Appendix A. Survey 1 Questions
Dear Pharmacist,
The Pharmacy Board now requires registered pharmacists to acquire annual Continuing Professional Development (CPD) credits for renewal of registration. This online survey will aim to investigate what registered pharmacists understand about mandatory CPD by asking how you are managing to complete your annual CPD credits.
It would be appreciated and of considerable value if you could spend approximately 10 min completing this survey. Please note that the Pharmacy Board of Australia has provided the link to the survey to you on behalf of the UQ research team and names or contact details of participants will not be disclosed to the research team.
Participation in the survey is voluntary, but completing a survey will allow entry into a prize draw, which provides an opportunity to win a $50 Myers gift voucher.
If you would like to participate, then read the attached participant information leaflet (see the link at the end of question 1).This provides a more detailed explanation of what the study involves.
Participation in the survey will contribute to understanding how pharmacists are dealing with the introduction of mandatory CPD, and the resulting data may identify if further assistance or modifications could improve the process.
Thank you for considering this request.
Note: Continuing Professional Development will be referred to as CPD.
1. Before starting this survey, please can you confirm that you have read and understood the participant information leaflet and that you consent to participate in this survey? Click here for participant information.
Yes, I have read the participant information and I agree to participate.
No, I do not wish to participate.
To help us put your answers into context, please can you answer the following questions before you start the survey on CPD?
2. Approximately how long have you been on the register of pharmacists in Australia (after your intern year)?
0–5 years
6–10 years
more than 10 years
3. What is your gender?
4. Please indicate your age bracket.
20–24 years
25–29 years
30–34 years
35–39 years
40–44 years
45–49 years
50–54 years
55–59 years
60–64 years
65 years or above
5. What is your main area of practice?
Hospital
Community
Academia
Not practising
Consultants/accredited
Other (please specify)
This page is just for practising Pharmacists.
6. Approximately how many hours per week do you work as a pharmacist?
The questions on this page ask how you found out about mandatory CPD and investigate how well you understand the process.
7. Please show your level of agreement with the following statements. KEY: SA = Strongly Agree, A = Agree, N = Neutral, D = Disagree, SD = Strongly Disagree.
8. Which source has provided the most information about the CPD requirements?
Pharmacy Board of Australia
Pharmaceutical Society of Australia
Society of Hospital Pharmacists
Pharmacy Guild
Other (please specify)
The questions on this page will explore in more detail what you understand about the CPD process and ask which type of CPD you prefer.
9. The Pharmacy Board has classified CPD activities into three groups and each group acquires a different number of CPD credits. Do you understand how these groups are classified?
10. Do these groups influence which CPD activities you will do?
11. Not more than 50% of the annual CPD credits required for renewal of registration can be claimed by undertaking Group 1 CPD activities. Should Group 1 activities be limited?
12. If you have answered yes to the previous question, please indicate what you believe the limitation should be.
less than 50%
more than 50%
equal to 50%
13. For the following list of CPD activities, please give them a numerical rating between 1 and 5; with 1 indicating MOST preferred and 5 the LEAST preferred.
Attend a lecture.
Give a conference presentation.
Complete an online interactive case study.
Publish an article in a journal.
Read a journal article.
Complete a postgraduate education course.
View an online lecture.
Join the board of a local pharmacy committee.
Read an online journal and complete the MCQ assessment.
Attend an interactive workshop.
Introduce a new professional service into your pharmacy.
View an online interactive lecture.
14. Do you know how to undertake selfdirected learning as part of a structured learning plan?
15. Are you using self-directed structured learning plans to guide your CPD activities?
Always
Often
Sometimes
Never
16. Did you use self-directed structured learning plans before national mandatory CPD was introduced?
Always
Often
Sometimes
Never
17. Are you recording CPD activities in the correct format required for audit?
18. Continuing professional development can also be known as continuing education.
The last few questions on this page investigate how you acquire CPD credits.
19. Please show your level of agreement with the following statements. KEY: SA = Strongly Agree, A = Agree, N = Neutral, D = Disagree, SD = Strongly Disagree
Since CPD became mandatory, I have increased my number of annual CPD activities.
