Development of Pharmacy Practice in European Countries—The Polish Perspective




Abstract
:1. Introduction
2. Community Pharmacy in Poland—The Legal Framework
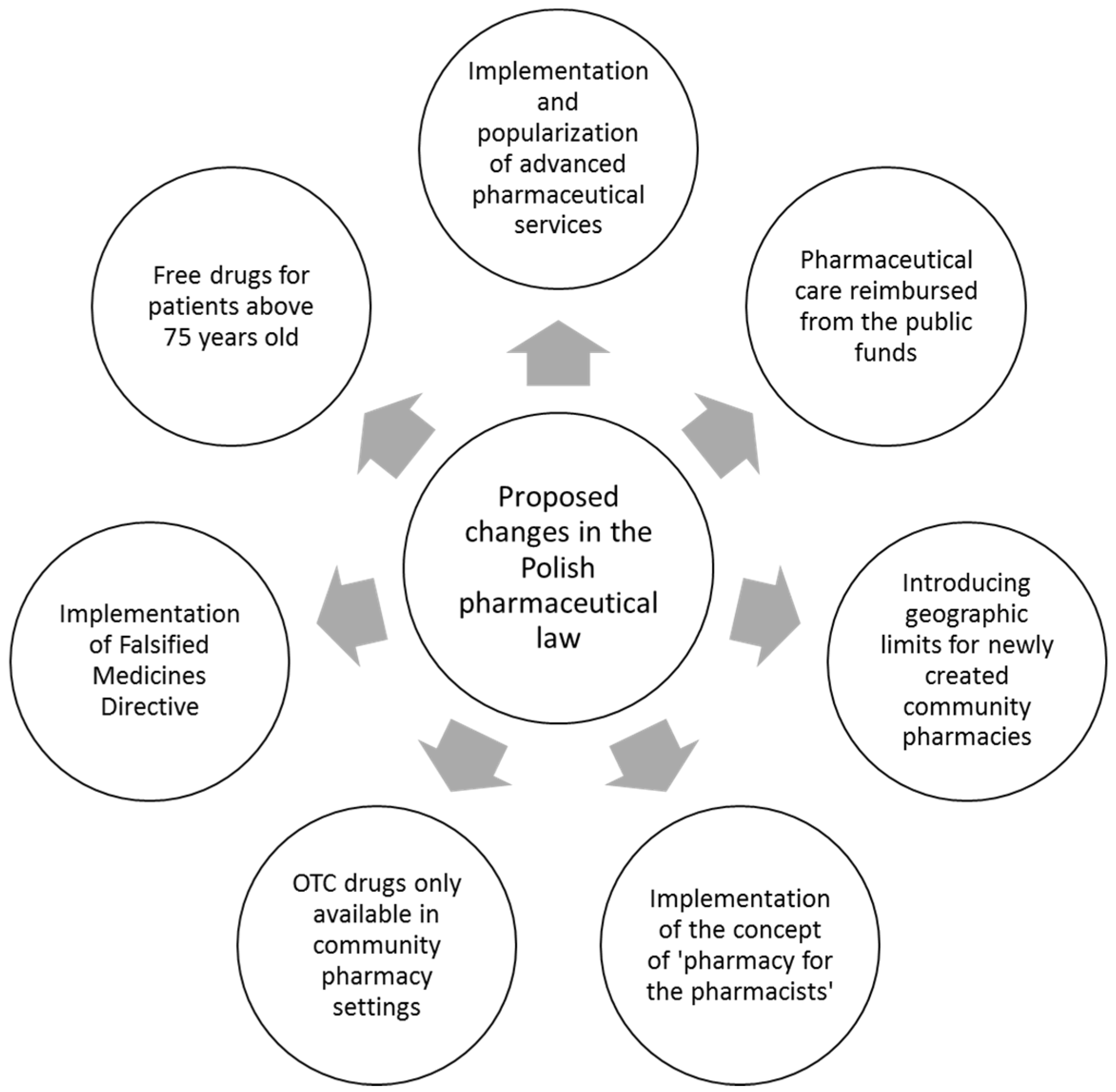
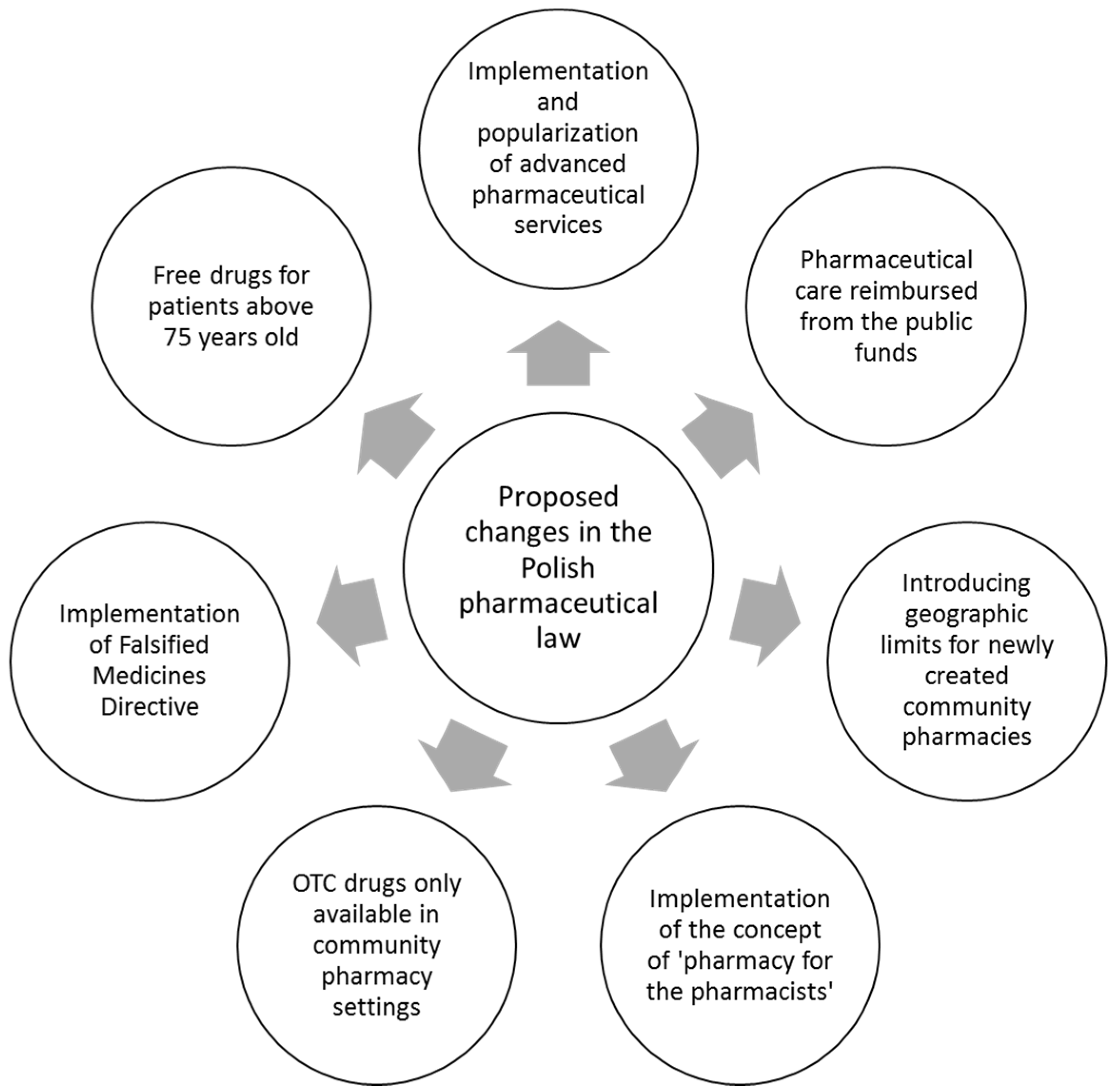
3. Pharmaceutical Care in Poland—Still Not Implemented
4. Reimbursed Services—The Future of Pharmacy Practice in Poland
5. New Deal in Community Pharmacies—“Pharmacy for the Pharmacist”
6. OTC Drugs—Only in Community Pharmacies
7. Free Drugs for Patients above 75 Years Old
8. Falsified Medicines Directive—New Responsibilities for Community Pharmacists
9. Other Challenges and a Glimpse of the Future
Author Contributions
Conflicts of Interest
References
- Pawłowska, I.; Pawłowski, L.; Kocić, I.; Krzyżaniak, N. Clinical and conventional pharmacy services in Polish hospitals: A national survey. Int. J. Clin. Pharm. 2016, 38, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Rynek Aptek. Statystycznie co trzecia apteka powinna być zlikwidowana—POLITYKA LEKOWA. Available online: http://www.rynekaptek.pl/polityka-lekowa/statystycznie-co-trzecia-apteka-powinna-byc-zlikwidowana,2538.html (accessed on 30 July 2017).
