Assessment of Insulin-related Knowledge among Healthcare Professionals in a Large Teaching Hospital in the United Kingdom



Abstract
:1. Introduction
- To identify specific knowledge gaps amongst healthcare professionals regarding insulin products and dosing regimens.
- To determine correlations between insulin knowledge, self-reported confidence level, professional group and years of experience of healthcare professionals.
- To describe healthcare professionals’ experiences of previous involvement in insulin-related medication errors, and their recommendations for improving insulin safety.
2. Materials and Methods
Data Analysis Approach
3. Results
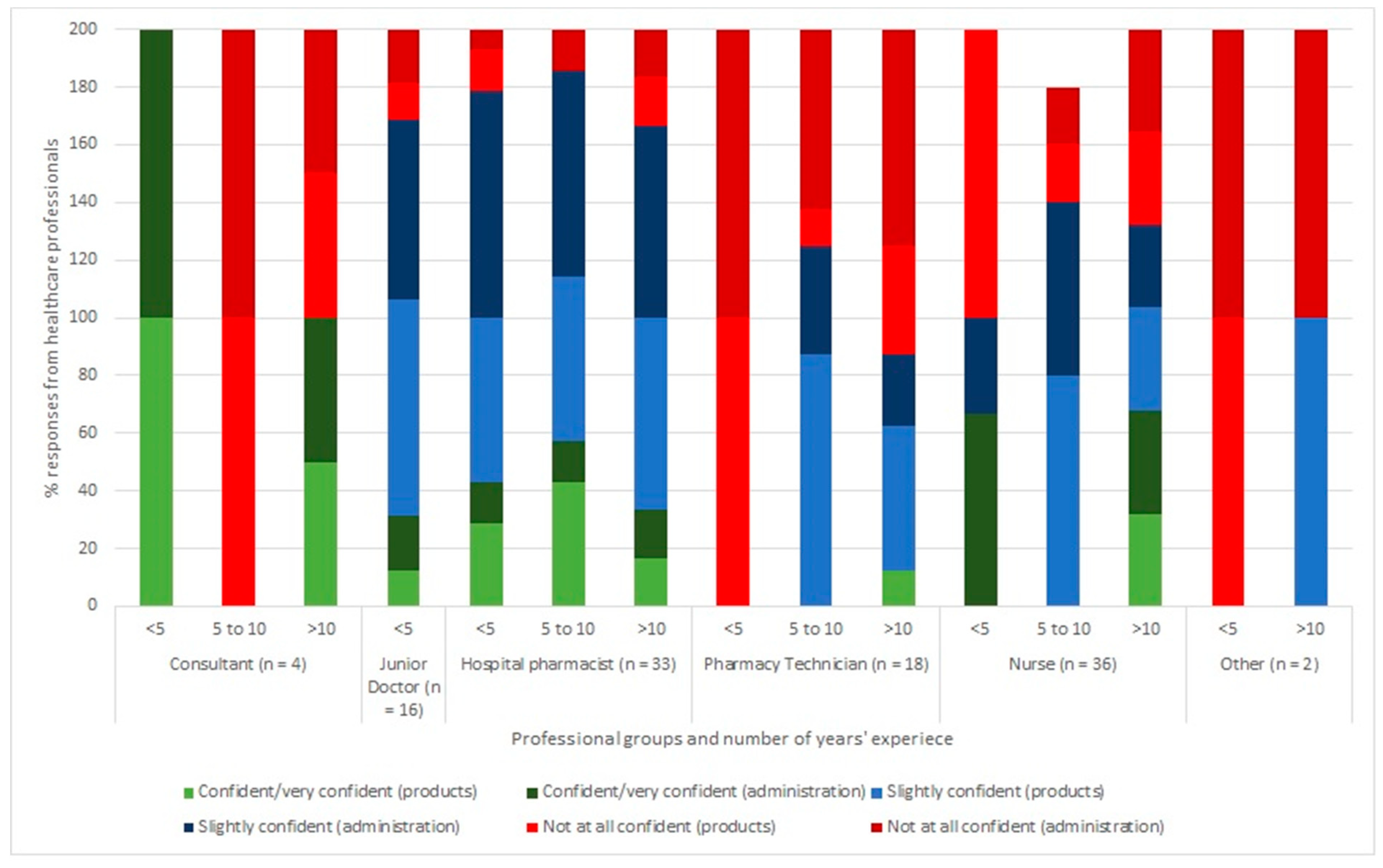
3.1. Confidence Level and Insulin-Related Knowledge
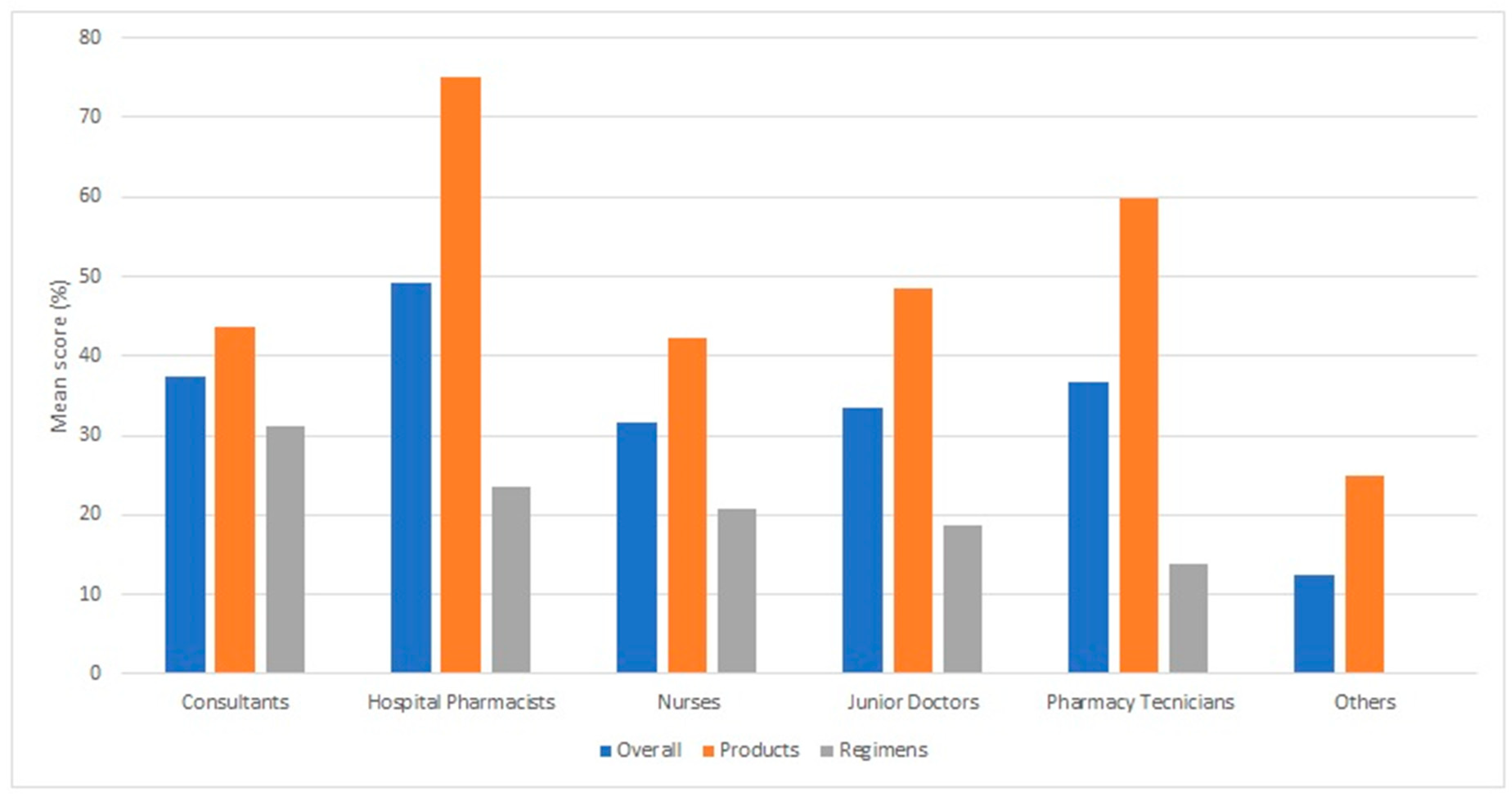
3.2. Professional Group, Experience and Insulin-Related Knowledge
3.3. Insulin Incidents and Interventions
4. Discussion
4.1. Confidence Level and Insulin-Related Knowledge
4.2. Professional Group, Experience and Insulin-Related Knowledge
4.3. Insulin Incidents and Interventions
4.4. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Institute of Safe Medication Practitices. ISMP List of High-Alert Medications in Acute Care Settings. 2011. Available online: https://www.ismp.org/Tools/institutionalhighAlert.asp (accessed on 10 January 2019).