Since CPD became mandatory, I have participated in a wider variety of CPD activities.
It will be difficult for me to acquire 40 CPD credits annually.
20. Which of the following make it difficult for you to acquire CPD credits? Tick more than one box if required.
21. Describe the main difficulty (if any) to obtaining your annual CPD credits.
22. Why is this challenging for you?
23. What has helped you to acquire your annual CPD credits?
24. Are you a member of a professional organisation?
25. If you answered ‘yes’ to the previous question, please state which professional organisation(s) you are a member of.
This now ends the survey on CPD. Thank you for participating.
If you would like to be entered into the prize draw then answer ‘Yes’ to the next question, otherwise answer ‘No’ to finish the survey.
26. Would you like to be entered into our prize draw? Two participants will be selected to win a $50 Coles/Myer voucher?
Please enter your e-mail address in the text box and we will contact you if you are selected in the draw.
27. Please note that your e-mail address will be used for the purpose of this draw only and it will be deleted immediately after the winners are selected.
Appendix C. Social Media Comments
Probably because it is a useless process that has been poorly outlined and explained by the Pharmacy Board. PSA has a CPD planning tool which is laborious and unhelpful. Yet they tell us if we don’t use it, we’re probably doing it wrong.
Surely we all do CPD that is relevant to our practice, or to practice that we’re interested in moving into. Why would we waste our time doing anything else?
We have no time and no motivation for CPD plans, especially since it is all for a pay-packet that we could get at the local supermarket.
For soooo many to not understand means it hasn’t been explained very well at all!!!!
The Guild’s MYCPD is still developing a tool so that’s part of my reasoning of not having a plan as yet .... not going to do the process twice, don’t have the time and don’t get paid for it .... hard enough to make a buck as it is!!
That’s because it is nonsense. I refuse to write a plan and will continue to study and read what takes my fancy or I feel needs refreshing. It’s [a] fluid thing—i.e., meet [a] patient with a certain condition and research it.
Attend a conference that takes my fancy. Do a post graduate uni course that presents itself. It’s not planned but adjusted to need in an environment of continual learning. Whoever comes up with this crap needs a life and to stop finding more crap for us to do instead of helping patients.
