▯
- I do not know
- ▯
- Not Performed
- ▯
- Daily
- ▯
- Weekly
- ▯
- Monthly
- ▯
- Quarterly
- ▯
- Annually
- ▯
- For cause only
- ▯
- I do not know
- ▯
- Other (enter frequency below)
- Does your organization use secure caps or other tamper-evident packaging for compounded controlled substances (CS)?
- Does your CS storage (e.g., vault or cabinet) allow for ongoing (perpetual) electronic inventory monitoring?
- Does your facility control access to the CS areas by work schedule?
- Does your organization serialize prescription pads to prevent unauthorized duplication or misuse?
- Is the process for prescription pad management audited?
- Packaging/Compounding
- Does your organization have a process for addressing broken or crushed tablets of controlled substance (CS) medications that may occur during the repackaging process?
- Does your organization have an audit process for multi-dose and bulk CS transactions to account for each milligram (or unit)?
- ▯
- No policy/procedure has been created
- ▯
- Immediately
- ▯
- By end of shift
- ▯
- By end of day
- ▯
- Other
- ▯
- I do not know
- ▯
- Yes, vials only
- ▯
- Yes, Bulk bottles only
- ▯
- Yes, for vials and bulk bottles
- ▯
- No
- ▯
- I do not know
- Dispensing
- Are prepared controlled substance (CS) medications ever unobserved and accessible prior to delivery to the patient care units?
- Does your facility have a process for auditing how often the amounts (quantity of units) programmed in the cabinet are less than or greater than the suggested PAR for CS?
- Does a second tech or pharmacist verify CS medications removed from the vault against printed receipts?
- Does your organization require witness verification for stocking of controlled substance (CS) medications at the ADC?
- Are CS medications that are delivered outside of the ADC signed for by the deliverer and the receiver? (or code-locked in a tube system)
- Are CS restricted from being placed in matrix-style drawers in the ADC?
- ▯
- Not performed
- ▯
- Immediately
- ▯
- End of shift
- ▯
- End of week
- ▯
- I do not know
- ▯
- Other
- Waste, Return, Disposal
- Does your organization have a process to ensure returned controlled substance (CS) medications are inspected for tampering prior to returning to circulation for potential use?
- Does your organization have training on signs of product tampering as part of the annual training for individuals?
- Do all areas across your organization where CS are located have secured waste receptacles (including pharmacy department space)?
- Are the keys to CS waste containers accessible to only restricted personnel?
- Does your organization have a process for auditing controlled substance (CS) orders discontinued for a patient and corresponding return to the controlled substance vault?
- Does your facility have a process to verify that all CS medications that are expired from the ADCs and vault are indeed expired and placed in the appropriate waste/reverse distributor bin?
- Does your facility require the CS medications returned to the pharmacy to have witness verification and signature?
- Does your facility require that CS medications wasted or added to the reverse distributor bin in the pharmacy have witness verification and signature?
- Does your facility inventory the CS medications to be sent for disposal and reconcile with the reports from the reverse distributor?
- ▯
- No, for cause only
- ▯
- Yes, for 100% of controlled substance waste
- ▯
- Yes, for 75–99% of controlled substance waste
- ▯
- Yes, for 50–74% of controlled substance waste
- ▯
- Yes, for 25–49% of controlled substance waste
- ▯
- Yes, for <25% of controlled substance waste
- ▯
- Other
- ▯
- I do not know
- ▯
- Weekly
- ▯
- Bi-weekly
- ▯
- Monthly
- ▯
- Quarterly
- ▯
- As needed
- ▯
- Other
- ▯
- I do not know
- ▯
- Weekly
- ▯
- Bi-weekly
- ▯
- Monthly
- ▯
- Quarterly
- ▯
- As needed
- ▯
- Other
- ▯
- I do not know
- Resources
- Does your facility have a dedicated drug diversion surveillance team?
