Can We Create a Circular Pharmaceutical Supply Chain (CPSC) to Reduce Medicines Waste?



_Sivarajah.jpg)
Abstract
:1. Introduction
- pathological; this includes body parts, body fluids, human waste, and tissue waste and animal corpses that are contaminated;
- pharmaceutical; this is either unused, contaminated medicine or medicine which has expired;
- cytotoxic; genotoxic waste (highly hazardous);
- sharps; includes syringes, needles, and blades, etc.;
- infectious; this usually contains blood or any bodily fluid which is contaminated and could, therefore, infect other people when they come into contact;
- non-hazardous; these waste materials can not cause any chemical, radioactive, biological, or physical dangers; and,
- radioactive; products that are infected by radionuclides.
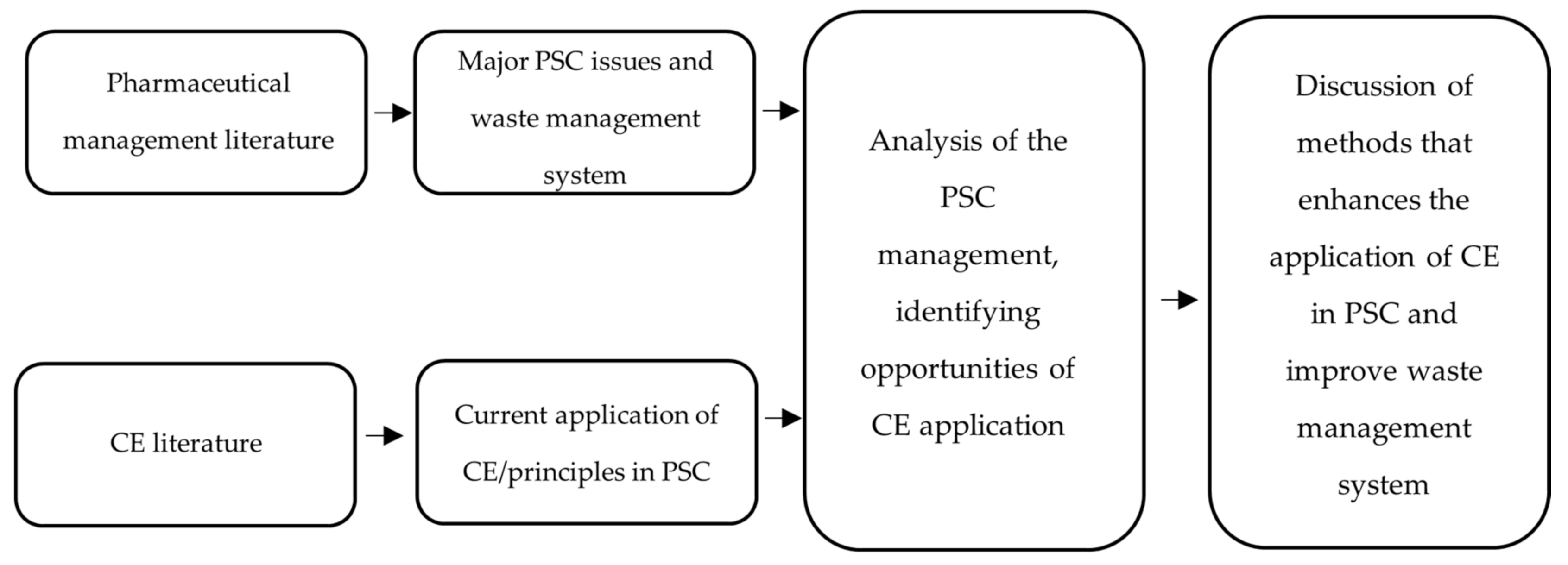
2. Materials and Methods
3. Results
3.1. Pharmaceutical Waste Management
3.1.1. Waste Creation
3.1.2. Waste Management
3.1.3. Waste Disposal
3.1.4. Waste Reuse and Recycling
3.1.5. Obstacles to the Safety and Quality of Returned Pharmaceuticals
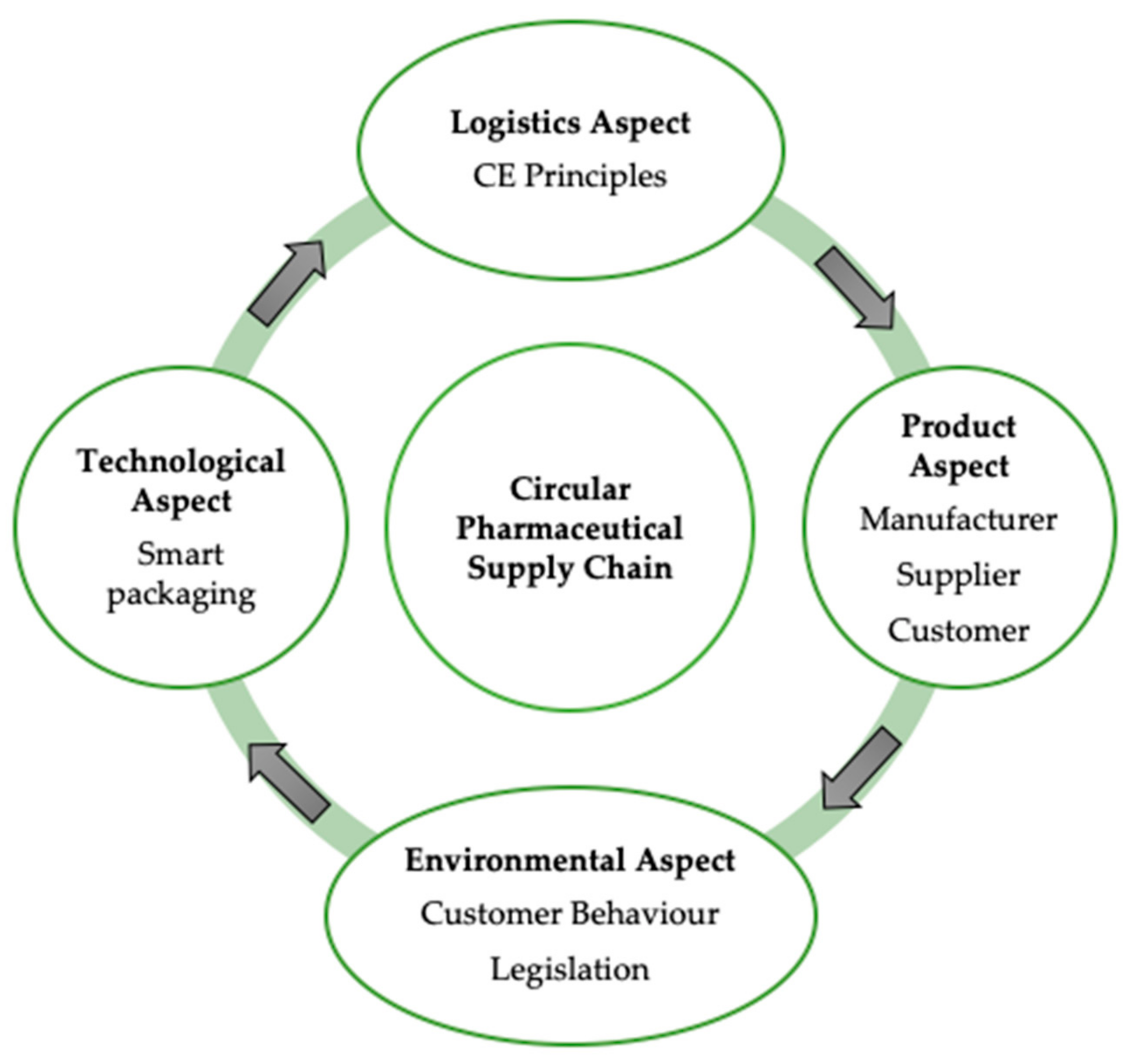
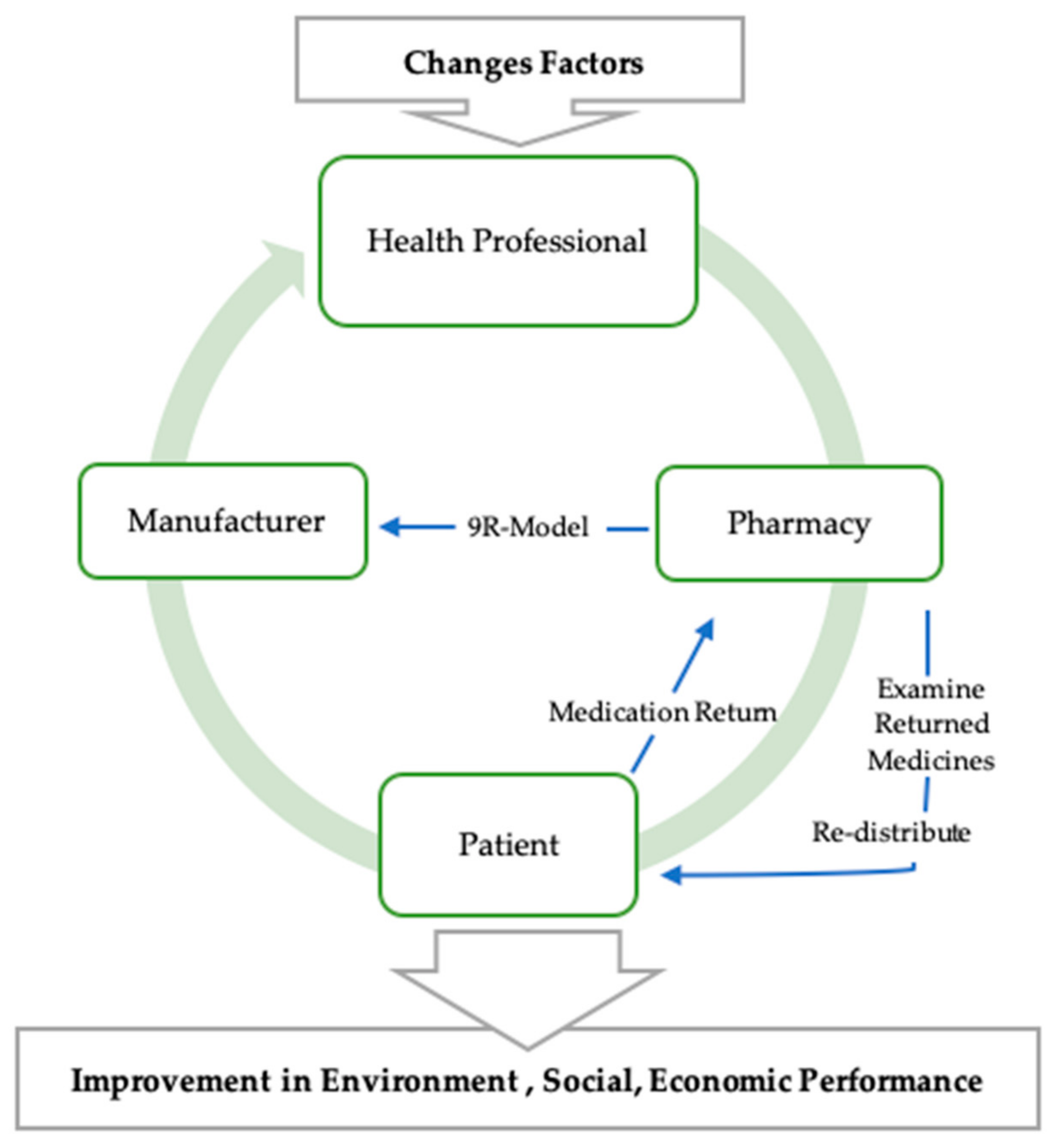
3.2. Circular Economy and the Management of Pharmaceutical Waste
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Guidelines for Safe Disposal of Unwanted Pharmaceuticals in and After Emergencies. 1999. Available online: https://www.who.int/water_sanitation_health/medicalwaste/unwantpharm.pdf (accessed on 1 March 2020).
- Hui, T.; Mohammed, B.; Donyai, P.; McCrindle, R.; Sherratt, R. Enhancing Pharmaceutical Packaging through a Technology Ecosystem to Facilitate the Reuse of Medicines and Reduce Medicinal Waste. Pharmacy 2020, 8, 58. [Google Scholar] [CrossRef] [Green Version]
- PSNC. Essential Facts, Stats and Quotes Relating to Prescriptions. 2014. Available online: https://psnc.org.uk/services-commissioning/essential-facts-stats-and-quotes-relating-to-prescriptions/ (accessed on 7 June 2020).
- Statista. Global Spending on Medicines 2024 Forecast|Statista, Statista. 2020. Available online: https://www.statista.com/statistics/280572/medicine-spending-worldwide/ (accessed on 27 May 2020).
- Clark, D. Regional Expenditure on Health 2019 Statistic|Statista. 2019. Available online: https://www.statista.com/statistics/651514/identifiable-expenditure-on-health-by-region-united-kingdom/ (accessed on 24 October 2020).