I mean who seriously has the time to sit down and plan their CPD footprint for the next 12 months. Get a life people. I’ll take the fine any day. It’s not like my $25/hr job is that great anyway. Worse comes to worse I’ll just get a job at Bing Lee.
Seems that our regulators have run out of good and worthwhile things to do—and run out of people to annoy all at the same time. Someone or some committee must have needed to justify their ongoing employment. Thus a further load of regulatory bs has been added to that which already exists.
Having worked through the PSA “tool” and having developed a “plan” I am in the compliant 10% and am happy to have given assorted regulators and software “tool” developers something to do for the time being but I wonder what new schemes are being dreamt up to bother us next year and in years to come
That approx. 90% appear not to be compliant tends to demonstrate that the CPD plan and the PGA and PSA tools are bad policy and not acceptable to the majority and that the whole “plan” concept needs to be re-evaluated for real life relevance
Now I assume that the regulators and software developers are actually being paid—unlike the rest of us who must do CPD in our own unpaid time and pay to attend courses etc.—so there’s probably little realisation of the financial and social costs of CPD schemes as they apply to the profession as a whole—maybe there needs to be a cost/benefit study into CPD before any more regulatory schemes
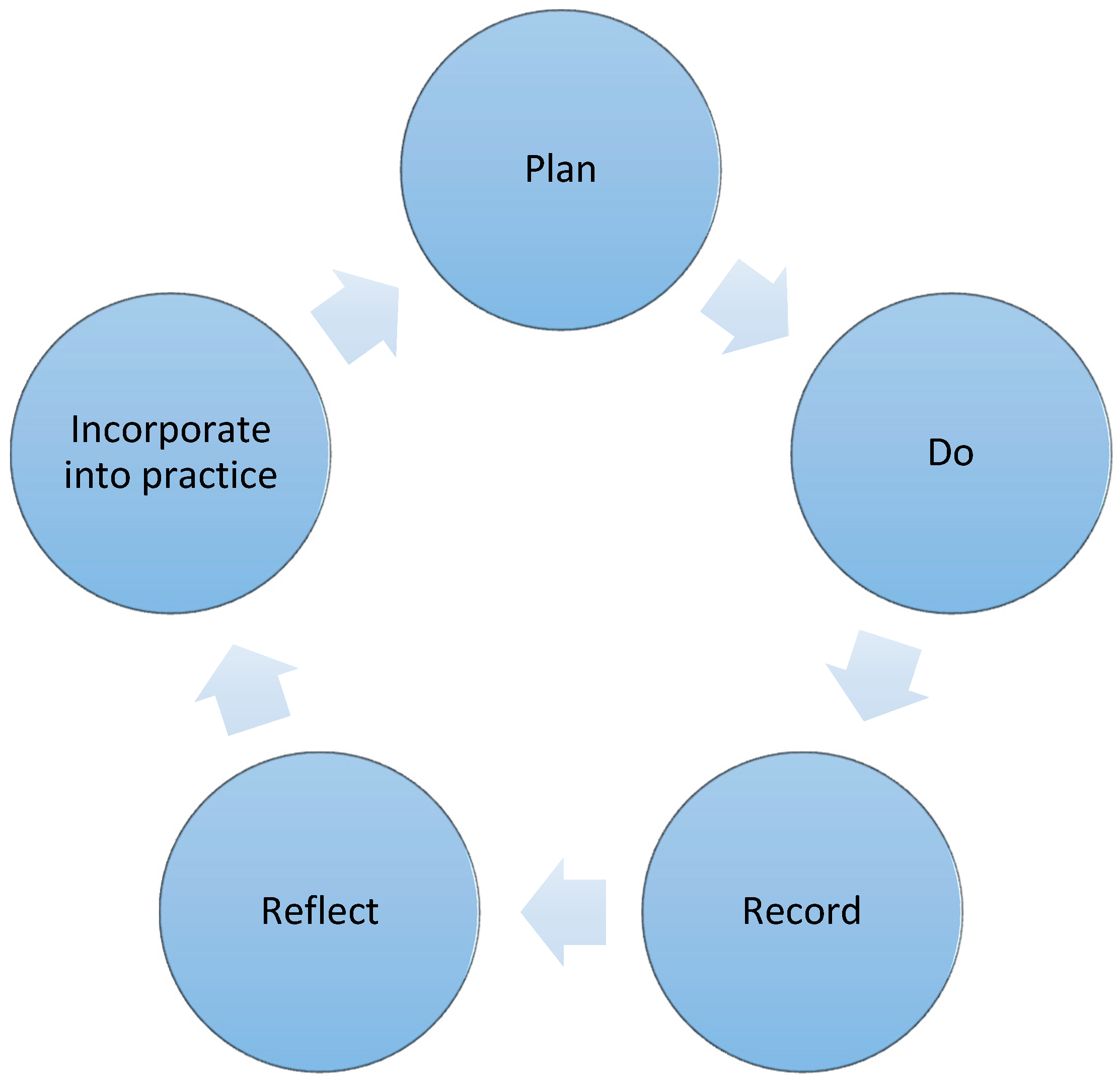
When we develop an in-store promotion or a protocol to achieve a desired outcome we plan the event. We start with a need, weed out the non-essential elements and hone the process until we have a desired workable system. The CPD plan is nothing but an extension of that process. It is to ensure we develop in the best path possible so that we can deliver our knowledge, remain focused and enthused in our profession and not wander off on unproductive tangents. The only difficulty at the moment is the means to develop this, just as professional bodies are also still formulating, but we should be able to jots down personal guideline and ideas as we wait patiently for a definitive checklist or table. Good luck with yours. I realise how challenging it is as I believe that even though I have one, I need to continually monitor and work on it as situations and demands on my talents change.