- Does your facility utilize drug diversion software?
- ▯
- Once
- ▯
- Quarterly
- ▯
- Annually
- ▯
- Other
- ▯
- I do not know
- ▯
- No training
References
- Berge, K.H.; Dillon, K.R.; Sikkink, K.M.; Taylor, T.K.; Lanier, W.L. Diversion of drugs within health care facilities, a multiple-victim crime: Patterns of diversion, scope, consequences, detection, and prevention. Mayo Clin. Proc. 2012, 87, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Draime, J.A.; Anderson, D.C.; Anderson, T.S. Description and comparison of medication diversion in pharmacies by pharmacists, interns, and pharmacy technicians. J. Am. Pharm. Assoc. 2018, 58, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.; Fera, T.; Fortier, C.; Gullickson, K.; Hays, A.; Murdaugh, L.; Ogden, R.; O’Neal, B.; Rush, J.; Vest, T. ASHP Guidelines on Preventing Diversion of Controlled Substances. Am. J. Health-Syst. Pharm. 2022, 79, 2279–2306. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Justice. Practitioner’s Manual: An Informational Outline of the Controlled Substances Act. 2023. Available online: https://www.deadiversion.usdoj.gov/GDP/(DEA-DC-071)(EO-DEA226)_Practitioner's_Manual_(final).pdf (accessed on 19 September 2024).
- Tortorici, A.; Turner, B. Investigate and manage suspected drug diversion. Pharm. Purch. Prod. 2011, 8, 12–15. [Google Scholar]
- McLaren Health and Feds Reach Record $7.75M Settlement of Drug Allegations. The Detroit News. 19 January 2021. Available online: https://www.detroitnews.com/story/news/local/michigan/2021/01/19/mclaren-health-agrees-record-7-75-m-penalty-following-drug-probe/4219917001/ (accessed on 31 August 2024).
- Maki, D.G.; Klein, B.S.; McCormick, R.D.; Alvarado, C.J.; Zilz, M.A.; Stolz, S.M.; Hassemer, C.A.; Gould, J.; Liegel, A.R. Nosocomial Pseudomonas pickettii bacteremias traced to narcotic tampering. A case for selective drug screening of health care personnel. J. Am. Med. Assoc. 1991, 265, 981–986. [Google Scholar] [CrossRef]
- Bouffard. UM Pays $4.3M to Settle Federal Charges for Stolen Drugs, but Criminal Charges Possible. The Detroit News. 30 August 2018. Available online: https://www.detroitnews.com/story/news/local/michigan/2018/08/30/university-michigan-3-million-settle-federal-drug-diversion-lawsuit/1145373002/ (accessed on 31 August 2021).
- Anderson, T. General to Pay $2.3M over Drug Thefts. The Boston Globe. 28 September 2015. Available online: https://www.bostonglobe.com/metro/2015/09/28/mass-general-agrees-pay-million-settlement-federal-government-over-drug-thefts/NNgyVznhbmJnRuc3W2dYOK/story.html?p1=BGSearch_Overlay_Results (accessed on 16 October 2016).
- Brown, J. Hospital Tech Who Spread Hep C via Drug Thefts Gets 30 Years. The Denver Post. 6 May 2016. Available online: www.denverpost.com (accessed on 16 October 2016).
