Development, Testing and Results of a Patient Medication Experience Documentation Tool for Use in Comprehensive Medication Management Services

Abstract
:1. Introduction
2. Materials and Methods
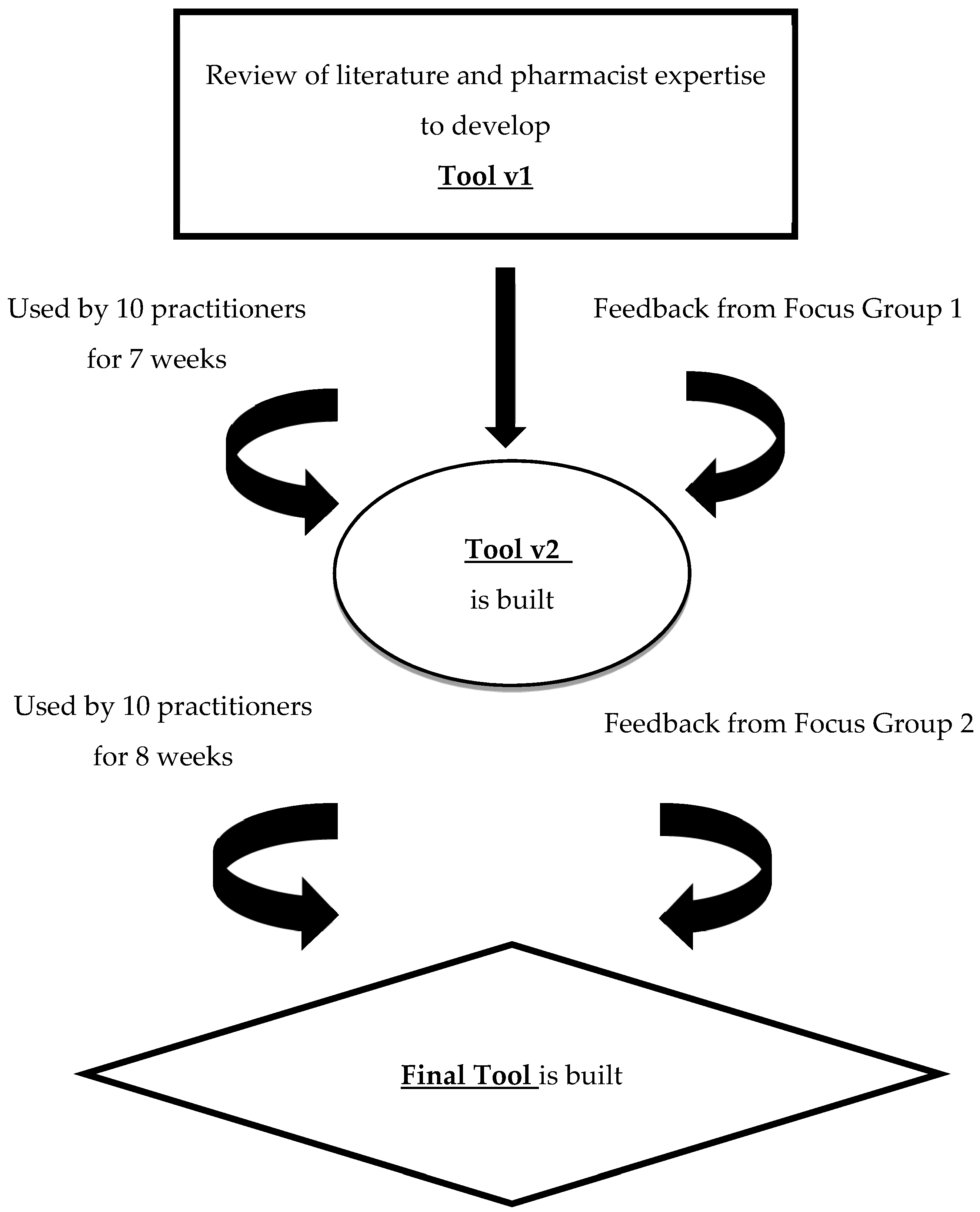
2.1. Tool Development
2.2. Tool Testing
2.2.1. Setting
2.2.2. Testing Period
2.2.3. Tool Results
2.3. Focus Groups with Pharmacists
Human Subjects Protection
3. Results
3.1. Tool Development
3.2. Tool Utilization and Results
3.3. Pharmacist Focus Groups
3.3.1. Usefulness of the Tool
The Tool Makes CMM Pharmacists More Aware of the Medication Experience and More Reflexive
Using the Tool Makes Pharmacists Realize the Fluidity of the Medication Experience
The Tool Assists with Teaching
The Tool Helps with Future Care Plans
3.3.2. Challenges of Using the Tool
Being Reflexive Can Be Burdensome
Unearthing the Difference between the Medication Experience and a Drug Therapy Problem
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. The Medication Experience Documentation Tool
| MEDICATION EXPERIENCE AFFECTING MEDICATION OUTCOMES FOR TODAY’S VISIT (select one or more and then select associated overall strategies): |
| None |
| Feelings of burden and being overwhelmed (ex: pill burden) |
Does not want to take medications because:
|
Fears/concerns about side effects:
|
| Fears/concerns about becoming dependent on a medication |
| Fears/concerns medication (ex: generic) will not be effective |
| Self adjusts medication regimen (increases, decrease, or skips doses) |
Increasing medication(s) or increasing medication dose(s) means:
|
| Prefers alternative non-drug therapy or lifestyle changes |
| Fear of not having medication(s)/too reliant on Rx medication(s) (security) |
| *** (write-in) |
| STRATEGIES USED TODAY THAT EFFECTIVELY IMPROVED MEDICATION RELATED OUTCOMES: |
| Open ended questions |
| Collaboration/Shared Decision Making |
| Negotiate |
| Evocation/Empower |
| Support autonomy /Emphasizing personal choice and control |
| Ask permission |
| Raise concern, educate, or inform |
| Reframe/ Reflection |
| Roll with resistance |
| Using a rating scale, on scale of 1-10, Importance *** Confidence *** |
| Elicit change talk |
| Encourage non-drug therapy or lifestyle changes |
| Referral to care team member |
| *** (write-in) |
Appendix B. Motivational Interviewing Strategy Definitions (11–13)
- Open ended questions: Using stems such as “what” and “how” that can elicit unlimited answers from a patient and invite them to talk.
- Collaboration/Shared Decision Making: Co-developing goals with the patient to make sure they are involved in creating a plan that will indeed work for the patient.
