

Multi-Classification of Lung Infections Using Improved Stacking Convolution Neural Network



Abstract
:1. Introduction
- We propose an improved integrated image enhancement approach to enhance the image contrast.
- We propose an improved kernel in the stacking CNN to detect lung infection using CT scans and chest X-rays.
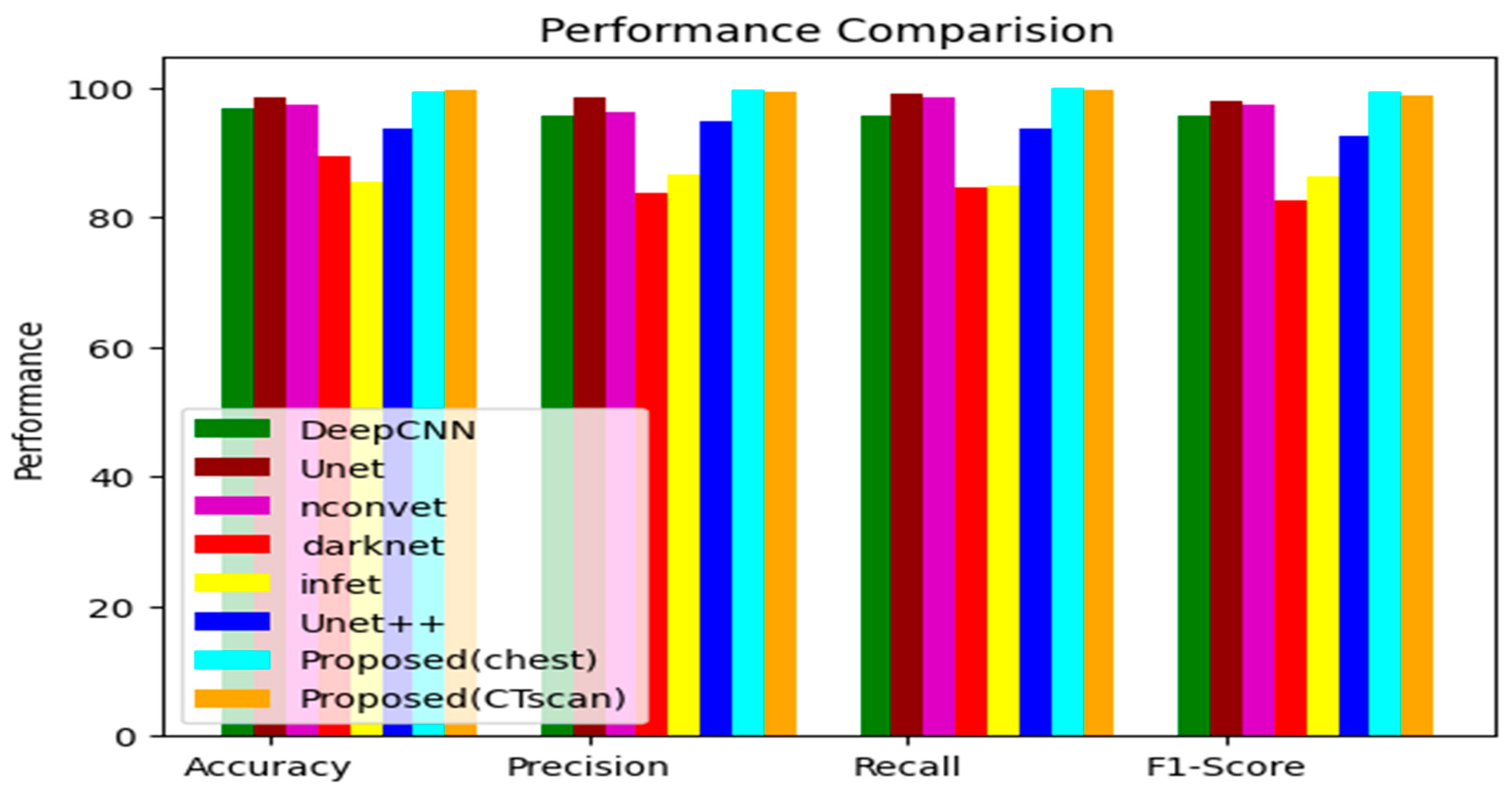
- The proposed model is compared to the existing models utilizing the CT scan and chest X-ray images.
- A comparison of the proposed model with other models shows that the proposed models have the highest performance.
