
Infrared Thermal Imaging and Artificial Neural Networks to Screen for Wrist Fractures in Pediatrics



Abstract
:1. Introduction
- A new method of IRTI feature extraction to suitably represent the fracture site.
- Demonstration of a statistically significant temperature difference between wrist fracture and wrist sprain (no fracture).
- Development of a multilayer perceptron (MLP) neural network model to discriminate between wrist fracture and wrist sprain.
- Effective utilization of available patient data through random selection of participants for inclusion in the training and test files for MLP processing and averaging the results over 100 trials to obtain sensitivity and specificity.
2. IR Thermal Imaging for Bone Fracture Detection and Monitoring
3. Materials and Methods
3.1. Evaluation Statistics
- True positives, TP, (a): number of participants with wrist fracture (confirmed by x-ray) correctly identified as fracture by IRTI.
- False positives, FP, (b): number of participants with wrist sprain (not-fracture, confirmed by x-ray) misidentified as fracture by IRTI.
- False negatives, FN, (c): number of participants with wrist fracture misidentified as sprain by IRTI.
- True negatives, TN, (d): number of participants with wrist sprain correctly identified as sprain by IRTI.
- Sensitivity: the percentage of true positives (fractures) correctly identified by IRTI, i.e.,
- Positive predictive value: IRTI-identified percentage of participants with positive result (identified as fracture) who have fracture, i.e.,
- Negative predictive value: IRTI-identified percentage of participants with a negative result (identified as sprain) who do not have fracture, i.e.,
- Accuracy: IRTI-identified proportion of true results, either true positive or true negative, in a population. It measures the degree of veracity of IRTI as the fracture screening scheme.
3.2. Recruitment
- Non-native English speakers (the study did not utilize interpreters).
- Patients sustaining multiple injuries (including injury to both wrists).
- Patients triaged above category D due to severe pain or deformity.
- Patients who declined consent.
3.3. Recording
3.4. Image Processing and Feature Extraction
3.4.1. Selection of Region of Interest and Tracking
3.4.2. ROI Feature Extraction
3.5. Discrimination Using Multilayer Perceptron Neural Network
- Error backpropagation learning function to update the weights: gradient descent with momentum. This learning function is commonly used with MLP. The function incorporated two parameters: learning rate and momentum. Learning rate controls its adaptation (learning or training) speed. The momentum term helps the function to move out of local minima to a global minimum when determining error [34]. For both parameters, values between 0.01 and 1 were explored, and 0.05 was selected, as it provided the best differentiation.
- Training termination: Training stopped the duration of each trial when the error became insignificant (0.01) or when the number of iterations reached 20,000. The second criteria ensured training to be terminated when the error could not reach its specified target value.
- Transfer (activation function): the sigmoid transfer function was used for all processing elements. It provides an output between 0 and 1 and is commonly used for MLP [31].
4. Results
4.1 Feature Analysis
- 13 (68.4%) participants with fracture had maximum temperatures greater than sprain participants maximum temperature.
- 10 (52.6%) participants with fracture had minimum temperatures greater than sprain participants minimum temperature.
- 12 (63.2%) participants with fracture had mean temperatures greater than sprain participants mean temperature.
- 14 (73.7%) participants with fracture had standard deviations (from the mean) greater than sprain participants standard deviation.
- 12 (63.2%) participants with fracture had median temperatures greater than sprain participants median temperature.
- 8 (42.1%) participants with fracture had mode temperatures greater than the sprain participants mode temperature.
- 13 (68.4%) participants with fracture had skewness values lower than sprain participants skewness.
- 16 (82.2%) participants with fracture had kurtosis values lower than sprain participants kurtosis.
- 14 (73.7%) participants with fracture had IQR values greater than sprain participants IQR.
- Kurtosis;
- Standard deviation from the mean and IQR;
- Skewness and maximum temperature;
- Mean and median;
- Minimum;
- Mode.