- Negotiate: Meeting the patient “in the middle”. Perhaps the plan does not exactly match what you want as the practitioner, but is a smaller more reasonable goal is agreed upon that acts as a stepping stone to reach the ultimate goal.
- Evocation/Empower:
- Helping your patient explore how they can make a difference in their own health by utilizing their own ideas and resources.
- Facilitating the patient in bringing their own expertise to the discussion on how best to accomplish change.
- Drawing out the patient’s own motivation to change.
- Support autonomy/Emphasizing personal choice and control:
- Acknowledge to the patient that they are ultimately responsible for change and as the practitioner we separate ourselves from the outcome.
- Communicating respect and dignity of the patient through unconditional positive regard.
- Ask permission: Informing or advising only after the patient has given you permission to do so. Forms of permission would include a patient asking for advice or asking the patient for permission to inform (like knocking on a door before entering). Examples are; “May I make a suggestion?” or prefacing advice with “You can tell me what you think of this idea….”.
- Raise concern, educate, or inform: The actual act of providing patient with information and advice.
- Reframe/Reflection:
- Captures and returns to patients something about what they have just said (rephrasing one or two ideas)
- They do not have to be accurate (could be amplified or exaggerated) and may or may not introduce new meaning.
- Different types of complex reflections: adding content or meaning, amplification, double-sided, reframing, verbalizing unspoken emotion, emphasizing one side
- Roll with resistance: When patients display signs of resistance, such as blaming or minimizing, the practitioner lets the resistance flow rather than use oppositional tactics, such as telling the person he is wrong.
- Using a rating scale, one a scale of 1–10, Importance***Confidence*** Using a numerical rating scale or other ruler to assess the patient’s attitude toward importance and confidence behind changing a certain behavior. Typically asked as: “Could you tell me, on a scale from 1 to 10, how important it is for you to _____? Why did you give yourself a score of __ and not 1?” The same style question can be asked about confidence. Could follow up with a question such as “How can I help you move higher up the scale?” These types of questions will help support self-efficacy.
- Elicit change talk:
- Explore how their current behavior is inconsistent with their values.
- Selectively asking and identifying when patients state desire, ability, reasons for, and the need to change and responding to this by evoking, affirming, and reflecting these back to them.