I think a bigger concern is the current expectation for plan + CPD exceeds all other areas of allied health ... whilst getting paid less.
Anyone who has any clinical responsibility where there recommendation are held to account by medical teams does this automatically. It is not challenging it is a waste of time.
Actually I need sit down and partake in dribble. I learn, and study and do plenty of CPD but I don’t waste time writing a plan. I don’t feel lacking in any areas to plan. Things present themselves and it is only then you realise you don’t know enough so you research it. If you see an interesting conference you do it, as CPD pops up on various websites you follow what takes your fancy. A course comes up that is relevant you do it, I don’t waste time planning and documenting and fluffing about, I get on with it. I don’t waste time recording interventions either as we do to many being in a medical centre and time is precious.
Over documentation and fakery are the nonsense bull dust of the modern world. Wasting time, money and intentions.
Some people might operate that way and it works for them but for me I feel like screaming every time a new rule is introduced to complicate life.
No time for this kind of craps. I have my own plan in my head. I don’t need to write it down as proof to show the board. Pharmacists are not kids and the Board is not our parents. I don’t waste my time that I can use to treat my patients. At home, I need time for my family. Otherwise, my wife would divorce me. Believe it or not, it is true. Will the Board pay me the divorce fee? If not, then leave all pharmacists alone. With only $25 an hour, don’t ask too much from pharmacists. Otherwise, everyone will quit and work for Aldi or BingLee. Same money, but less responsibilities and less crap.
When did Intern supervising get taken off? If that’s the case, I have a lot of hours to do in the next month.
The template is headed ‘Plan/Record’. Are we required to make a record of the past year or a plan for the next year?
Seriously, could there be any more work they want to load on us for the measly $27/hr???!!! I can get that wage at Aldi without all this headache.
Pharmacy is a dead end job!!! Get out while you can.
I really find this ridiculous—I refuse to write a plan. Do they not realise people will write what ever and just dribble in then go about what they do normally anyway? Just like QCPP? All words and fluff and no substance.
I do so much CPD more than I do work actually and spend considerable money on it. I refuse to write a plan. It’s ridiculous. I can now either lie like most people will or send a copy of my new postgraduate degree and say this should bloody cover it. It makes my blood boil. I think everyone should refuse. They can’t deregister us all
Absolutely agree. I doubt that anyone who actually works full time in the profession was involved in the development of this rubbish.
No, I don’t think I’ll be doing this. Undertake and record my mandated yearly points, that’s what I’ll do.
How do you decide what CPD to do? Is it anything that is timely and convenient, or to fill gaps in your knowledge and skills?
Thanks to HMR caps, expensive CPD events/post grad courses were the first thing I culled despite their clinical relevance and profession expansion. Clinical knowledge and practice is not monetarily rewarded, nor is it recognised by the PGA, AACP, PSA in terms of career expansion .... so why put any time and money into it?
Knowledge is power. And that can bring rewards. Think for example about the pilot sites for health care homes announced yesterday. How will practices choose a pharmacist to be part of the HC home? It will be based on your reputation and capacity to contribute to the team. They will be looking for pharmacists with a high level of clinical knowledge.
No, it will be decided as all these things are by informal networks between Pharmacy owners and GP practices. Employee Clinical Pharmacist input = Zero
Knowledge is power, at least in most industries. Absolutely reputation will help you gain a position such as this. However, I’m not holding my breath regarding the HC homes until I see the remuneration offered. Only then can we gauge how the government values clinical pharmacist input. With HMRs being one of the most valuable services available...culling them to me sends a pretty clear message. This move was met with very little resistance from all pharmacy bodies (including accreditation bodies) which sends an even bigger message. This would not have happened in any other industry. So it would appear clinical knowledge gives you very little power where it matters most.
On a side note anyone know the role of the AACP? They didn’t release a position statement when the caps were announced. Their fees haven’t decreased since the caps. All I can see is that they release an occasional newsletter and email regarding upcoming expensive CPD programs they are holding to receive more money (I’m yet to see a medical consultant on the list of speakers, who often offer far greater insight into medication use in their field than a pharmacist).