- Gebremariam, E.T.; Gebregeorgise, D.T.; Fenta, T.G. Factors contributing to medicines wastage in public health facilities of South West Shoa Zone, Oromia Regional State, Ethiopia: A qualitative study. J. Pharm. Policy Pract. 2019, 12, 1–7. [Google Scholar] [CrossRef]
- WHO Health-Care Waste. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 23 October 2020).
- Bungau, S.; Tit, D.M.; Fodor, K.; Cioca, G.; Agop, M.; Iovan, C.; Nistor-Cseppento, D.C.; Bumbu, A.; Bustea, C. Aspects Regarding the Pharmaceutical Waste Management in Romania. Sustainability 2018, 10, 2788. [Google Scholar] [CrossRef] [Green Version]
- Kane, G.; Bakker, C.; Balkenende, A. Towards design strategies for circular medical products. Resour. Conserv. Recycl. 2018, 135, 38–47. [Google Scholar] [CrossRef]
- Delahaye, R.; Hoekstra, R.; Ganzevles, J.; Lijzen, J.; Potting, J.; Hanemaaijer, A. Circular Economy: What we Want to Know and Can Measure Framework and Baseline Assessment for Monitoring the Progress of the Circular Economy in the Netherlands; PBL: Hague, The Netherlands, 2018. [Google Scholar]
- Manavalan, E.; Jayakrishna, K. An Analysis on Sustainable Supply Chain for Circular Economy. Procedia Manuf. 2019, 33, 477–484. [Google Scholar] [CrossRef]
- Kirchherr, J.; Reike, D.; Hekkert, M. Conceptualizing the circular economy: An analysis of 114 definitions. Resour. Conserv. Recycl. 2017, 127, 221–232. [Google Scholar] [CrossRef]
- MacArthur. Towards the Circular Economy, Ellenmacarthurfoundation.org. 2020. Available online: https://www.ellenmacarthurfoundation.org/assets/downloads/publications/Ellen-MacArthur-Foundation-Towards-the-Circular-Economy-vol.1.pdf (accessed on 3 March 2020).
- United Nation. Sufficient Economy Philosophy—United Nations Partnerships for SDGs Platform. 2012. Available online: https://sustainabledevelopment.un.org/partnership/?p=2126 (accessed on 17 August 2020).
- Mongsawad, P. The philosophy of the sufficiency economy: A contribution to the theory of development. Asia Pac. Dev. J. 2012, 17, 123–143. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Palsule-Desai, O.D. Sustainable Supply Chain Management: Review and Research Opportunities. IIMB Manag. Rev. 2011, 23, 195. [Google Scholar] [CrossRef] [Green Version]
- European Parliament. Circular Economy: Definition, Importance and Benefits|News|European Parliament. 2018. Available online: https://www.europarl.europa.eu/news/en/headlines/economy/20151201STO05603/circular-economy-definition-importance-and-benefits (accessed on 27 July 2020).
- Grdic, Z.S.; Nizic, M.K.; Rudan, E. Circular Economy Concept in the Context of Economic Development in EU Countries. Sustainability 2020, 12, 3060. [Google Scholar] [CrossRef] [Green Version]
- Smol, M.; Marcinek, P.; Duda, J.; Szołdrowska, D. Correction: Smol, M., et al. Importance of Sustainable Mineral Resource Management in Implementing the Circular Economy (CE) Model and the European Green Deal Strategy. Resource 2020, 9, 55. Resources 2020, 9, 78. [Google Scholar] [CrossRef]
- GE Healthcare. GoldSeal Refurbished Imaging Systems Reliable Quality. Certified Confidence. www3.gehealthcare.com. 2012. Available online: http://www3.gehealthcare.in/~/media/documents/us-global/products/goldseal-refurbished/brochures/gehealthcare-brochure_goldseal_refurbished-imaging-systems.pdf (accessed on 12 August 2020).
- Philips. Addressing Healthcare Challenges Through Innovation. 2018. Available online: https://www.philips.com/static/annualresults/2017/PhilipsFullAnnualReport2017-English.pdf (accessed on 12 August 2020).
- WHO. The World Medicines Situation 2011 Rational Use of Medicines. 2011. Available online: https://www.who.int/medicines/areas/policy/world_medicines_situation/WMS_ch14_wRational.pdf (accessed on 23 May 2020).
- Narwat, A.; Sindhu, A. Practice towards disposal of medicines (unused/expired drugs) among the patients visiting tertiary care teaching hospital in Haryana, India. Int. J. Res. Med. Sci. 2019, 7, 3050. [Google Scholar] [CrossRef]
- FDA. Drug Shortages: Root Causes and Potential Solutions. 2020. Available online: https://www.fda.gov/media/131130/download (accessed on 1 August 2020).
- Bohmer, R.; Pisano, G.; Sadun, R.; Tsai, T. How Hospitals Can Manage Supply Shortages as Demand Surges. 2020. Available online: https://hbr.org/2020/04/how-hospitals-can-manage-supply-shortages-as-demand-surges (accessed on 2 August 2020).
- Ali, A. Inventory Management in Pharmacy Practice: A Review of Literature. J. Pharm. Pract. 2011, 2, 151–156. [Google Scholar]
- Khan, S.A.; Arora, D.S.; Mey, A.; Maganlal, S. Provision of pharmaceutical care in patients with limited English proficiency: Preliminary findings. J. Res. Pharm. Pract. 2015, 4, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Shafaat, K.; Yadav, V.; Kumar, B. An overview: Storage of Pharmaceutical Products. J. Pharm. Pharm. Sci. 2013, 2, 2499–2513. [Google Scholar]
- Mayimele, N.; Meyer, H.; Schellack, N. What role does the pharmacist play in medicine management at ward level? SA Pharm. J. 2015, 82, 33–36. [Google Scholar]
- Ofori-Asenso, R.; Agyeman, A.A. Irrational Use of Medicines—A Summary of Key Concepts. Pharmacy 2016, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Makki, M.; Hassali, M.A.; Awaisu, A.; Hashmi, F.K. The Prevalence of Unused Medications in Homes. Pharmacy 2019, 7, 61. [Google Scholar] [CrossRef] [Green Version]
- NHS. Medicines Re-use Pathway. 2020. Available online: https://www.leeds.gov.uk/docs/medicines%20reuse%20pathway%20and%20FAQs.pdf (accessed on 2 August 2020).