- Ostrowsky, B.E.; Whitener, C.; Bredenberg, H.K.; Carson, L.A.; Holt, S.; Hutwagner, L.; Arduino, M.J.; Jarvis, W.R. Serratia marcescens bacteremia traced to an infused narcotic. N. Engl. J. Med. 2002, 346, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, M.K.; Perz, J.F. Outbreaks of infections associated with drug diversion by US health care personnel. Mayo Clin. Proc. 2014, 89, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Njuguna, H.N.; Stinson, D.; Montgomery, P.; Turner, N.; D’angeli, M.; Carr, J.; Podczervinski, S.; Wasserman, C.; Ramachandran, S.; Lucas, T.; et al. Hepatitis C Virus Potentially Transmitted by Opioid Drug Diversion from a Nurse-Washington, August 2017–March 2018. Morb. Mortal. Wkly. Rep. 2019, 68, 374–376. [Google Scholar] [CrossRef] [PubMed]
- United States Attorney’s Office. Pikeville Medical Center to Pay $4.39 Million to Resolve Alleged Controlled Substance Act Violations That Allowed Drug Diversion. 7 December 2022. Available online: https://www.justice.gov/usao-edky/pr/pikeville-medical-center-pay-439-million-resolve-alleged-controlled-substance-act (accessed on 19 September 2024).
- United States Food and Drug Administration. Pharmacy Technician Pleads Guilty to Tampering with Hospital Pain Medication. 30 April 2024. Available online: https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/press-releases/pharmacy-technician-pleads-guilty-tampering-hospital-pain-medication (accessed on 19 September 2024).
- United States Food and Drug Administration. Sovah Health to Pay United States $4.36 Million to Settle Claims of Controlled Substance Act Violations. 8 June 2022. Available online: https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/press-releases/sovah-health-pay-united-states-436-million-settle-claims-controlled-substance-act-violations (accessed on 19 September 2024).
- United States Drug Enforcement Administration. Southern District of Georgia Announces Largest Hospital Drug Diversion Civil Penalty in U.S. History. 16 May 2018. Available online: https://www.dea.gov/press-releases/2018/05/16/southern-district-georgia-announces-largest-hospital-drug-diversion-civil (accessed on 19 September 2024).
- Fan, M.; Tscheng, D.; Hamilton, M.; Hyland, B.; Reding, R.; Trbovich, P. Diversion of Controlled Drugs in Hospitals: A Scoping Review of Contributors and Safeguards. J. Hosp. Med. 2019, 14, 419–428. [Google Scholar] [CrossRef] [PubMed]
- McClure, S.R.; O’Neal, B.C.; Grauer, D.; Couldry, R.J.; King, A.R. Compliance with recommendations for prevention and detection of controlled-substance diversion in hospitals. Am. J. Health-Syst. Pharm. 2011, 68, 689–694. [Google Scholar] [CrossRef] [PubMed]
- de Vries, M.; Fan, M.; Tscheng, D.; Hamilton, M.; Trbovich, P. Vulnerabilities for Drug Diversion in the Handling, Data Entry, and Verification Tasks of 2 Inpatient Hospital Pharmacies: Clinical Observations and Healthcare Failure Mode and Effect Analysis. J. Patient Saf. 2022, 18, e227–e235. [Google Scholar] [CrossRef] [PubMed]
- Definitive Healthcare. Hospital Search. Definitive Healthcare. October 2024. Available online: https://www.definitivehc.com/ (accessed on 14 October 2024).