References
- Ramalho de Oliveira, D.; Brummel, A.R.; Miller, D.B. Medication Therapy Management: 10 years of experience in a large integrated health care system. J. Manag. Care Pharm. 2010, 16, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Isetts, B.J.; Schondelmeyer, S.W.; Artz, M.B.; Lenarz, L.A.; Heaton, A.H.; Wadd, W.B.; Brown, L.M.; Cipolle, R.J. Clinical and economic outcomes of medication therapy management services: The Minnesota experience. J. Am. Pharm. Assoc. 2008, 48, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Cipolle, R.J.; Strand, L.M.; Morley, P.C. Pharmaceutical Care Practice: The Clinician’s Guide, 2nd ed.; McGraw-Hill: New York, NY, USA, 2004. [Google Scholar]
- Cipolle, R.J.; Strand, L.M.; Morley, P.C. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management, 3rd ed.; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Shoemaker, S.J.; Ramalho de Oliveira, D. Understanding the meaning of medications for patients: The medication experience. Pharm. World Sci. 2008, 30, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Shoemaker, S.J.; Ramalho de Oliveira, D.; Alves, M.; Ekstrand, M. The medication experience: Preliminary evidence of its value for patient education and counseling on chronic medications. Patient Educ. Couns. 2011, 83, 443–450. [Google Scholar] [CrossRef]
- Ramalho de Oliveira, D.; Shoemaker, S.J.; Ekstrand, M.; Alves, M.R. Preventing and resolving drug therapy problems by understanding patients’ medication experiences. J. Am. Pharm. Assoc. 2012, 52, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Moen, J.; Bohm, A.; Tillenius, T.; Antonov, K.; Nilsson, J.L.; Ring, L. “I don’t know how many of these [medicines] are necessary.”—A focus group study among elderly users of multiple medicines. Patient Educ. Couns. 2009, 74, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Alfano, G. The older adult and drug therapy: Part two. Meaning of the medication: Clue to acceptance or rejection. Geriatr. Nurs. 1982, 3, 28–30. [Google Scholar] [CrossRef]
- Seale, C.; Champlin, R.; Lelliot, P.; Quirk, A. Antipsychotic medication, sedation and mental clouding: An observational study of psychiatric consultations. Soc. Sci. Med. 2007, 65, 698–711. [Google Scholar] [CrossRef] [PubMed]
- Sim, M.G.; Wain, T.; Khong, E. Influencing behavior change in general practice; Part 1 brief intervention and motivational interviewing. Aust. Fam. Physician 2009, 38, 885–888. [Google Scholar] [PubMed]
- Rollnick, S.; Miller, W.; Butler, C. Motivational Interviewing in Health Care; Helping Patients Change Behavior; The Guilford Press: New York, NY, USA, 2008. [Google Scholar]
- Sim, M.G.; Wain, T.; Khong, E. Influencing behavior change in general practice; Part 2 motivational interviewing approaches. Aust. Fam. Physician 2009, 38, 986–989. [Google Scholar] [PubMed]
- PCPCC Medication Management Task Force. The Patient-Centered Medical Home: Integrating Comprehensive Medication Management to Optimize Patient Outcomes, 2nd ed.; Patient-Centered Primary Care Collaborative: Washington, DC, USA, 2012. [Google Scholar]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research; SAGE: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Droege, M. The role of reflective practice in pharmacy. Educ. Health 2003, 1, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Ramalho de Oliveira, D.; Shoemaker, S.J. Achieving patient centeredness in pharmacy practice: Openness and the pharmacist’s natural attitude. J. Am. Pharm. Assoc. 2006, 46, 56–66. [Google Scholar] [CrossRef]
- Ramalho-de-Oliveira, D. Autoethnography—Overview and its Prospect to Advance Pharmacy Education and Practice. Am. J. Pharm. Educ. 2019. [Google Scholar] [CrossRef]
- Possidente, C.J.; Bucci, K.K.; McClain, W.J. Motivational interviewing: A tool to improve medication adherence? Am. J. Health Syst. Pharm. 2005, 62, 1311–1314. [Google Scholar] [CrossRef] [PubMed]