- Rynek Aptek. PharmaExpert: Konsolidacja przebiega oddolnie—FINANSE I ZARZĄDZANIE. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/pharmaexpert-konsolidacja-przebiega-oddolnie,10782.html (accessed on 30 July 2017).
- Rynek Aptek. Opieka farmaceutyczna: Zaczniemy od rzeczy prostych—FINANSE I ZARZĄDZANIE. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/opieka-farmaceutyczna-zaczniemy-od-rzeczy-prostych,14602.html (accessed on 30 July 2017).
- Ministerstwo Zdrowia. O zawodzie farmaceuty. Available online: http://www.mz.gov.pl/system-ochrony-zdrowia/kadra-medyczna-i-ksztalcenie/farmaceuci/o-zawodzie-farmaceuty/ (accessed on 30 July 2017).
- Swieczkowski, D.; Zimmermann, A. Zawod technika farmaceutycznego. Farm. Pol. 2014, 4, 198–204. [Google Scholar]
- Ustawa z dn. 6 września 2001 r. Prawo farmaceutyczne (Polish). Pharmaceutical Law Act, Dz.U. 2001 nr 126 poz. 1381. Available online: https://www.ksiegarnia.beck.pl/media/product_custom_files/1/0/10411-prawo-farmaceutyczne-the-pharmaceutical-law-michele-le-mauviel-darmowy-fragment.pdf (accessed on 30 July 2017).
- Swieczkowski, D.; Mogielnicki, M.; Merks, P.; Gruchala, M.; Jaguszewski, M. Pharmaceutical services as a tool to improve outcomes in patients with cardiovascular diseases. Int. J. Cardiol. 2016, 29, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Rotta, I.; Salgado, T.M.; Silva, M.L.; Correr, C.J.; Fernandez-Llimos, F. Effectiveness of clinical pharmacy services: An overview of systematic reviews (2000–2010). Int. J. Clin. Pharm. 2015, 37, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Ustawa z dn. 19.04.1991 r. o izbach aptekarskich (Polish), Pharmaceutical Chambers Act, Dz.U. 2014 poz. 1429. Available online: http://isap.sejm.gov.pl/DetailsServlet?id=WDU20140001429 (accessed on 30 July 2017).
- Mokrzycka, A.; Kowalska-Bobko, I.; Sagan, A.; Wlodarczyk, W.C. The 2014 primary health care reform in Poland: Short-term fixes instead of a long-term strategy. Health Policy 2016, 120, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Stepurko, T.; Pavlova, M.; Groot, W. Overall satisfaction of health care users with the quality of and access to health care services: A cross-sectional study in six Central and Eastern European countries. BMC Health Serv. Res. 2016, 16, 342. [Google Scholar] [CrossRef] [PubMed]
- Holecki, T.; Romaniuk, P.; Woźniak-Holecka, J. The Systemic Changes to Improve Efficiency in Polish Primary Health Care. Front. Pharmacol. 2016, 7, 209. [Google Scholar] [CrossRef] [PubMed]
- Skowron, A.; Bułaś, L.; Drozd, M.; Karolewicz, B.; Machalska, J. Prospects for development of pharmacy in Poland until the year 2030. The document of the National Section of Pharmaceutical Care of The Polish Pharmaceutical Society. Acta Pol. Pharm. 2016, 73, 255–266. [Google Scholar] [PubMed]
- Skowron, A.; Polak, S.; Brandys, J. The impact of pharmaceutical care on patients with hypertension and their pharmacists. Pharm. Pract. 2011, 9, 110–115. [Google Scholar] [CrossRef]
- Rynek Aptek. Recepty powtarzane—jeden z przykładów opieki farmaceutycznej. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/recepty-powtarzane-jeden-z-przykladow-opieki-farmaceutycznej,12411.html (accessed on 30 July 2017).