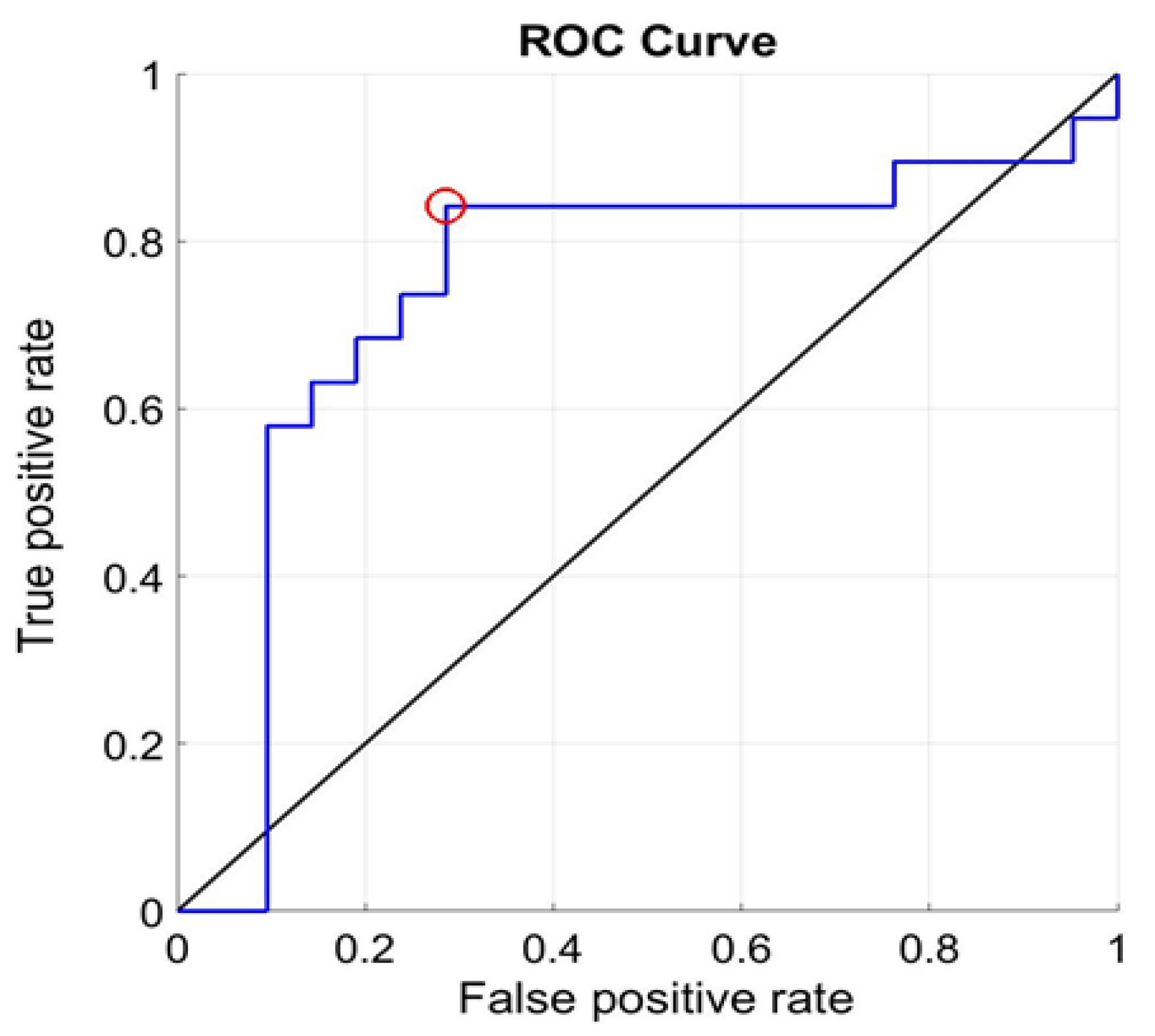
4.2 Multilayer Perceptron Discrimination Results for Investigation A
- Number of true positives = 16;
- Number of true negatives = 15;
- Number of false negatives = 3;
- Number of false positives = 6.
4.3 Multilayer Perceptron Discrimination Results for Investigation B
- Number of true positives = 16;
- Number of true negatives = 15;
- Number of false negatives = 3;
- Number of false positives = 6.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Error Backpropagation Algorithm
- The subscripts i, j and k represent the input, hidden and output layers of the MLP, respectively.
- The weights from the hidden layer to the output layer: wkj;
- The weights from the input layer to the hidden layer: wji;
- The input to a processing element: net;
- The output of a processing element (i.e., the transfer function output): y;
- The target (desired) value provided during training: t;
- Number of input examples used during training: k;
- The convergence control parameter (learning rate): ;
- Proportionality: .