The only thing Pharmacy owners ever ask prospective Pharmacist employees is how many scripts can you dispense per hour. No one cares about your clinical skills or knowledge nor is it reflected in the Pharmacy award which has become not only the legal minimum but the de facto pay rate for many.
I never, ever, ever do the business-related CPD. It has SFA to do with my practice as a pharmacist and to be frank is insulting that it is scored the same in terms of development in learning about a new drug class, treatment regimen, or health topic.
If I come across a topic I feel I don’t know enough about—that’s my CPD. Hard to plan and map that, because like Uncle Don said “There’s things you know you don’t know, and there’s things you don’t know you don’t know”.
That is what people will do regardless—they will just pretend to plan it at the end of the year. I also feel you don’t know what you want to learn until you realise you don’t know it—then you immediately rectify the situation. Such as coming across a drug or a condition you need to know about but don’t. You don’t plan to study it later in the year to open google and get to it. You target your CPD to your interests and practice anyway.
I understand some people might like to operate that way but for me, useless meaningless paperwork I will not partake of.
Those that are not keeping will not change their practice either—They will just lie.
I do CPD based on (admittedly, self-ID’d) knowledge gaps. Personal and family commitments mean that for me a plan is too constricting (ie. do x at time y), and sometimes things that I thought I needed to study two months ago don’t actually require the active study I thought they did because of the passive intake of information (like Zika for instance—bits and pieces over months complete the picture, rather than a block of time to swot the subject). I’m taking a calculated risk and if I’m audited that’s fine, that’s the game.
All it will do is make people consider what the most relevant training is for them .... and then make them reconcile that against competency standards. And then make them document what they did. And then make them document how it changed their practice. No, that won’t be time consuming at all ....
Why can’t pharmacy just go back to voluntary CPD? Instead of this “Big Brother with the Big (deregistration) Stick” approach.
Umm, I just made my plan; “Get to 40 CPD points” Isn’t that sufficient?
I think this the ultimate “nanny” phenomena. If we accrue 40 points, subject finished requirements met. If you can’t meet the 40 points without a plan you shouldn’t be a registered pharmacist “GO HARD OR GO HOME”.
Anyone with any level of clinical accountability who is not actively seeking to fill knowledge gaps and expand should not be practicing. Direct HMR referrals uncapped would assist with this over “CPD plans” ... call itself auditing by GPs. Written plans are useless. Most will be completed in hindsight based on what was completed earlier in the year.
As pharmacy continues to get raped this plan is ridiculous! CPD is expensive and time consuming as it is. Accredited pharmacists need to complete 60 CPD points .... can only see 20 patients a month and now require a plan! What a joke!!!!
Here’s perspective physio CPD is 20 hours a year
Since we are scientists and deal with evidence-based therapies, can AHPRA or the Pharmacy Board provide us with studies that prove that pharmacists with a CPD plan perform better or are more up to date than those who don’t have a CPD plan?
Time and time again we see examples of how some moron trying to justify their salary and position on the board come up with some stupid idea that gets supported by other idiots who think they are actually more important than they really are. The new requirement for a compulsory CPD plan is yet another example.
I’ve yet to meet one pharmacist who believes in the idea who doesn’t have some other agenda they’re working on (e.g., seeking a position on the board or some academic position because they themselves can’t stand working in community pharmacy anymore).
All the negative comments from other readers to date will as usual be ignored. The point that our pay is a joke is always rebutted with the argument that we should be happy to be working at all or that we are lucky to be in a respected job. Well I’ve got news for you—pharmacy is definitely not what it used to be. The only people I feel worse for are the pharmacy assistants who work their backsides off for the lowest pay rates in the country.
We are all expected to perform a lot more for a lot less these days and sell out our dignity in the process (e.g., Generic substation/“value plus”, discount pharmacy models, etc.). This is apparently the better working standard that is the trade-off for the low pay we’re expected to be content with.
