The Development and Proof of Principle Test of TRIAGE: A Practical Question Set to Identify and Discuss Medication-Related Problems in Community Pharmacy



Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of TRIAGE
2.1.1. Literature
2.1.2. Input from Steering Committee and Pharmacy Team Members
2.1.3. Pre-Test
2.1.4. Incorporation in Pharmaceutical Care Program
2.2. Evaluation of TRIAGE in Community Pharmacies
2.2.1. Setting
2.2.2. Patients
2.2.3. Procedure
2.2.4. PTs’ and Patients’ Experiences with TRIAGE
3. Results
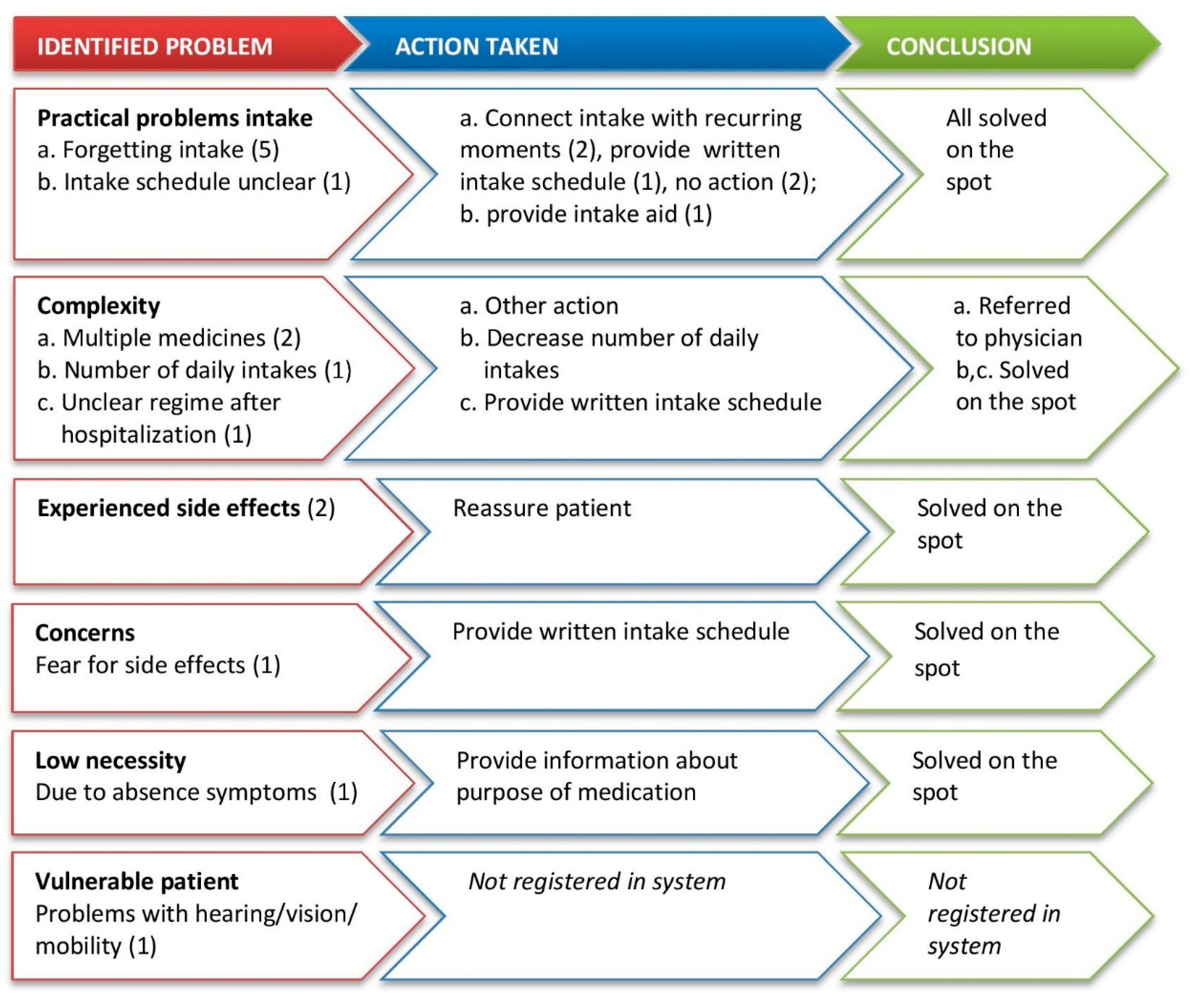
3.1. Identified Problems in TRIAGE Conversations
3.2. PTs’ Experiences with TRIAGE
3.3. Patients’ Experiences with TRIAGE
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice and Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kardas, P.; Lewek, P.; Matyjaszczyk, M. Determinants of patient adherence: A review of systematic reviews. Front. Pharm. 2013, 4, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conn, V.S.; Ruppar, T.M. Medication adherence outcomes of 771 intervention trials: Systematic review and meta-analysis. Prev. Med. 2017, 99, 269–276. [Google Scholar] [CrossRef]
- van der Laan, D.M.; Elders, P.J.M.; Boons, C.C.L.M.; Nijpels, G.; Hugtenburg, J.G. Factors Associated with Nonadherence to Cardiovascular Medications: A Cross-sectional Study. J. Cardiovasc. Nurs. 2019, 34, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Leslie, K.H.; McCowan, C.; Pell, J.P. Adherence to cardiovascular medication: A review of systematic reviews. J. Public Health (Oxf.) 2019, 41, e84–e94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilhelmsen, N.C.; Eriksson, T. Medication adherence interventions and outcomes: An overview of systematic reviews. Eur. J. Hosp. Pharm. 2019, 26, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allemann, S.S.; van Mil, J.W.; Botermann, L.; Berger, K.; Griese, N.; Hersberger, K.E. Pharmaceutical care: The PCNE definition 2013. Int. J. Clin. Pharm. 2014, 36, 544–555. [Google Scholar] [CrossRef] [PubMed]
- Aslani, P.; Ahmed, R.; da Costa, F.A. The Role of Adherence in Pharmaceutical Care. In The Pharmacist Guide to Implementing Pharmaceutical Care; Alves da Costa, F., van Mil, J., Alvarez-Risco, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar] [CrossRef]
- Lamberts, E.J.; Bouvy, M.L.; van Hulten, R.P. The role of the community pharmacist in fulfilling information needs of patients starting oral antidiabetics. Res. Social Adm. Pharm. 2010, 6, 354–364. [Google Scholar] [CrossRef]