- Schneider, P.J.; Pedersen, C.A.; Ganio, M.C.; Scheckelhoff, D.J. ASHP National Survey of Pharmacy Practice in Hospital Settings: Operations and Technology—2023. Am. J. Health-Syst. Pharm. 2024, 81, 684–705. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.A.; Schneider, P.J.; Ganio, M.C.; Scheckelhoff, D.J. ASHP National Survey of Pharmacy Practice in Hospital Settings: Workforce-2022. Am. J. Health-Syst. Pharm. 2023, 80, 719–741. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Respondent Demographics | Number | Percent |
|---|---|---|
| Number of Respondents | 66 | 100% |
| Role/Job Title (Select All Roles That Apply) | ||
| Staff/Operations Pharmacist | 1 | 1.5% |
| Clinical Pharmacist | 4 | 6.1% |
| Pharmacy Manager/Supervisor | 11 | 16.7% |
| Director of Pharmacy | 25 | 37.9% |
| Chief Pharmacy Officer/Vice President of Pharmacy | 2 | 3.0% |
| Drug Diversion Team Member | 7 | 10.6% |
| Drug Diversion Lead/Director | 19 | 28.8% |
| Safety, Quality, or Compliance Officer | 4 | 6.1% |
| Pharmacy Informaticist/Analyst | 4 | 6.1% |
| Geography (US Division) *^ | ||
| New England | 5 | 7.6% |
| Middle Atlantic | 4 | 6.1% |
| East North Central | 13 | 19.7% |
| West North Central | 6 | 9.1% |
| South Atlantic | 16 | 24.2% |
| East South Central | 4 | 6.1% |
| West South Central | 7 | 10.6% |
| Mountain | 3 | 4.5% |
| Pacific | 6 | 9.1% |
| Single Facility or IDN | ||
| Single Facility | 36 | 54.5% |
| System of Facilities | 30 | 45.5% |
| Type of Facility (If Single Facility, n = 36) | ||
| Academic Medical Center | 6 | 16.7% |
| Community Hospital | 26 | 39.4% |
| Government Hospital | 2 | 5.6% |
| Long-Term Care Facility | 1 | 2.8% |
| Surgical Hospital | 1 | 2.8% |
| Bed Size (If Single Facility, n = 36) | ||
| <150 | 18 | 50.0% |
| 150–300 | 9 | 25.0% |
| 301–500 | 8 | 22.2% |
| >500 | 1 | 2.8% |
| Diversion System | ||
| Facility(ies) Utilizes Drug Diversion Software | 47 | 71.2% |
| Facility(ies) Have a Dedicated Drug Diversion Surveillance Team | 47 | 71.2% |
| Responses | Health-System Level (n = 30) | Single Facility (n = 36) |
|---|---|---|
| Pharmacy Buyer | 15 (50.0%) | 20 (55.6%) |
| Pharmacist Manager | 26 (86.7%) | 29 (80.6%) |
| Pharmacist Non-Manager | 12 (40.0%) | 12 (33.3%) |
| Pharmacist Director | 0 (0.0%) | 4 (11.1%) |
| Pharmacy Technician Manager | 2 (6.7%) | 2 (5.6%) |
| Pharmacy Technician Non-Manager | 5 (16.7%) | 1 (2.8%) |
| Other | 0 (0.0%) | 1 (2.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bastow, S.S.; Borrelli, E.P.; Lucaci, J.D.; Nelkin, H.; Graves, A.; Hays, A. Insights from a National Survey on Controlled Substance Diversion Practices in U.S. Hospital Pharmacies: Opportunities for Enhanced Surveillance and Compliance. Pharmacy 2024, 12, 183. https://doi.org/10.3390/pharmacy12060183
Bastow SS, Borrelli EP, Lucaci JD, Nelkin H, Graves A, Hays A. Insights from a National Survey on Controlled Substance Diversion Practices in U.S. Hospital Pharmacies: Opportunities for Enhanced Surveillance and Compliance. Pharmacy. 2024; 12(6):183. https://doi.org/10.3390/pharmacy12060183
Chicago/Turabian StyleBastow, Samantha S., Eric P. Borrelli, Julia D. Lucaci, Heather Nelkin, April Graves, and Amanda Hays. 2024. "Insights from a National Survey on Controlled Substance Diversion Practices in U.S. Hospital Pharmacies: Opportunities for Enhanced Surveillance and Compliance" Pharmacy 12, no. 6: 183. https://doi.org/10.3390/pharmacy12060183
APA StyleBastow, S. S., Borrelli, E. P., Lucaci, J. D., Nelkin, H., Graves, A., & Hays, A. (2024). Insights from a National Survey on Controlled Substance Diversion Practices in U.S. Hospital Pharmacies: Opportunities for Enhanced Surveillance and Compliance. Pharmacy, 12(6), 183. https://doi.org/10.3390/pharmacy12060183