References
- Eschweiler, J.; Li, J.; Quack, V.; Rath, B.; Baroncini, A.; Hildebrand, F.; Migliorini, F. Anatomy, biomechanics, and loads of the wrist joint. Life 2022, 12, 188. [Google Scholar] [CrossRef]
- Jennison, T.; Brinsden, M. Fracture admission trends in England over a ten-year period. Ann. R. Coll. Surg. Engl. 2019, 101, 208–214. [Google Scholar] [CrossRef]
- Mamoowala, N.; Johnson, N.A.; Dias, J.J. Trends in paediatric distal radius fractures: An eight-year review from a large UK trauma unit. Ann. R. Coll. Surg. Engl. 2019, 101, 297–303. [Google Scholar] [CrossRef]
- Khosla, S.; Melton, L.J.; Dekutoski, M.B.; Achenbach, S.J.; Oberg, A.L.; Riggs, B.L. Incidence of childhood distal forearm fractures over 30 years: A population-based study. JAMA 2003, 290, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Rennie, L.; Court-Brown, C.M.; Mok, J.Y.Q.; Beattie, T.F. The epidemiology of fractures in children. Injury 2007, 38, 913–922. [Google Scholar] [CrossRef]
- Welling, R.D.; Jacobson, J.A.; Jamadar, D.A.; Chong, S.; Caoili, E.M.; Jebson, P.J.L. MDCT and radiography of wrist fractures: Radiographic sensitivity and fracture patterns. AJR 2008, 190, 10–16. [Google Scholar] [CrossRef]
- Jahagirdar, R.; Scammell, B.E. Principles of fracture healing and disorders of bone union. Surgery 2008, 27, 63–69. [Google Scholar] [CrossRef]
- Little, J.T.; Klionsky, N.B.; Chaturvedi, A.; Soral, A.; Chaturvedi, A. Pediatric distal forearm and wrist injury: An imaging review. RadioGraphics 2014, 33, 472–490. [Google Scholar] [CrossRef]
- Sendher, R.; Ladd, A. The scaphoid. Orthop. Clin. N. Am. 2013, 44, 107–120. [Google Scholar] [CrossRef]
- Wraighte, P.J.; Scammell, B.E. Principles of fracture healing. Surgery 2006, 24, 198–207. [Google Scholar]
- Slaar, A.; Bentohami, A.; Kessels, J.; Bijlsma, T.S.; van Dijkman, B.A.; Maas, M.; Wilde, J.C.H.; Goslings, J.C.; Schep, N.W.L. The role of plain radiography in paediatric wrist trauma. Insights Imaging 2012, 3, 513–517. [Google Scholar] [CrossRef]
- Owen, R.; Ramlakhan, S. Infrared thermography in paediatrics: A narrative review of clinical use. BMJ Paediatr. Open 2017, 1, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Usamentiaga, R.; Venegas, P.; Guerediaga, J.; Vega, L.; Molleda, J.; Bulnes, F.G. Infrared thermography for temperature measurement and non-destructive testing. Sensors 2014, 14, 12305–12348. [Google Scholar] [CrossRef] [Green Version]
- Halužan, D.; Davila, S.; Antabak, A.; Dobric, I.; Stipic, I.; Augustin, G.; Ehrenfreund, T.; Prlić, I. Thermal changes during healing of distal radius fractures-Preliminary findings. Injury 2015, 46, S103–S106. [Google Scholar] [CrossRef]
- Ćurković, S.; Antabak, A.; Halužan, D.; Luetić, T.; Prlić, I.; Šiško, J. Medical thermography (digital infrared thermal imaging—DITI) in paediatric forearm fractures—A pilot study. Injury Int. J. Care Injured 2015, 46S, S36–S39. [Google Scholar] [CrossRef] [Green Version]
- De Salis, A.F.; Saatchi, R.; Dimitri, P. Evaluation of high resolution thermal imaging to determine the effect of vertebral fractures on associated skin surface temperature in children with osteogenesis imperfecta. Med. Biol. Eng. Comput. 2018, 56, 1633–1643. [Google Scholar] [CrossRef]
- Reed, C.; Saatchi, R.; Burke, D.; Ramlakhan, S. Infrared thermal imaging as a screening tool for paediatric wrist fractures. Med. Biol. Eng. Comput. 2020, 58, 1549–1563. [Google Scholar] [CrossRef]
- Sanchis-Sánchez, E.; Salvador-Palmer, R.; Codoñer-Franch, P.; Martín, J.; Vergara-Hernández, C.; Blasco, J.; Ballester, E.; Sanchis, E.; González-Peña, R.; Cibrián, R. Infrared thermography is useful for ruling out fractures in paediatric emergencies. Eur. J. Pediatr. 2015, 174, 493–499. [Google Scholar] [CrossRef]
- Lalkhen, A.G.; McCluskey, A. Clinical tests: Sensitivity and specificity. Contin. Educ. Anaesth. Crit. Care Pain 2008, 8, 221–223. [Google Scholar] [CrossRef] [Green Version]
- Ramlakhan, S.L.; Saatchi, R.; Sabir, L.; Ventour, D.; Shobayo, O.; Hughes, R.; Singh, Y. Building artificial intelligence and machine learning models: A primer for emergency physicians. BMJ Emerg. Med. J. 2022, 39, e1. Available online: https://emj.bmj.com/content/39/5/e1 (accessed on 21 November 2022). [CrossRef]
- Teledyne FLIR. Available online: https://www.flir.co.uk/ (accessed on 20 October 2022).