- Swieczkowski, D.; Poniatowski, P.; Merks, P. The pharmaceutical care in asthma—Polish and global perspective. Pneumonol. Alergol. Pol. 2016, 84, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Ministerstwo Zdrowia. Minister zdrowia podpisał rozporządzenia umożliwiające realizację nowych uprawnień pielęgniarek i położnych. Available online: http://www.mz.gov.pl/aktualnosci/minister-zdrowia-podpisal-rozporzadzenia-umozliwiajace-realizacje-nowych-uprawnien-pielegniarek-i-poloznych/ (accessed on 30 July 2017).
- Rynek Aptek. Opieka farmaceutyczna dla wszystkich chętnych aptek—FINANSE I ZARZĄDZANIE. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/opieka-farmaceutyczna-dla-wszystkich-chetnych-aptek,12565.html (accessed on 30 July 2017).
- Rynek Aptek. MZ: Zespół ds. opieki farmaceutycznej został rozwiązany. Available online: http://www.rynekzdrowia.pl/Farmacja/MZ-Zespol-ds-opieki-farmaceutycznej-zostal-rozwiazany,165190,6.html (accessed on 30 July 2017).
- Rynek Aptek. Prezydent podpisał ustawę “apteka dla aptekarza”—PRAWO. Available online: http://www.rynekaptek.pl/prawo/prezydent-podpisal-ustawe-apteka-dla-aptekarza,19804.html (accessed on 30 July 2017).
- Rynek Aptek. Poselski projekt nowelizacji ustawy Prawo Farmaceutyczne—PRAWO. Available online: http://www.rynekaptek.pl/prawo/poselski-projekt-nowelizacji-ustawy-prawo-armaceutyczne,17450.html (accessed on 30 July 2017).
- Employed community Pharmacists in Europe (EPhEU)—Pharmacy in Europe—Poland. Available online: http://www.epheu.eu/pharmacy-in-europe/poland/ (accessed on 30 July 2017).
- Rynek Aptek. MZ: Co najmniej 51 proc. udziałów w aptece dla magistra farmacji—FINANSE I ZARZĄDZANIE. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/mz-co-najmniej-51-proc-udzialow-w-aptece-dla-magistra-farmacji,13494.html (accessed on 30 July 2017).
- Rynek Aptek. KP Lewiatan: Zmiana prawa, wyższe ceny—FINANSE I ZARZĄDZANIE. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/kp-lewiatan-zmiana-prawa-wyzsze-ceny,17590.html (accessed on 30 July 2017).
- Rynek Aptek. BAS: Proponowane kryteria mogą naruszać prawo UE—PRAWO. Available online: http://www.rynekaptek.pl/prawo/bas-proponowane-kryteria-moga-naruszac-prawo-ue,17511.html (accessed on 30 July 2017).
- Rynek Aptek. Sprzedaż leków w sklepach rodzi wiele nieprawidłowości—FINANSE I ZARZĄDZANIE. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/sprzedaz-lekow-w-sklepach-rodzi-wiele-nieprawidlowosci,15124.html (accessed on 30 July 2017).
- Rynek Aptek. PharmaNET: Apelujemy o rzetelną debatę—FINANSE I ZARZĄDZANIE. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/pharmanet-apelujemy-o-rzetelna-debate,9631.html (accessed on 30 July 2017).
- Portal farmaceutyczno—medyczny. Poza apteką zły pomysł. Available online: https://www.pfm.pl/artykuly/poza-apteka-zly-pomysl/668 (accessed on 30 July 2017).
- Wyborcza.biz. Będą ograniczenia w sprzedaży leków w Polsce. A jak jest w Europie? Available online: http://wyborcza.biz/biznes/1,147743,19481770,beda-ograniczenia-w-sprzedazy-lekow-w-polsce-a-jak-jest-w-europie.html?disableRedirects=true (accessed on 30 July 2017).