- Smith, W.D.; Winterstein, A.G.; Johns, T.; Rosenberg, E.; Sauer, B.C. Causes of hyperglycemia and hypoglycemia in adult inpatients. Am. J. Health Syst. Pharm. 2005, 62, 714–719. [Google Scholar] [PubMed]
- National Patient Safety Agency. Safer Administration of Insulin; 14410; NHS: London, UK, 2010. [Google Scholar] [CrossRef]
- Frier, B.M.; Heller, S.; McCrimmon, R. Hypoglycaemia in Clinical Diabetes, 3rd ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Bilous, R.; Donnelly, R. Handbook of Diabetes; Wiley-Blackwell: Oxford, UK, 2010. [Google Scholar] [CrossRef]
- Sims, J.; Richardson, T.; Kerr, D. Insulin errors in hospital: Time for a radical re-think on risk? Clin. Risk 2010, 16, 89–92. [Google Scholar] [CrossRef]
- Budnitz, D.S.; Pollock, D.A.; Weidenbach, K.N.; Mendelsohn, A.B.; Schroeder, T.J.; Annest, J.L. National surveillance of emergency department visits for outpatient adverse drug events. JAMA 2006, 296, 1858–1866. [Google Scholar] [CrossRef] [PubMed]
- Cousins, D.; Rosario, C.; Scarpello, J. Insulin, hospitals and harm: A review of patient safety incidents reported to the National Patient Safety Agency. Clin. Med. 2011, 11, 28–30. [Google Scholar] [CrossRef]