- Togawa, T. Non-contact skin emissivity: Measurement from reflectance using step change in ambient radiation temperature. Clin. Phys. Physiol. Meas. 1989, 10, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Ammer, K.; Ring, F.J. Medical Infrared Imaging: Principles and Practice; Diakides, M., Bronzino, J.D., Perterson, D.R., Eds.; CRC Press: Boca Raton, FL, USA; Taylor and Francis Group: Abingdon, UK, 2012. [Google Scholar]
- Matlab©. Available online: https://uk.mathworks.com/products/matlab.html (accessed on 20 October 2022).
- Lewis, J.P. Fast template matching. In Proceedings of the Vision Interface 95, Canadian Image Processing and Pattern Recognition Society, Quebec City, QC, Canada, 15–19 May 1995; pp. 120–123. Available online: http://scribblethink.org/Work/nvisionInterface/vi95_lewis.pdf (accessed on 24 October 2019).
- Munsayac, F.E.T.; Alonzo, L.M.B.; Lindo, D.E.G.; Baldovino, R.G.; Bugtai, N.T. Implementation of a normalized cross-correlation coefficient-based template matching algorithm in number system conversion. In Proceedings of the IEEE 9th International Conference on Humanoid, Nanotechnology, Information Technology, Communi-cation and Control, Environment and Management (HNICEM), Manila, Philippines, 1–3 December 2017. Corpus 39411265. [Google Scholar] [CrossRef]
- Popescu, M.-C.; Balas, V.E.; Perescu-Popescu, L.; Mastorakis, N. Multilayer perceptron and neural networks. WSEAS Trans. Circuits Syst. 2009, 7, 579–588. [Google Scholar]
- Bishop, C.M. Neural networks and their applications. Rev. Sci. Instrum. 1994, 65, 1083–1832. [Google Scholar] [CrossRef] [Green Version]
- Ramlakhan, S.; Saatchi, R.; Sabir, L.; Singh, Y.; Hughes, R.; Shobayo, O.; Ventour, D. Understanding and interpreting artificial intelligence, machine learning and deep learning in Emergency Medicine. BMJ Emerg. Med. J. 2022, 39. Available online: https://emj.bmj.com/content/39/5/380 (accessed on 21 November 2022). [CrossRef] [PubMed]
- Sharkawy, A.-N. Principle of neural network and its main types: Review. J. Adv. Appl. Comput. Math. 2020, 7, 8–19. [Google Scholar] [CrossRef]
- Harrington, P.B. Sigmoid transfer functions in backpropagation neural networks. Anal. Cham. 1993, 65, 2167–2168. [Google Scholar] [CrossRef]
- Suliman, A.; Zhang, Y. A review on back-propagation neural networks in the application of remote sensing image classification. J. Earth Sci. Eng. 2015, 5, 52–65. [Google Scholar]
- Streiner, D.L.; Cairney, J. What’s under the ROC? An introduction to receiver operating characteristics curves. Can. J. Psychiatry 2007, 52, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Qian, N. On the momentum term in gradient descent learning algorithms. Neural Netw. 1999, 12, 145–151. [Google Scholar] [CrossRef]
- Willemink, M.J.; Koszek, W.A.; Hardell, C.; Wu, J.; Fleischmann, D.; Harvey, H.; Folio, L.R.; Summers, R.M.; Rubin, D.L.; Lungren, M.P. Preparing medical imaging data for machine learning. Radiology 2020, 295, 4–15. [Google Scholar] [CrossRef]
- Pasini, A. Artificial neural networks for small dataset analysis. J. Thorac. Dis. 2015, 7, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Kokol, P.; Kokol, M.; Zagoranski, S. Machine learning on small size samples: A synthetic knowledge synthesis. Sci. Prog. 2022, 105, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Shaikhina, T.; Khovanova, N.A. Handling limited datasets with neural networks in medical applications: A small-data approach. Artif. Intell. Med. 2017, 75, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Zuallaert, J.; De Neve, W. Few-shot learning using a small-sized dataset of high-resolution FUNDUS images for glaucoma diagnosis. In Proceedings of the MMHealth’17: Proceedings of the 2nd International Workshop on Multimedia for Personal Health and Health Care, Mountain View, CA, USA, 23 October 2017; pp. 89–92. [Google Scholar] [CrossRef] [Green Version]