- NHS. Medicines Policy Version 17. 2019. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjuw-WRkYLrAhVNqxoKHQ5qBe8QFjAAegQIBRAB&url=https%3A%2F%2Fwww.southernhealth.nhs.uk%2F_resources%2Fassets%2Fattachment%2Ffull%2F0%2F44372.pdf&usg=AOvVaw3WfBxx01PpYUC1uJmq8OI8 (accessed on 1 August 2020).
- NHS. Moving Medicines Safely: Implementing and Sustaining a ‘Green Bag’ Schem. 2020. Available online: https://www.sps.nhs.uk/wp-content/uploads/2015/12/Moving_Meds_Safely-Imp_a_Green_Bag_Scheme_Vs-2.2.pdf (accessed on 1 August 2020).
- NICE. Recommendations|Controlled Drugs: Safe Use and Management|Guidance|NICE. 2016. Available online: https://www.nice.org.uk/guidance/ng46/chapter/recommendations (accessed on 1 August 2020).
- NHS. Stopping Managed Repeats. 2019. Available online: https://midessexccg.nhs.uk/livewell/your-medicines-your-nhs/reducing-medicines-waste/increasing-erds-and-stopping-managed-repeats/3531-1-practice-frequently-asked-questions-stopping-managed-repeats-december-2019/file (accessed on 1 August 2020).
- Royal College of Nursing. COVID-19 Remote Prescribing|Medicines Management|Royal College of Nursing. 2020. Available online: https://www.rcn.org.uk/clinical-topics/medicines-management/covid-19-remote-prescribing (accessed on 1 August 2020).
- Amaral, M.; Fop, L. Unused Pharmaceuticals Where Do They End up? 2013. Available online: https://noharm-europe.org/sites/default/files/documents-files/4646/2013-12%20Unused%20pharmaceuticals.pdf (accessed on 4 August 2020).
- Michael, I.; Ogbonna, B.O.; Sunday, N.; Anetoh, M.; Matthew, O. Assessment of disposal practices of expired and unused medications among community pharmacies in Anambra State southeast Nigeria: A mixed study design. J. Pharm. Policy Pract. 2019, 12, 12. [Google Scholar] [CrossRef]
- Dyer, C. Coroner warns about poor drug reviews after patient dies from tramadol overdose. BMJ 2020, 370. [Google Scholar] [CrossRef]
- Hazell, B.; Robson, R. Pharmaceutical waste reduction in the NHS. Rep. Version 2015, 1, 6–23. [Google Scholar]
- McGuire, M.J.; Iuga, A.O. Adherence and health care costs. Risk Manag. Healthc. Policy 2014, 7, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- York Health Economics Consortium. Evaluation of the Scale Causes and Costs of Waste Medicines. 2010. Available online: https://discovery.ucl.ac.uk/id/eprint/1350234/1/Evaluation_of_NHS_Medicines_Waste__web_publication_version.pdf (accessed on 14 May 2020).
- Royal College of Physicians. Less Waste, more Health: A Health Professional’s Guide to Reducing Waste, RCP London. 2016. Available online: https://www.rcplondon.ac.uk/projects/outputs/less-waste-more-health-health-professionals-guide-reducing-waste (accessed on 19 May 2020).
- Dilokthornsakul, P.; Chaiyakunapruk, N.; Nimpitakpong, P.; Jeanpeerapong, N.; Jampachaisri, K.; Lee, T.A. Understanding medication oversupply and its predictors in the outpatient departments in Thailand. BMC Health Serv. Res. 2014, 14, 408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhamad, H.; Patel, N.; Donyai, P. How do people conceptualize the reuse of medicines? An interview study. Int. J. Pharm. Pract. 2017, 26, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Albaroodi, K. Pharmacists’ Knowledge Regarding Drug Disposal in Karbala. Pharmacy 2019, 7, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alnahas, F.; Yeboah, P.; Fliedel, L.; Abdin, A.Y.; Alhareth, K. Expired Medication: Societal, Regulatory and Ethical Aspects of a Wasted Opportunity. Int. J. Environ. Res. Public Health 2020, 17, 787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abahussain, E.; Waheedi, M.; Koshy, S. Practice, awareness and opinion of pharmacists toward disposal of unwanted medications in Kuwait. Saudi Pharm. J. 2012, 20, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Johnson, K.M.; González, M.L.; Dueñas, L.; Gamero, M.; Relyea, G.; Luque, L.E.; Caniza, M.A. Improving waste segregation while reducing costs in a tertiary-care hospital in a lower–middle-income country in Central America. Waste Manag. Res. 2013, 31, 733–738. [Google Scholar] [CrossRef]
- Zhang, A.; Venkatesh, V.; Liu, Y.; Wan, M.; Qu, T.; Huisingh, D. Barriers to smart waste management for a circular economy in China. J. Clean. Prod. 2019, 240, 118198. [Google Scholar] [CrossRef] [Green Version]
- White, K. UK interventions to control medicines wastage: A critical review. Int. J. Pharm. Pract. 2010, 18, 131–140. [Google Scholar]
- Boxall, A.B.A. The environmental side effects of medication. EMBO Rep. 2004, 5, 1110–1116. [Google Scholar] [CrossRef] [Green Version]
- McRae, D.; Allman, M.; James, D. The redistribution of medicines: Could it become a reality? Int. J. Pharm. Pract. 2016, 24, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Mbongwe, B.; Mmereki, B.T.; Magashula, A. Healthcare waste management: Current practices in selected healthcare facilities, Botswana. Waste Manag. 2008, 28, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.B.; De Mattos, C.A. Critical Success Factors of a Drug Traceability System for Creating Value in a Pharmaceutical Supply Chain (PSC). Int. J. Environ. Res. Public Health. 2019, 16, 1972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, T.K.L.; Donyai, P.; McCrindle, R.; Sherratt, R.S. Enabling Medicine Reuse Using a Digital Time Temperature Humidity Sensor in an Internet of Pharmaceutical Things Concept. Sensors 2020, 20, 3080. [Google Scholar] [CrossRef]
- WHO Safe Management of Wastes from Health-Care Activities. 2014. Available online: https://www.euro.who.int/__data/assets/pdf_file/0012/268779/Safe-management-of-wastes-from-health-care-activities-Eng.pdf (accessed on 1 August 2020).