- Health and Social Care Information Centre. National Diabetes Inpatient Audit 2016; Health and Social Care Information Centre: Leeds, UK, 2017.
- Cornish, W. Safe and appropriate use of insulin and other antihyperglycemic agents in hospital. Can. J. Diabetes 2014, 38, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Oiknine, R.; Bernbaum, M.; Mooradian, A.D. A critical appraisal of the role of insulin analogues in the management of diabetes mellitus. Drugs 2005, 65, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Prescrire Editorial Staff. Insulin use: Preventable errors. Prescrire Int. 2014, 23, 14–17. [Google Scholar]
- Remtulla, S.; Brown, G.; Frighetto, L. Best possible medication history by a pharmacy technician at a tertiary care hospital. Can. J. Hosp. Pharm. 2009, 62, 402–405. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22478923 (accessed on 14 June 2017). [CrossRef]
- Owen, M. Insulin administration in the community: A project. Br. J. Healthc. Assist. 2009, 3, 546–550. [Google Scholar] [CrossRef]
- Agbasi, N. Teaching carers how to administer insulin: A residential care home project. J. Diabetes Nurs. 2017, 21. Available online: http://www.thejournalofdiabetesnursing.co.uk/media/content/_master/4892/files/pdf/jdn21-2-67-71.pdf (accessed on 14 June 2017).