- Rynek Aptek. Projekt listy S będzie około 1 sierpnia—POLITYKA LEKOWA. Available online: http://www.rynekaptek.pl/polityka-lekowa/projekt-listy-s-bedzie-okolo-1-sierpnia,14455.html (accessed on 30 July 2017).
- Rynek Aptek. Wykaz S dość naukowo opracowany—POLITYKA LEKOWA. Available online: http://www.rynekaptek.pl/polityka-lekowa/wykaz-s-dosc-naukowo-opracowany,15330.html (accessed on 30 July 2017).
- Lewey, J.; Shrank, W.H.; Avorn, J.; Liu, J.; Choudhry, N.K. Medication adherence and healthcare disparities: Impact of statin co-payment reduction. Am. J. Manag. Care 2015, 21, 696–704. [Google Scholar] [PubMed]
- NICE. Medicines adherence: Involving patients in decisions about prescribed medicines and supporting adherence. Available online: https://www.nice.org.uk/guidance/cg76 (accessed on 30 July 2017).
- Merks, P.; Swieczkowski, D.; Byliniak, M.; Drozd, M.; Krupa, K.; Jaguszewski, M.; Brindley, D.A.; Naughton, B.D. The European Falsified Medicines Directive in Poland: Background, implementation and potential recommendations for pharmacists. Eur. J. Hosp. Pharm. 2016. [Google Scholar] [CrossRef]
- Smith, G.; Smith, J.A.; Brindley, D.A. The Falsified Medicines Directive: How to secure your supply chain. J. Generic Med. 2014, 11, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Naughton, B.; Roberts, L.; Dopson, S.; Chapman, S.; Brindley, D. Effectiveness of medicines authentication technology to detect counterfeit, recalled and expired medicines: A two-stage quantitative secondary care study. BMJ Open 2016, 6, e013837. [Google Scholar] [CrossRef] [PubMed]
- Beninger, P. Opportunities for Collaboration at the Interface of Pharmacovigilance and Manufacturing. Clin. Ther. 2017, 39, 702–712. [Google Scholar] [CrossRef] [PubMed]
- Rynek Aptek. Lubelskie: Braki leków w aptekach. “Odwrócony łańcuch” trwa—PRAWO. Available online: http://www.rynekaptek.pl/marketing-i-zarzadzanie/lubelskie-braki-lekow-w-aptekach-quot-odwrocony-lancuch-quot-trwa,11876.html (accessed on 30 July 2017).
- Rynek Aptek. Batalia ŚIA o przestrzeganie zakazu reklamy aptek—PRAWO. Available online: http://www.rynekaptek.pl/prawo/batalia-sia-o-przestrzeganie-zakazu-reklamy-aptek,17508.html (accessed on 30 July 2017).
- Piecuch, A.; Kozłowska-Wojciechowska, M.; Jaszewska, E.; Makarewicz-Wujec, M. Farmaceuta kliniczny—odpowiedź na zmieniające się potrzeby społeczne. Farm. Pol. 2014, 70, 395–399. [Google Scholar]

{kind=link}
| Highlights |
|---|
|
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Świeczkowski, D.; Merks, P.; Cwalina, N.; Jaguszewski, M.J. Development of Pharmacy Practice in European Countries—The Polish Perspective. Pharmacy 2017, 5, 43. https://doi.org/10.3390/pharmacy5030043
Świeczkowski D, Merks P, Cwalina N, Jaguszewski MJ. Development of Pharmacy Practice in European Countries—The Polish Perspective. Pharmacy. 2017; 5(3):43. https://doi.org/10.3390/pharmacy5030043
Chicago/Turabian StyleŚwieczkowski, Damian, Piotr Merks, Natalia Cwalina, and Miłosz J. Jaguszewski. 2017. "Development of Pharmacy Practice in European Countries—The Polish Perspective" Pharmacy 5, no. 3: 43. https://doi.org/10.3390/pharmacy5030043
APA StyleŚwieczkowski, D., Merks, P., Cwalina, N., & Jaguszewski, M. J. (2017). Development of Pharmacy Practice in European Countries—The Polish Perspective. Pharmacy, 5(3), 43. https://doi.org/10.3390/pharmacy5030043