- Ayele, Y.; Mamu, M. Assessment of knowledge, attitude and practice towards disposal of unused and expired pharmaceuticals among community in Harar city, Eastern Ethiopia. J. Pharm. Policy Pract. 2018, 11, 27. [Google Scholar] [CrossRef]
- Abahussain, E.A.; Ball, D.E. Disposal of unwanted medicines from households in Kuwait. Pharm. World Sci. 2007, 29, 368–373. [Google Scholar] [CrossRef]
- Rogowska, J.; Zimmermann, A.; Muszyńska, A.; Ratajczyk, W.; Wolska, L. Pharmaceutical Household Waste Practices: Preliminary Findings from a Case Study in Poland. Environ. Manag. 2019, 64, 97–106. [Google Scholar] [CrossRef]
- Abdallah, Q.M.A.; Al-Haddad, M.S.M.; Al-Khathami, O.H.M.; Al-Kherish, O.H.H.; Al-Marri, K.M.T.; Al-Matani, M.F.K.; Al-Rashed, A.M.N. Knowledge, Attitude and Practice towards Discarding Unwanted Household Medicines among Univerisity Students in Western Region, KSA. Int. J. Pharm. 2014, 4, 14–21. [Google Scholar]
- Kheir, N.; El Hajj, M.S.; Wilbur, K.; Kaissi, R.M.L.; Yousif, A. An exploratory study on medications in Qatar homes. Drug Healthc. Patient Saf. 2011, 3, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Bound, J.P.; Voulvoulis, N. Household Disposal of Pharmaceuticals as a Pathway for Aquatic Contamination in the United Kingdom. Environ. Health Perspect. 2005, 113, 1705–1711. [Google Scholar] [CrossRef] [Green Version]
- Law, A.V.; Sakharkar, P.; Zargarzadeh, A.; Tai, B.W.B.; Hess, K.; Hata, M.; Mireles, R.; Ha, C.; Park, T.J. Taking stock of medication wastage: Unused medications in US households. Res. Soc. Adm. Pharm. 2015, 11, 571–578. [Google Scholar] [CrossRef] [PubMed]
- UNEP. Basel Convention on the Control of Transboundary Movements of Hazardous Wastes and Their Disposal. 2014. Available online: https://www.basel.int/portals/4/basel%20convention/docs/text/baselconventiontext-e.pdf (accessed on 1 June 2020).
- WHO. 8 Treatment and Disposal Technologies for Health-Care Waste. 1999. Available online: https://www.who.int/docstore/water_sanitation_health/wastemanag/ch10.htm (accessed on 19 May 2020).
- Bujak, J. Thermal treatment of medical waste in a rotary kiln. J. Environ. Manag. 2015, 162, 139–147. [Google Scholar] [CrossRef]
- Askarany, D.; Franklin-Smith, A.W. Cost benefit analyses of organic waste composting systems through the lens of time driven activity-based costing. J. Appl. Manag. Account. Res. 2014, 12, 59–73. [Google Scholar]
- Lopez, G.; Artetxe, M.; Amutio, M.; Bilbao, J.; Olazar, M. Thermochemical routes for the valorisation of waste polyolefinic plastics to produce fuels and chemicals. A review. Renew. Sustain. Energy Rev. 2017, 73, 346–368. [Google Scholar] [CrossRef]
- Albu, A. Landfilling or Incineration of Waste? Practices for Choosing the Appropriate Solution for Waste Management. Quality—Access to Success. Calitatea 2014, 15, 189. [Google Scholar]
- Janagi, R.; Shah, J.; Maheshwari, D. Scenario of management of medical waste in US and UK: A review. J. Glob. Trends Pharm. Sci. 2015, 6, 2328–2339. [Google Scholar]
- Almuneef, M. Effective medical waste management: It can be done. Am. J. Infect. Control. 2003, 31, 188–192. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. Medical Waste. 2017. Available online: https://www.epa.gov/rcra/medical-waste (accessed on 17 November 2020).
- Australian Government. Safe Disposal of Unwanted Medicines. 2019. Available online: https://www.tga.gov.au/safe-disposal-unwanted-medicines (accessed on 1 August 2020).
- Connelly, D. Should pharmacists be allowed to reuse medicines? Pharm. J. 2018. [Google Scholar] [CrossRef]
- Lubick, N. Drugs in the Environment: Do Pharmaceutical Take-Back Programs Make a Difference? Environ. Health Perspect. 2010, 118, A210–A214. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.Y.C.; Peake, B.M.; Braund, R. Disposal practices for unused medications in New Zealand community pharmacies. J. Prim. Health Care 2011, 3, 197–203. [Google Scholar] [CrossRef]
- Alberta Emerald Foundation. ENVIRx|RxA—Alberta Pharmacists’ Association. 2015. Available online: https://rxa.ca/member-benefits/envirx/ (accessed on 1 August 2020).
- Breen, L. Medicines Optimisation—Extracting the Last Vestiges of Value from Your Medicines. 2016. Available online: https://www.pharman.co.uk/uploads/imagelib/pdfs/Journal_articles_by_issue/JoMO_Sep_2016/Medicines%20Optimisation.pdf (accessed on 14 May 2020).
- Xie, Y.; Breen, L. Greening community pharmaceutical supply chain in UK: A cross boundary approach. Supply Chain Manag. Int. J. 2012, 17, 40–53. [Google Scholar] [CrossRef]
- Raja, S.; Mohapatra, S.; Kalaiselvi, A.; Rani, R.J. Awareness and Disposal Practices of Unused and Expired Medication among Health Care Professionals and Students in a Tertiary Care Teaching Hospital. Biomed. Pharmacol. J. 2018, 11, 2073–2078. [Google Scholar] [CrossRef]
- Hsieh, D.S.; Lindrud, M.; Lu, X.; Zordan, C.; Tang, L.; Davies, M. A Process for Active Pharmaceutical Ingredient Recovery from Tablets Using Green Engineering Technology. Org. Process. Res. Dev. 2017, 21, 1272–1285. [Google Scholar] [CrossRef]
- FDA. Chapter 56 Drug Quality Assurance 2015. Available online: https://www.fda.gov/media/75201/download (accessed on 24 October 2020).
- Gould, H. 7 Things we Learned About Healthcare and the Circular Economy. The Guardian. 24 February 2016. Available online: https://www.theguardian.com/sustainable-business/2016/feb/24/opportunities-challenges-circular-economy-healthcare-live-chat-highlights (accessed on 14 April 2020).
- Urciuoli, L.; Sternberg, H.; Ekwall, D.; Nyquist, C. Exploring security effects on transport performance. Int. J. Shipp. Transp. Logist. 2013, 5, 303. [Google Scholar] [CrossRef]
- Agrawal, Y.K.; Shah, R.Y.; Prajapati, P. Anticounterfeit packaging technologies. J. Adv. Pharm. Technol. Res. 2010, 1, 368–373. [Google Scholar] [CrossRef] [Green Version]
- Kumar, K.; Gupta, V.; Lalasa, P.; Sandhil, S. A Review on Packaging Materials with Anti-Counterfeit, Tamper- Evident Features for Pharmaceuticals. Int. J. Drug Dev. Res. 2013, 5, 26–34. [Google Scholar]
- UK Government. Implementing the Falsified Medicines Directive: Safety Features. 2019. Available online: https://www.gov.uk/guidance/implementing-the-falsified-medicines-directive-safety-features (accessed on 28 August 2020).