- Koster, E.S.; van Meeteren, M.M.; van Dijk, M.; van de Bemt, B.J.; Ensing, H.T.; Bouvy, M.L.; Blom, L.; van Dijk, L. Patient-provider interaction during medication encounters: A study in outpatient pharmacies in the Netherlands. Patient Educ. Couns. 2015, 98, 843–848. [Google Scholar] [CrossRef] [Green Version]
- Van Dijk, M.; Blom, L.; Koopman, L.; Philbert, D.; Koster, E.; Bouvy, M.L.; van Dijk, L. Patient-provider communication about medication use at the community pharmacy counter. Int. J. Pharm. Pract. 2016, 24, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Olsson, E.; Ingman, P.; Ahmed, B.; Kälvemark Sporrong, S. Pharmacist-patient communication in Swedish community pharmacies. Res. Soc. Adm. Pharm. 2014, 10, 149–155. [Google Scholar] [CrossRef]
- Driesenaar, J.A.; De Smet, P.A.; van Hulten, R.; Hu, L.; van Dulmen, S. Communication during counseling sessions about inhaled corticosteroids at the community pharmacy. Patient Prefer. Adherence 2016, 10, 2239–2254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhill, N.; Anderson, C.; Avery, A.; Pilnick, A. Analysis of pharmacist-patient communication using the Calgary-Cambridge guide. Patient Educ. Couns. 2011, 83, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.G.; Lee, N.E.; Sohn, H.S. Gap between patient expectation and perception during pharmacist–patient communication at community pharmacy. Int. J. Clin. Pharm. 2020, 42, 677–684. [Google Scholar] [CrossRef]
- Stevenson, F.A.; Cox, K.; Britten, N.; Dundar, Y. A systematic review of the research on communication between patients and health care professionals about medicines: The consequences for concordance. Health Expect. 2004, 7, 235–245. [Google Scholar] [CrossRef]
- Linn, A.J.; Van Weert, J.C.M.; Smit, E.G.; Schouten, B.; Van Bodegraven, A.A.; Van Dijk, L. Words That Make Pills Easier to Swallow. The Development of a Communication Typology to Address Practical and Perceptual Barriers to Medication Intake Behavior. Patient Prefer. Adherence 2012, 6, 871–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Society of Health-System Pharmacists. ASHP guidelines on pharmacist-conducted patient education and counseling. Am. J. Health Syst. Pharm. 1997, 54, 431–434. [Google Scholar] [CrossRef]
- Royal Pharmaceutical Society. Pharmacy Guide on Counselling Patients on Medicines. Available online: https://www.rpharms.com/resources/quick-reference-guides/counselling-patients-on-medicines (accessed on 15 May 2020).