- Dritsas, E.; Trigka, M. Machine learning techniques for chronic kidney disease risk prediction. Big Data Cogn. Comput. 2022, 6, 98. [Google Scholar] [CrossRef]
- Maharana, K.; Mondal, S.; Nemade, B. A review: Data pre-processing and data augmentation techniques. Glob. Transit. Proc. 2022, 3, 91–99. [Google Scholar] [CrossRef]
- Shorten, C.; Khoshgoftaar, T.M. A survey on image data augmentation for deep learning. J. Big Data 2019, 6, 1–48. [Google Scholar] [CrossRef]
- Zhang, C.; Bao, N.; Sun, H.; Li, H.; Li, J.; Qian, W.; Zhou, S. A deep learning image data augmentation method for single tumor segmentation. Front. Oncol. 2022. [Google Scholar] [CrossRef]
- Li, J.; Wang, D.; Li, S.; Zhang, M.; Song, C.; Chen, X. Deep learning based adaptive sequential data augmentation technique for the optical network traffic synthesis. Opt. Express 2019, 27, 18831–18847. [Google Scholar] [CrossRef]
- Chlap, P.; Min, H.; Vandenberg, N.; Dowling, J.; Holloway, L.; Haworth, A. A review of medical image data augmentation techniques for deep learning applications. J. Med. Imaging Radiat. Oncol. 2021, 65, 545–563. [Google Scholar] [CrossRef] [PubMed]
- Wythoff, B.J. Backpropagation neural networks: A tutorial. Chemom. Intell. Lab. Syst. 1993, 18, 115–155. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maximum (°C) | Minimum (°C) | Mean (°C) | Std Dev. (°C) | Median (°C) | Mode (°C) | Skewness | Kurtosis | IQR (°C) | |
|---|---|---|---|---|---|---|---|---|---|
| Fracture | 1.396 | 0.696 | 0.962 | 0.187 | 0.938 | 0.696 | 0.408 | 2.478 | 0.272 |
| Sprain | 1.048 | 0.530 | 0.711 | 0.136 | 0.690 | 0.530 | 0.595 | 2.804 | 0.202 |
| %Difference | 24.942 | 23.873 | 26.076 | 27.322 | 26.439 | 23.873 | −45.931 | 13.157 | 25.752 |
| Number of participants differentiated | 13 (f > s) | 10 (f > s) | 12 (f > s) | 14 (f > s) | 12 (f > s) | 8 (f > s) | 13 (f < s) | 16 (f < s) | 14 (f > s) |
| Injury Types | Average | Standard Deviation |
|---|---|---|
| Fracture | 0.589 | 0.264 |
| Sprain | 0.349 | 0.247 |
| Injury Types | Average | Standard Deviation |
|---|---|---|
| Fracture | 0.617 | 0.280 |
| Sprain | 0.345 | 0.252 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shobayo, O.; Saatchi, R.; Ramlakhan, S. Infrared Thermal Imaging and Artificial Neural Networks to Screen for Wrist Fractures in Pediatrics. Technologies 2022, 10, 119. https://doi.org/10.3390/technologies10060119
Shobayo O, Saatchi R, Ramlakhan S. Infrared Thermal Imaging and Artificial Neural Networks to Screen for Wrist Fractures in Pediatrics. Technologies. 2022; 10(6):119. https://doi.org/10.3390/technologies10060119
Chicago/Turabian StyleShobayo, Olamilekan, Reza Saatchi, and Shammi Ramlakhan. 2022. "Infrared Thermal Imaging and Artificial Neural Networks to Screen for Wrist Fractures in Pediatrics" Technologies 10, no. 6: 119. https://doi.org/10.3390/technologies10060119
APA StyleShobayo, O., Saatchi, R., & Ramlakhan, S. (2022). Infrared Thermal Imaging and Artificial Neural Networks to Screen for Wrist Fractures in Pediatrics. Technologies, 10(6), 119. https://doi.org/10.3390/technologies10060119