- ISO. Packaging—Tamper Verification Features for Medicinal Product Packaging. 2018. Available online: https://www.iso.org/obp/ui/#iso:std:iso:21976:ed-1:v1:en (accessed on 28 August 2020).
- Snell, E. Benefits, Challenges of Secure Healthcare Data Sharing. 2017. Available online: https://healthitsecurity.com/features/benefits-challenges-of-secure-healthcare-data-sharing (accessed on 2 July 2020).
- WHO. WHO Guidelines on Transfer of Technology in Pharmaceutical Manufacturing. 2011. Available online: https://www.who.int/medicines/areas/quality_safety/quality_assurance/TransferTechnologyPharmaceuticalManufacturingTRS961Annex7.pdf?ua=1 (accessed on 1 July 2020).
- WHO. Circular Economy and Health: Opportunities and Risks. 2018. Available online: https://www.euro.who.int/__data/assets/pdf_file/0004/374917/Circular-Economy_EN_WHO_web_august-2018.pdf?ua=1 (accessed on 3 August 2020).
- Pachauri, A.; Shah, P.; Almroth, B.C.; Sevilla, N.P.M.; Narasimhan, M. Safe and sustainable waste management of self-care products. BMJ 2019, 365, l1298. [Google Scholar] [CrossRef] [Green Version]
- Potting, J.; Hekkert, M.; Worrell, E.; Hanemaaijer, A. Circular Economy: Measuring Innovation in the Product Chain; PBL Netherlands Environmental Assessment Agency: The Hague, The Netherlands, 2017. [Google Scholar]
- UNDP Sustainable Development Goals. 2020. Available online: https://www.undp.org/content/undp/en/home/sustainable-development-goals.html#:~:text=The%20Sustainable%20Development%20Goals%20(SDGs,peace%20 (accessed on 28 August 2020).
- Toh, M.R.; Chew, L. Turning waste medicines to cost savings: A pilot study on the feasibility of medication recycling as a solution to drug wastage. Palliat. Med. 2016, 31, 35–41. [Google Scholar] [CrossRef]
- Viegas, C.V.; Bond, A.; Vaz, C.R.; Bertolo, R.J. Reverse flows within the pharmaceutical supply chain: A classificatory review from the perspective of end-of-use and end-of-life medicines. J. Clean. Prod. 2019, 238, 117719. [Google Scholar] [CrossRef]
- FDA. Coronavirus (COVID-19) Supply Chain Update. 2020. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-supply-chain-update (accessed on 28 August 2020).
- Mylan. EpiPen Supply Information. 2020. Available online: https://www.epipen.com/about-epipen-and-generic/supply-information (accessed on 28 August 2020).
- Ogden, J. Implementing the EU Falsified Medicines Directive. Prescriber 2019, 30, 30–33. [Google Scholar] [CrossRef] [Green Version]
- NHS UK. Principles on the Disposal of Waste Pharmaceuticals Used Within Community Health Services. Version 3.1. 2013. Available online: https://www.sps.nhs.uk/wpcontent/uploads/2012/08/Disposal20of20Waste20Pharmaceuticals20used20within20CHS.pdf (accessed on 25 June 2019).
- GSK Complete the Cycle|GSK UK. 2018. Available online: https://uk.gsk.com/en-gb/responsibility/our-planet/complete-the-cycle (accessed on 19 July 2019).
- Crews, J. Prescription Drug Reuse and Recycling. Oncol. Issues 2019, 34, 2. [Google Scholar] [CrossRef]
- Settanni, E.; Harrington, T.S.; Srai, J.S. Pharmaceutical supply chain models: A synthesis from a system view of operations research. Oper. Res. Perspect. 2017, 4, 74–95. [Google Scholar] [CrossRef] [Green Version]
- NHS Novel Coronavirus (COVID-19) Standard Operating Procedure Running a Medicines Re-Use Scheme in a Care Home or Hospice Setting. 2020. Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-reuse-of-medicines-in-a-care-home-or-hospice/novel-coronavirus-covid-19-standard-operating-procedure-running-a-medicines-re-use-scheme-in-a-care-home-or-hospice-setting (accessed on 1 June 2020).
- Taylor, D. The Impact of Politics on UK Pharmacy and the Economics of Medicines Supply. 2007. Pharm. J. 2007, 279, 308. [Google Scholar]
- WHO. WHO Guideline on Country Pharmaceutical Pricing Policies. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/153920/;jsessionid=DD2BEA983D83DD818AA64A81F3BA3B28?sequence=1 (accessed on 5 July 2020).
- European Commission. Leading the Way to a Global Circular Economy: State of Play and Outlook. 2020. Available online: https://ec.europa.eu/environment/circular-economy/pdf/leading_way_global_circular_economy.pdf (accessed on 5 July 2020).
- De Groene Zaak. Governments Going Circular. 2015. Available online: http://www.govsgocircular.com/media/1354/governments-going-circular-dgz-feb2015.pdf (accessed on 9 July 2020).
- Briguglio, M.; Spiteri, J. Enablers and Barriers to a Circular Economy. 2018. Available online: http://www.r2piproject.eu/wp-content/uploads/2018/08/R2pi-stakeholders-report-sept-2018.pdf (accessed on 6 July 2020).
- Goodwin, E. Opinion: Circular Economy in Pharmaceutical Production Plants. 2020. Available online: https://www.cleanroomtechnology.com/news/article_page/Opinion_Circular_economy_in_pharmaceutical_production_plants/162646 (accessed on 5 July 2020).