- Derr, R.L.; Sivanandy, M.S.; Bronich-Hall, L.; Rodriguez, A. Insulin-related knowledge among health care professionals in internal medicine. Diabetes Spectr. 2007, 20, 177–185. [Google Scholar] [CrossRef]
- Robb, A.; Reid, B.; Laird, E.A. Insulin knowledge and practice: A survey of district nurses in Northern Ireland. Br. J. Community Nurs. 2017, 22, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, L. Improving safety of insulin administration: A pilot audit of hospital staff knowledge. J. Diabetes Nurs. 2012, 16, 8–16. [Google Scholar]
- Lee, M.K.; Liu, Z.; Quek, T.P.; Chew, D.E. Insulin-related knowledge among health care professionals at a tertiary hospital. Diabetes Spectr. 2013, 26, 187–193. [Google Scholar] [CrossRef]
- Hellman, R. A systems approach to reducing errors in insulin therapy in the inpatient setting. Endocr. Pract. 2004, 10, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.G.; Morris, C.; Rayman, G. An interactive 1-h educational programme for junior doctors, increases their confidence and improves inpatient diabetes care. Diabet. Med. 2012, 29, 1574–1578. [Google Scholar] [CrossRef]
- Sullivan, M.M.; O’brien, C.R.; Gitelman, S.E.; Shapiro, S.E.; Rushakoff, R.J. Impact of an interactive online nursing educational module on insulin errors in hospitalized pediatric patients. Diabetes Care 2010, 33, 1744–1746. [Google Scholar] [CrossRef] [PubMed]
- Herring, R.; Pengilley, C.; Hopkins, H.; Tuthill, B.; Patel, N.; Nelson, C.; Currie, A.; Russell-Jones, D.L. Can an interprofessional education tool improve healthcare professional confidence, knowledge and quality of inpatient diabetes care: A pilot study? Diabet. Med. 2013, 30, 864–870. [Google Scholar] [CrossRef]
- DeSalvo, D.J.; Greenberg, L.W.; Henderson, C.L.; Cogen, F.R. A learner-centered diabetes management curriculum: Reducing resident errors on an inpatient diabetes pathway. Diabetes Care 2012, 35, 2188–2193. [Google Scholar] [CrossRef]
- Al-Yassin, A.; Al-Khaja, A.; Jichi, F.; Clarke, C.; Lisk, C.; Katz, J.R. Introducing a diabetes e-learning module: A means of improving junior doctors’ confidence and ability in managing inpatients with diabetes. Pract. Diabetes 2013, 30, 122. [Google Scholar] [CrossRef]
- Cohen, M.R. Pharmacists’ role in ensuring safe and effective hospital use of insulin. Am. J. Health Syst. Pharm. AJHP 2010, 67, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Segal, A.R.; Brunner, J.E.; Burch, F.T.; Jackson, J.A. Use of concentrated insulin human regular (U-500) for patients with diabetes. Am. J. Health Syst. Pharm. 2010, 67, 1526–1535. [Google Scholar] [CrossRef] [PubMed]
- NHS Improvement. Risk of severe harm and death due to withdrawing insulin from pen devices. Patient Saf. Alert. 2016. Available online: https://improvement.nhs.uk/uploads/documents/Patient_Safety_Alert_-_Withdrawing_insulin_from_pen_devices.pdf (accessed on 22 May 2017).
- NHS Wales. Ensuring the Safe Administration of Insulin Patient Safety Alert Risks associated with extracting insulin from pen devices Use of Safety-Engineered Devices. Patient Saf. Alert. 2016. Available online: http://www.patientsafety.wales.nhs.uk/sitesplus/documents/1104/PSA004 Admin of insulin WEB.pdf (accessed on 22 May 2017).