- KNMP. Pharmaceutical Consultation, concept guideline. 2019. Available online: https://www.knmp.nl/praktijkvoering/richtlijnen/knmp-richtlijnen-farmaceutische-zorg/consultvoering-1 (accessed on 4 May 2020).
- Kurtz, S.; Silverman, J.; Benson, J.; Draper, J. Marrying content and process in clinical method teaching: Enhancing the Calgary-Cambridge guides. Acad. Med. 2003, 78, 802–809. [Google Scholar] [CrossRef]
- Silverman, J.D.; Kurtz, S.M.; Draper, J. Skills for Communicating with Patients; Radcliffe Medical Press: Oxford, UK, 1998. [Google Scholar]
- Gardner, M.; Boyce, R.; Herrier, R. Pharmacist-Patient Consultation Program: An Interactive Approach to Verify Patient Understanding. Public Health Service, Indian Health Service/Roerig Division of Pfizer Pharmaceuticals: Rockville, MD, USA, 1991. [Google Scholar]
- Pringle, J.L.; Boyer, A.; Conklin, M.H.; McCullough, J.W.; Aldridge, A. The Pennsylvania Project: Pharmacist intervention improved medication adherence and reduced health care costs. Health Aff. (Millwood) 2014, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Feifer, R.A.; Greenberg, L.; Rosenberg-Brandl, S.; Franzblau-Isaac, E. Pharmacist counseling at the start of therapy: Patient receptivity to offers of in-person and subsequent telephonic clinical support. Popul. Health Manag. 2010, 13, 189–193. [Google Scholar] [CrossRef]
- Kuipers, E.; Wensing, M.; De Smet, P.A.; Teichert, M. Exploring patient’s perspectives and experiences after start with inhalation maintenance therapy: A qualitative theory-based study. Patient Prefer. Adherence 2020, 14, 203–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrijens, B.; Antoniou, S.; Burnier, M.; de la Sierra, A.; Volpe, M. Current situation of medication adherence in hypertension. Front Pharm. 2017, 8, 100. [Google Scholar] [CrossRef] [Green Version]
- Hommel, K.A.; McGrady, M.E.; Peugh, J.; Zacur, G.; Loreaux, K.; Saeed, S.; Williams, E.; Denson, L.A. Longitudinal Patterns of Medication Nonadherence and Associated Health Care Costs. Inflamm. Bowel Dis. 2017, 23, 1577–1583. [Google Scholar] [CrossRef] [PubMed]
- Hattingh, H.L.; Emmerton, L.; Ng Cheong Tin, P.; Green, C.; Kardas, P.; Lewek, P.; Matyjaszczyk, M. Utilization of community pharmacy space to enhance privacy: A qualitative study. Health Expect. 2016, 19, 1098–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zolnierek, K.B.; Dimatteo, M.R. Physician communication and patient adherence to treatment: A meta-analysis. Med. Care 2009, 47, 826–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Problem Domains |
|---|
| 1. Practical intake problems; |
| 2. Problems with incorporating intake in daily routine; |
| 3. Complexity of the medication (regime); |
| 4. Experienced side effects; |
| 5. Perceived low necessity of the medication; |
| 6. Concerns about the medication; |
| 7. Knowledge barriers; |
| 8. Costs; |
| 9. Vulnerable patients who are unable to understand or apply information; |
| 10. Social support. |
| Opening Questions | Follow-Up Questions |
|---|---|
| 1. I am curious about your experiences. How have you been taking this medicine lately? | Suggestions for first refill:
Suggestions for follow-up refill:
Can you tell me more about that?