{kind=link}
{kind=link}
{kind=link}
| Waste Creation Point | Issue | Current Resolution/Practice |
|---|---|---|
| Manufacturing | Overproduction of stock based on forecasted demand. | Secure accurate demand based on transparency and sharing of information across the supply chain facilitated by government bodies [24,25] |
| Overproduction of stock based on actual demand, e.g., a medicines shortage (but short lived so excess stock is created). | Ensure the transparency of stock production and use and effective reporting of medicines shortages between pharmacies, wholesalers, and manufacturers [24] Distinguish the cause of the shortage and focus efforts there to increase or use on-hand supply [24,25] | |
| Pharmacy | Overordering of stock by pharmacy. | Implement effective procurement training and inventory management systems [26] |
| Insufficient storage conditions by pharmacy. | Conduct regular checks ensure suitable conditions of light, humidity, ventilation, temperature, and security [26] | |
| Hospital Wards/Clinics/Estates | Excess stock requested and held by wards or clinics. | Create stock lists at the ward level with the support of pharmacy store teams to manage stock levels of wards effectively [27] |
| Incorrect medication prescribed for patient and not enough or unclear information given. | Enact effective processes to process and dispense prescriptions supported by accurate information from a consultant to avoid irrational medication. Also, ensure that clarification is offered to the patients regarding the dosage, use, and advantages and disadvantages of the recommended pharmaceutical [28,29,30] | |
| Patient is deceased but medication is in their name and cannot be used by anyone else. | Reuse prescribed medications if the patient is deceased. This applies if, for example, there is no available stock, no available alternatives, and there is no risk associated with other patients using the medicines [31,32] | |
| Medicines not rotated or used effectively (manual intervention based on expiry dates) or inventory management systems not utilized effectively to reduce stock obsolescence. | Provide effective training for staff and use of inventory management systems [26] | |
| Patient’s own medicine lost on admission and, therefore, are not available for use. | Encourage patients to bring their own medicines. Design system to ensure patients’ own medicines stay with them using green bags, e.g., the green bag scheme for improving the utilization of prescriptions for better results and decreased waste [29,30] | |
| Inadequate resources to support effective management of pharmaceuticals waste segregation and disposal. | Create dedicated resources to support pharmaceuticals waste management and safe disposal [33] Both small-scale (e.g., training programs) and large-scale (e.g., legislative and administrative) solutions are needed to ensure safe waste management [34] | |
| General Practitioner (GP)/Consultants | Overprescribing by GPs/consultants. | Undertake informed prescribing in relation to quantity and frequency, guided by current data on stock availability provided by government bodies [35,36] Develop a system to permit patients to improve their overstocking and ordering of medication [35,36] |
| Remote prescribing by GPs. | Remote prescribing are applied care home. But is being addressed with the introduction of pharmacists to manage prescriptions more effectively [37,38,39] | |
| Care Homes | Excess stock received and held for patients. | Educate staff to contact GP regarding prescribing patterns and use a pharmacist to support medicines use [31,32,33,34,35,36,37,38,39,40] |
| Patients | Repeating prescriptions requested by patients. | Educate and facilitate patients to request stock when needed and approved by GP without overstocking [34,35,36,40] |
| Advising GP or healthcare professional when they cannot take medicines and no longer needed. | Educate and facilitate medicines returns to pharmacy, GP, or another reliable repository [38] |
| Treatment | Advantages | Disadvantages |
|---|---|---|
| Incineration [67] | Low cost, accepts different waste types, minimises the waste volume | Not environmentally friendly, increases pollution, high cost |
| Autoclaving [68] | Environmentally friendly, used for infectious waste and sharps | Does not minimise the volume and is not cost effective |
| Microwave Irradiation [69] | No combustion or gasification, minimal emissions | Not applicable for all waste, high cost |
| Pyrolysis [69] | Environmentally friendly, disposes of all kinds of waste, minimises the waste volume | High cost, requires certified professional workers |
| Landfill [68] | Low cost | Not environmentally friendly, increases health risks |
| Recycling [70] | Environmentally friendly, reduces cost | Not all types of waste can be recycled |
| Issues | Obstacles |
|---|---|
| Safety [2,31,76,85] | Returned medicines may have been subject to intentional tampering, e.g., incorrect packaging. Some presently utilised seals on external medication packaging lack careful designs and effectiveness. Packaging may be unsealed. Packaging may have been contaminated while in a patient’s possession. |
| Quality [2,31,76,85] | Medicines may have been stored in undesirable conditions, e.g., temperature, moisture, light. Medicines may have an undesirable smell. Counterfeit medicines via a redistribution scheme. The dispensing and expiration dates may affect the quality of the medication. |
| R-Strategies | Aim | ||
|---|---|---|---|
 | Better Use of Products and Manufacture | (0) Refuse | Make product redundant by abandoning its function or by offering the same function with a radically different product. |
| (1) Rethink | Make product use more intensive (e.g., by sharing product). | ||
| (2) Reduce | Increase efficiency in product manufacture or use by consuming fewer natural resources and materials. | ||
| Expanding the Lifecycle of Product and Elements | (3) Reuse | Reuse by another consumer of discarded product which is still in good condition and fulfils its original function. | |
| (4) Repair | Repair and maintenance of defective product so it can be used with its original function. | ||
| (5) Refurbish | Restore an old product and bring it up to date. | ||
| (6) Remanufacture | Use parts of discarded product in a new product with the same function. | ||
| Useful Application of Material | (7) Repurpose | Use discarded product or its parts in a new product with a different function. | |
| (8) Recycle | Process materials to obtain the same (high grade) or lower (low grade) quality. | ||
| (9) Recover | Incineration of material with energy recovery. |
| Product/Practice | Action |
|---|---|
| Drug Donations [9,94,95,97,98] | Consideration of how medicine donations from medicinal services and patients could help reduce waste and increase the reuse and recycling of medicines. These medicines could be used for individuals who cannot afford their medication. |
| Epinephrine Injection (EpiPen) [99,100] | Extension of the product’s lifecycle, as prompted by medicine shortages. |
| Falsified Medicines Directive (FMD) and Support of Anti Counterfeit Technologies [101] | The introduction of FMD and the adoption of technologies to reduce counterfeit drug presence in the supply chain. This increases the transparency of stock, increases confidence in stock integrity and reduces risk of patient harm. |
| Inhalers [102,103] | Promotion of more environmentally friendly inhalers and recycling of outer packaging/cartridges for reuse. |
| Medication Dosing—Cancer Treatments [31] | Based on group volume, offering clinics to share vials of medications, ensuring maximum utilisation of stock and reducing waste and cost. This also positively impacts stock creation and holding within the supply chain due to the reduced risk of obsolescence. |
| Prescribing (quantity/frequency) [26,41,48,52] | Consideration of a practice of prescribing medicines in specific quantities and frequencies, which can smooth out the demand for specific medications, reducing the risk of shortage and domestic stockpiling. This practice could also promote the equity of access to medication. |