Back to the compulsory CPD plan debate—it won’t achieve anything other than waste pharmacists’ time. The idiot who drafted it will somehow put a spin on it with fancy stats to indicate how it will improve pharmacy practice but it will be a lie. Every pharmacist I’ve spoken to has indicated that if push comes to shove and they have to do it the only way they can draw up a plan is in retrospect i.e., do the compulsory CPD during the year to get the points then work backwards to come up with a plan. How else could it work if you don’t even know what CPD activities are available at the start of the year? So if most pharmacists are planning to come up with the plan in this way how does it achieve anything other than waste all our valuable time. And while on the topic of time could someone please work out what our actual hourly rates are after factoring in all the hours we spend on compulsory CPD as well as the money spent to attend activities, pay for annual registration, professional indemnity insurance, and so on and so on.
Pharmacy is the joke among all university studied professions!
Year after year I see disillusioned young men and women come out into the pharmacy workforce regretting their choice of career.
For myself I only work in pharmacy on weekends because the penalty rates (while they still exist) at least make it bearable. I have a second job in another industry during the week so that I can maintain a half decent lifestyle otherwise I would fall below the poverty line like all our poor pharmacy assistants.
I’m a casual locum ......... I’m stuffed if I can satisfy the Boards multi-level requirements in their “PLAN” ....... I have had no problem obtaining 100 plus Points annually since CPD started, you can’t tell me I’m not trying!!
CPD’s should only be used as a punishment system for pharmacists who have demonstrated negligent practices. Everyone else has demonstrated that the knowledge they acquired studying to become b a pharmacist or due to their experience as being a pharmacist is sufficient enough for the health care needs of their workplace and demographic.
I do believe we need to keep up-to-date and do a lot of CPD to [keep] up to speed and because I like to learn but these plans are just bull shittery concocted up by some numpty with ocd.
The board is dreaming if they think their $26 pharmacists will spend a single minute on this rubbish. Hell being deregistered could be a blessing in disguise. You’ll probably earn more elsewhere anyways.
No time for this kind of crap. I have my own plan in my head. I don’t need to write it down as proof to show the board. Pharmacists are not kids and the Board is not our parents. I don’t waste my time that I can use to treat my patients. At home, I need time for my family. Otherwise, my wife would divorce me. Will the Board pay me the divorce fee? If not, then leave all pharmacists alone. With only $25 an hour, don’t ask too much from pharmacists. Otherwise, everyone will quit and work for Aldi or BingLee. Same money, but less responsibilities and less craps.
If the board has time to audit pharmacists regarding the CPD plan, I am wondering why they don’t audit Chemist Warehouse for compliance of Pharmacy Standards? Pharmacists in Chemist Warehouse don’t counsel patients at all. It is not their fault, but the fault of the founders of Chemist Warehouse.
Pharmacists with no CPD plan do not cause any harm to patients, but Chemist Warehouse giving out medications without counseling would cause harm.
I myself don’t have time to write down the CPD plan. I won’t do it until the Board provide proof that all other pharmacists have the plan. I have the same plan as “Ain’t nobody got time for dat” in this forum, namely: Get to 40 CPD points. Simple!!!
Can I point out that a plan is personal to you and your circumstances. It can be simple or complicated and you sure don’t need a workshop to make one. I’m pretty sure you are not going to be marked on it! Bit of common sense needed in this discussion.
Exactly, it’s mindless busy work.
The revised registration standards and CPD guidelines followed a rigorous public consultation process
I agree that we were informed early enough of the need to have a CPD plan, however I strongly dispute the suggestion that this followed a “rigorous consultation process”. Who exactly was consulted. I certainly wasn’t, nor was I aware that there was a consultation process.
Bureaucratic time wasting. Next they’ll have us write a protocol for attending CPD events, requiring a plan on where we sit, when we started sitting and how it impacted our learning by sitting in that spot.
SHPA also has a package of material to support members prepare a learning plan—including an online presentation that explains in detail how to develop a learning plan and competency grids for a range of pharmacist roles.


 ,
, 

{kind=link}
{kind=link}
{kind=link}