- Rubak, S.; Sandbaek, A.; Lauritzen, T.; Christensen, B. Motivational interviewing: A systematic review and meta-analysis. Br. J. Gen. Pract. 2005, 55, 305–312. [Google Scholar] [PubMed]
- Oliveira, I.V.; Freitas, E.L.; Detoni, K.B.; Ramalho-de-Oliveira, D. Use of the patient’s medication experience in pharmacists’ decision making process. Int. J. Pharm. 2017, 7, 1–8. [Google Scholar]
- Nascimento, Y.d.A.; Silva, L.D.; Ramalho-de-Oliveira, D. Experiences with the daily use of medications among chronic hepatitis c patients. Res. Soc. Adm. Pharm. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Levensky, E.R.; Forcehimes, A.; O’Donohue, W.T.; Beitz, K. Motivational interviewing; An evidence-based approach to counseling helps patients follow treatment recommendations. Am. J. Nurs. 2007, 107, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Behner, P.; Klink, A.; Visser, S.; Böcken, J.; Etgeton, S. Unleashing the Potential of Therapy Adherence; High Leverage Changes in Patient Behavior for Improved Health and Productivity; Booz & Company: Amsterdam, The Netherlands, 2012. [Google Scholar]


{kind=link}
| Focus Group 1 | Focus Group 2 |
|---|---|
| |
|
|
|
|
| |
| |
| |
| |
| |
| Round 1 | Round 2 | |
|---|---|---|
| Tool Version | Tool v1 | Tool v2 |
| Testing Duration | 7 weeks | 8 weeks |
| Pharmacists | 10 RPhs | 10 RPhs (same as Round1) |
| Pharmacists’MTM experience | 4 months–15 years | 4 months–15 years |
| # of Patient encounters | 620 | 649 |
| # (%) Patient encounters pharmacists used Tool | 180 (29%) | 227 (35%) |
| Changes to the Tool | ||
| Changes to the Medication Experiences |
|
|
| Changes to Strategies |
|
|
| Most Common Medication Experiences (Med Exp) | Medication Experiences N (%) | MI Strategies Used (% for each Med Exp) | |||||
|---|---|---|---|---|---|---|---|
| Raise Concern, Educate or Inform | Collaboration/SDM | Open-Ended Question | Support Autonomy | Roll With Resistance | Negotiate | ||
| Self-adjusts medication regimen (increases, decrease, or skips doses) | 31 (15%) | 87% | 77% | 77% | 52% | 19% | 19% |
| Feelings of burden and being overwhelmed (e.g., pill burden) | 27 (13%) | 93% | 78% | 67% | 56% | 41% | 37% |
| Fears/concerns about side effects: History of personal side effects. | 23 (11%) | 91% | 87% | 70% | 35% | 30% | 26% |
| Fears/concerns about side effects: Current personal side effects. | 17 (8%) | 76% | 82% | 76% | 65% | 18% | 35% |
| Prefers alternative non-drug therapy or lifestyle changes. | 16 (8%) | 81% | 88% | 88% | 44% | 6% | 6% |
| Fear of not having medication(s)/(security). | 10 (5%) | 80% | 90% | 70% | 60% | 40% | 20% |
| Does not want to take medications: Does not like to take them (cultural background, other). | 10 (5%) | 90% | 80% | 70% | 50% | 40% | 20% |
| Other Experiences. | 72 (35%) | ||||||
| Total | 206 (100%) | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Redmond, S.; Paterson, N.; Shoemaker-Hunt, S.J.; Ramalho-de-Oliveira, D. Development, Testing and Results of a Patient Medication Experience Documentation Tool for Use in Comprehensive Medication Management Services. Pharmacy 2019, 7, 71. https://doi.org/10.3390/pharmacy7020071
Redmond S, Paterson N, Shoemaker-Hunt SJ, Ramalho-de-Oliveira D. Development, Testing and Results of a Patient Medication Experience Documentation Tool for Use in Comprehensive Medication Management Services. Pharmacy. 2019; 7(2):71. https://doi.org/10.3390/pharmacy7020071
Chicago/Turabian StyleRedmond, Stephanie, Nicole Paterson, Sarah J. Shoemaker-Hunt, and Djenane Ramalho-de-Oliveira. 2019. "Development, Testing and Results of a Patient Medication Experience Documentation Tool for Use in Comprehensive Medication Management Services" Pharmacy 7, no. 2: 71. https://doi.org/10.3390/pharmacy7020071
APA StyleRedmond, S., Paterson, N., Shoemaker-Hunt, S. J., & Ramalho-de-Oliveira, D. (2019). Development, Testing and Results of a Patient Medication Experience Documentation Tool for Use in Comprehensive Medication Management Services. Pharmacy, 7(2), 71. https://doi.org/10.3390/pharmacy7020071