| Return Schemesfor Medication Reuse [46,104] | Verifying the safety and quality of returned medications and ensuring that medicines have tamper evident packaging to help endorse the reuse of medication scheme. |
| Return Schemesfor Safe Disposal [79] | For example, DUMP schemes, where patients are encouraged to remove unwanted products from their homes to reduce risks to patient and family safety and reduce potential environmental harm. |
| API Recovery for Reuse | Green engineering technology to recover and reuse the API (extracting, purifying, and repacking) can help to minimize waste and provide it value again [48,83]. |
| Criteria PESTLE | Enablers | Barriers | Importance |
|---|---|---|---|
| (P) [107,108,109] | Tax incentives in the PSC positively support the CE. International agreements and collaborations lead to the enforcement of effective policies in the PSC. Government funding exists for CE projects. | There is inadequate government funding to shift the PSC to the CE. There is no effective enforcement strategy to shift the pharmaceutical sector to the CE. The discriminatory implementation and establishment of PSC policies discourage the shift to the CE. | Political factors help to set the directions and encourage innovation through funding. |
| (E) [80,81,82] | Reduction in the use of pharmaceuticals leads to minimised costs. An increase in household healthcare expenditures creates a need to reduce the cost of production. | There are pricing pressure in the PSC between different suppliers. The high cost of establishing the CE is challenged by the low revenues of the pharmaceutical industry. The current medicine taxation system is a barrier to the transition to the CE. | The economy is a significant determinant of the running of the PSC because it guides supply and demand. |
| (S) [46,109,110] | New preferences in the population regarding the form of medications that are administered enable the shift towards the CE. Suppliers in the sector have a shared CE vision, which facilitates achieving it. | There is resistance from internal PSC and society to change from linear production to the CE in the PSC. Insufficient information on the recycling and reuse of medicine and related benefits results in hesitation to change. There is an absence of technical skills in applying the CE in the PSC while saving on costs. | Social factors determine the demand for medications by consumers of pharmaceutical products and their medication disposal behaviours. |
| (T) [2,92,110] | Secure information sharing systems are needed within medication tracking systems. Technology makes it easier to engage with patients. Technology helps minimise the stockpile of medications on the shelf and efficiently manage the stock. Advanced medicine manufacturing technology supports the transition to CE. | The cost of developing and applying a new advanced technology to transition to the CE is high. There is inadequate expertise in running the technical equipment needed for the CE in the PSC. | The PSC relies on technology for production and efficiency in its operations. |
| (L) [82,111,112] | Proposals concerning the reduction of waste produced by pharmaceutical manufacturers support the CE. Regulations on standards of pharmaceutical distribution process support the CE. | There is a lack of systems to measure and assess the CE in the PSC. There is a lack of effective legislation on poor waste management. The existing laws are not clear about pharmaceutical producers’ responsibility for waste management. | The PSC requires legal regulations to guide supply chain operations. |
| (E) [62,63,64] | Pharmaceutical and biotech companies’ high levels of energy consumption drive them to seek more eco-friendly means of operation. Emphasis that is placed on the benefits of recycling, reusing and reducing medicines supports the production of medicines in a CE. Needs to change the poor management of pharmaceutical disposal methods. | There is a lack of adequately set strategies on the recycling and reuse of medicine in an environmentally friendly way. Existing laws are not clear about the responsibility of the producers regarding waste management. Individuals’ awareness of proper medicine disposal is low. | The PSC is a sector that must meet high standards of quality, which are achieved by improving existing environmental conditions. |
| Level of Analysis | Focus Area | Consideration for Change |
|---|---|---|
| Meta Level (Global) E.g., WHO, UN, International Federation of Pharmacists | Recognition and endorsement Policy generation | Global recognition of pharmaceutical waste levels. Inclusion of waste reduction targets in global sustainability policy |
| Macro Level (National) E.g., government, suppliers/wholesalers, healthcare bodies, pharma advisory bodies | Recognition and endorsement Resource allocation CE philosophy acknowledgment Financial support Adoption of innovative technologies Awareness and education | Endorsement of CE agenda in the pharmaceutical supply chain. Agreement to provide resources to target pharmaceuticals waste reduction Acknowledgment of the value of CE philosophy in the design of waste reduction policies and practices Financial support for innovative technologies to deliver green design/logistics Building awareness of the 3Rs of CE (reduce, reuse, recycle) into pharmacist education Design and delivery of awareness campaigns to healthcare professionals and patients (co-designed output) |
| Meso Level (Organisational) E.g., hospitals, community pharmacies, GP, healthcare professionals | System design and delivery Patient education delivery and support Facilitation of medicine returns/design of collection channels Resource allocation Champion identification Strategic organisational approach to waste reduction | Creation of efficient medicine management systems to minimize waste creation and ensure safe disposal Engage in patient education to raise awareness of medicine use and waste creation channels Design effective channels for medicine returns/collections Dedicate time for medicine management training regarding ordering, storage, reuse/recycling Build teams to facilitate medicine stock management/retrieval from wards, conduct returns audits and safe disposal Identify champions to support pharmaceuticals waste reduction practices |
| Micro Level (Individual) E.g., pharmacy staff, manufacturers, suppliers wholesaler, distributors, patients | Awareness of pharmaceuticals waste creation Awareness of medicine returns Facilitation of returns Civic responsibility Engagement in educational campaigns | Engage in an educational campaign on the scale of pharmaceuticals waste and the financial, social and environmental repercussions associated with poor medicine management Adopt a personal responsibility to reduce pharmaceuticals waste as part of civic duty Work with stakeholders to design simple mechanisms to prompt medicine returns (e.g., text messages, flyers). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshemari, A.; Breen, L.; Quinn, G.; Sivarajah, U. Can We Create a Circular Pharmaceutical Supply Chain (CPSC) to Reduce Medicines Waste? Pharmacy 2020, 8, 221. https://doi.org/10.3390/pharmacy8040221
Alshemari A, Breen L, Quinn G, Sivarajah U. Can We Create a Circular Pharmaceutical Supply Chain (CPSC) to Reduce Medicines Waste? Pharmacy. 2020; 8(4):221. https://doi.org/10.3390/pharmacy8040221
Chicago/Turabian StyleAlshemari, Abdullah, Liz Breen, Gemma Quinn, and Uthayasankar Sivarajah. 2020. "Can We Create a Circular Pharmaceutical Supply Chain (CPSC) to Reduce Medicines Waste?" Pharmacy 8, no. 4: 221. https://doi.org/10.3390/pharmacy8040221
APA StyleAlshemari, A., Breen, L., Quinn, G., & Sivarajah, U. (2020). Can We Create a Circular Pharmaceutical Supply Chain (CPSC) to Reduce Medicines Waste? Pharmacy, 8(4), 221. https://doi.org/10.3390/pharmacy8040221