- Cardwell, J.; Hardy, K.; Ford, N.; O’Brien, S. Assessment of diabetes knowledge in trained and untrained ward nurses before and after intensive specialist support. J. Diabetes Nurs. 2016, 20, 60–64. [Google Scholar]



{kind=link}
{kind=link}
| Very Confident | Confident | Sligtly Confident | Not at All Confident | |
|---|---|---|---|---|
| Number of respondants (N) | ||||
| Insulin products questions | 3 | 20 | 58 | 28 |
| Insulin regimens questions | 5 | 17 | 51 | 36 |
| Mean (%) correct answers | ||||
| Insulin products questions (overall) | 67 (58) | 75 (54) | 57 (39) | 38 (22) |
| Insulin regimens questions (overall) | 50 (58) | 24 (43) | 25 (44) | 8 (25) |
| Multiple-choice Question Asked (Answers in Italic) | Pharmacist (n = 33) | Pharmacy Technician (n = 18) | Junior Doctor (n = 16) | Consultant (n = 4) | Nurse (n = 36) | Other (n = 2) | Overall (n = 109) |
|---|---|---|---|---|---|---|---|
| 6. Which insulin should be administered 15 min prior to meals?Humulin M3, Humulin S | 15 | 17 | 13 | 25 | 3 | 0 | 11 |
| 7. Which insulin(s) are to be administered at mealtimes?Humalog | 64 | 33 | 25 | 50 | 33 | 0 | 41 |
| 8. Which insulin preparation should never be given at night?Humalog Mix 50, Apidra, NovoRapid, Humulin S | 3 | 0 | 13 | 0 | 19 | 0 | 9 |
| 9. Levemir (detemir) isa long-acting insulin | 91 | 67 | 81 | 50 | 50 | 50 | 70 |
| 10. Which of the following is a basal (long-acting) insulin?Lantus (glargine) | 97 | 83 | 100 | 75 | 83 | 50 | 89 |
| 11.What is the duration of action for NovoMix 30?16–24 h | 33 | 33 | 0 | 0 | 6 | 0 | 17 |
| 12.Subcutaneous (SC) Actrapid should not be administered at intervals less than4 h | 12 | 6 | 25 | 50 | 28 | 0 | 19 |
| 13.Which of the following insulin products contain 100 units/mL?Humulin S, Lantus, Novorapid | 79 | 56 | 13 | 50 | 31 | 0 | 47 |
| Average | 49 | 37 | 34 | 38 | 32 | 13 | 38 |
| Max/Min | 97/3 | 83/0 | 100/0 | 75/0 | 83/3 | 50/0 | 89/9 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bain, A.; Kavanagh, S.; McCarthy, S.; Babar, Z.-U.-D. Assessment of Insulin-related Knowledge among Healthcare Professionals in a Large Teaching Hospital in the United Kingdom. Pharmacy 2019, 7, 16. https://doi.org/10.3390/pharmacy7010016
Bain A, Kavanagh S, McCarthy S, Babar Z-U-D. Assessment of Insulin-related Knowledge among Healthcare Professionals in a Large Teaching Hospital in the United Kingdom. Pharmacy. 2019; 7(1):16. https://doi.org/10.3390/pharmacy7010016
Chicago/Turabian StyleBain, Amie, Sallianne Kavanagh, Sinead McCarthy, and Zaheer-Ud-Din Babar. 2019. "Assessment of Insulin-related Knowledge among Healthcare Professionals in a Large Teaching Hospital in the United Kingdom" Pharmacy 7, no. 1: 16. https://doi.org/10.3390/pharmacy7010016
APA StyleBain, A., Kavanagh, S., McCarthy, S., & Babar, Z.-U.-D. (2019). Assessment of Insulin-related Knowledge among Healthcare Professionals in a Large Teaching Hospital in the United Kingdom. Pharmacy, 7(1), 16. https://doi.org/10.3390/pharmacy7010016