|
| 2. Any medication can also have side effects. How’s that for you? Do you experience side effects of this medicine? | Suggestion for first and follow-up refill:
|
| 3. How do you feel about using this medicine (long-term)? | Suggestions for first and follow-up refill:
Suggestion for specific for follow-up refill:
|
| 4. Which questions do you still have? | Refer to additional, reliable information about the medicine. |
| Pharmacy | First Refill | Follow-Up Refill | Total |
|---|---|---|---|
| 1 | 8 | 7 | 15 |
| 2 | 7 | 7 | 14 |
| 3 | 8 | 3 | 11 |
| 4 | 11 | 12 | 23 |
| 5 | 13 | 7 | 20 |
| 6 | 8 | 1 | 9 |
| 7 | 1 | 0 | 1 |
| 8 | 4 | 1 | 5 |
| 9 | 5 | 1 | 6 |
| 10 | 1 | 0 | 1 |
| Total | 66 | 39 | 105 |
| Aspects of the TRIAGE Conversation | First Refill | Follow-Up Refill |
|---|---|---|
| Number of questions asked | (n = 37) | (n = 24) |
| All 4 questions | 20 (54%) | 6 (25%) |
| 3 questions | 7 (19%) | 4 (17%) |
| 2 questions | 6 (16%) | 4 (17%) |
| 1 question | 4 (11%) | 10 (42%) |
| Length of TRIAGE conversation | ||
| <5 min | 27 (79%) | 13 (72%) |
| 5–10 min | 6 (18%) | 3 (17%) |
| >10 min | 1 (3%) | 2 (11%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vervloet, M.; Zwikker, H.E.; Linn, A.J.; Koster, E.S.; Gipmans, S.G.H.; van Aarle, M.C.W.; van Dijk, L. The Development and Proof of Principle Test of TRIAGE: A Practical Question Set to Identify and Discuss Medication-Related Problems in Community Pharmacy. Pharmacy 2020, 8, 178. https://doi.org/10.3390/pharmacy8040178
Vervloet M, Zwikker HE, Linn AJ, Koster ES, Gipmans SGH, van Aarle MCW, van Dijk L. The Development and Proof of Principle Test of TRIAGE: A Practical Question Set to Identify and Discuss Medication-Related Problems in Community Pharmacy. Pharmacy. 2020; 8(4):178. https://doi.org/10.3390/pharmacy8040178
Chicago/Turabian StyleVervloet, Marcia, Hanneke E. Zwikker, Annemiek J. Linn, Ellen S. Koster, Suzan G. H. Gipmans, Maaike C. W. van Aarle, and Liset van Dijk. 2020. "The Development and Proof of Principle Test of TRIAGE: A Practical Question Set to Identify and Discuss Medication-Related Problems in Community Pharmacy" Pharmacy 8, no. 4: 178. https://doi.org/10.3390/pharmacy8040178
APA StyleVervloet, M., Zwikker, H. E., Linn, A. J., Koster, E. S., Gipmans, S. G. H., van Aarle, M. C. W., & van Dijk, L. (2020). The Development and Proof of Principle Test of TRIAGE: A Practical Question Set to Identify and Discuss Medication-Related Problems in Community Pharmacy. Pharmacy, 8(4), 178. https://doi.org/10.3390/pharmacy8040178