2. Methods
2.1. Dataset
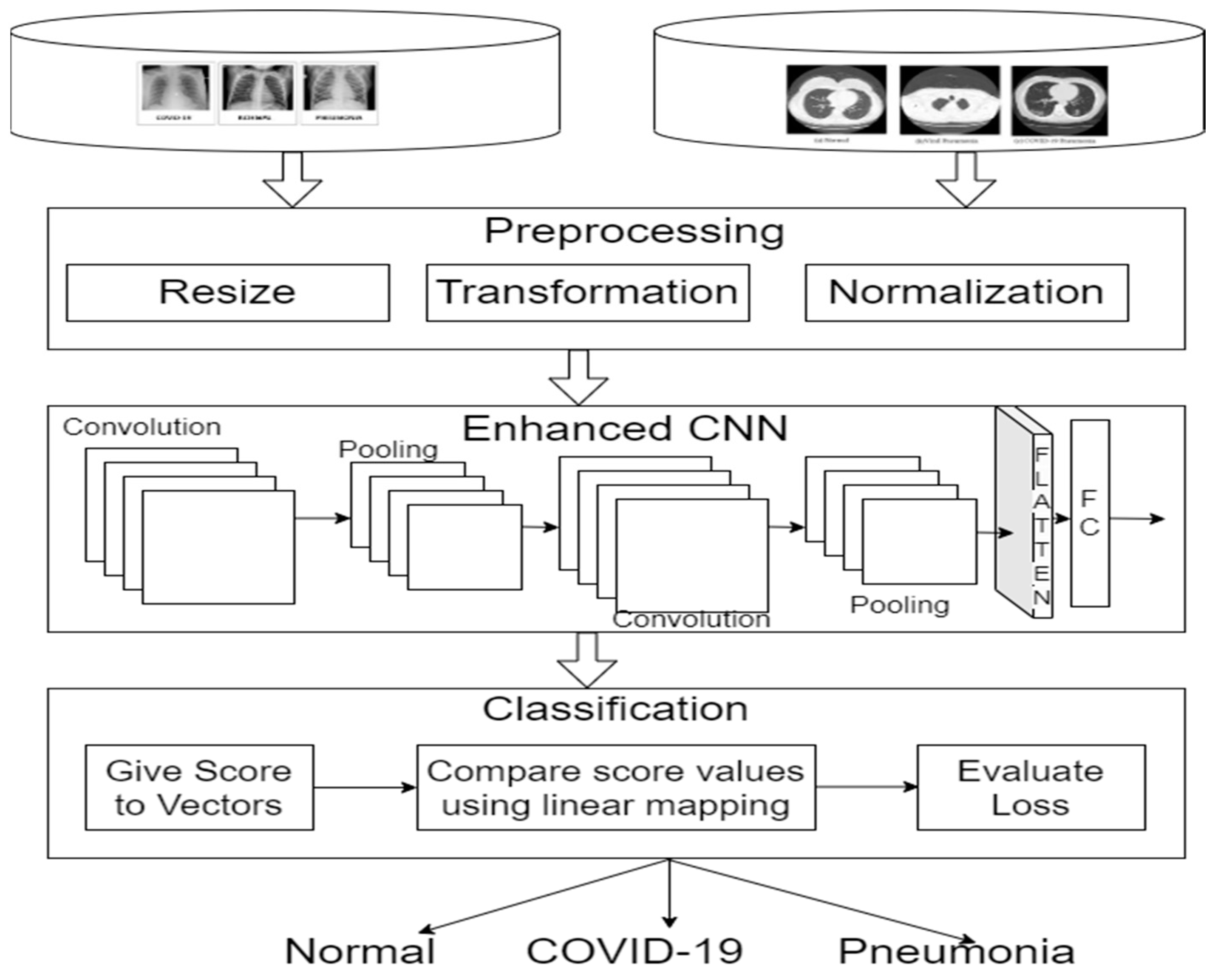
2.2. Data Pre-Processing
2.2.1. Enhanced CNN
Enhanced Kernel Convolution
| Algorithm 1: Enhanced Kernel Function |
| 1. X = {} 2. for all F, A, C {Fj, Aj, Cj} 3. obtain the kernel convolution weights 4. w(b) < −w[F⊙(b + A) + C] 5. evaluate the convolution with the enhanced kernel weights 6. X(b) < − 7. Discertize the dimensions of latent 8. For all b {b1, b2,…bn} do 9. X < −XU{}X(b)} 10. end for 11. end for 12. return list (X) |
2.2.2. Classification
| Algorithm 2: Improved SVM |
|
3. Experimental Results
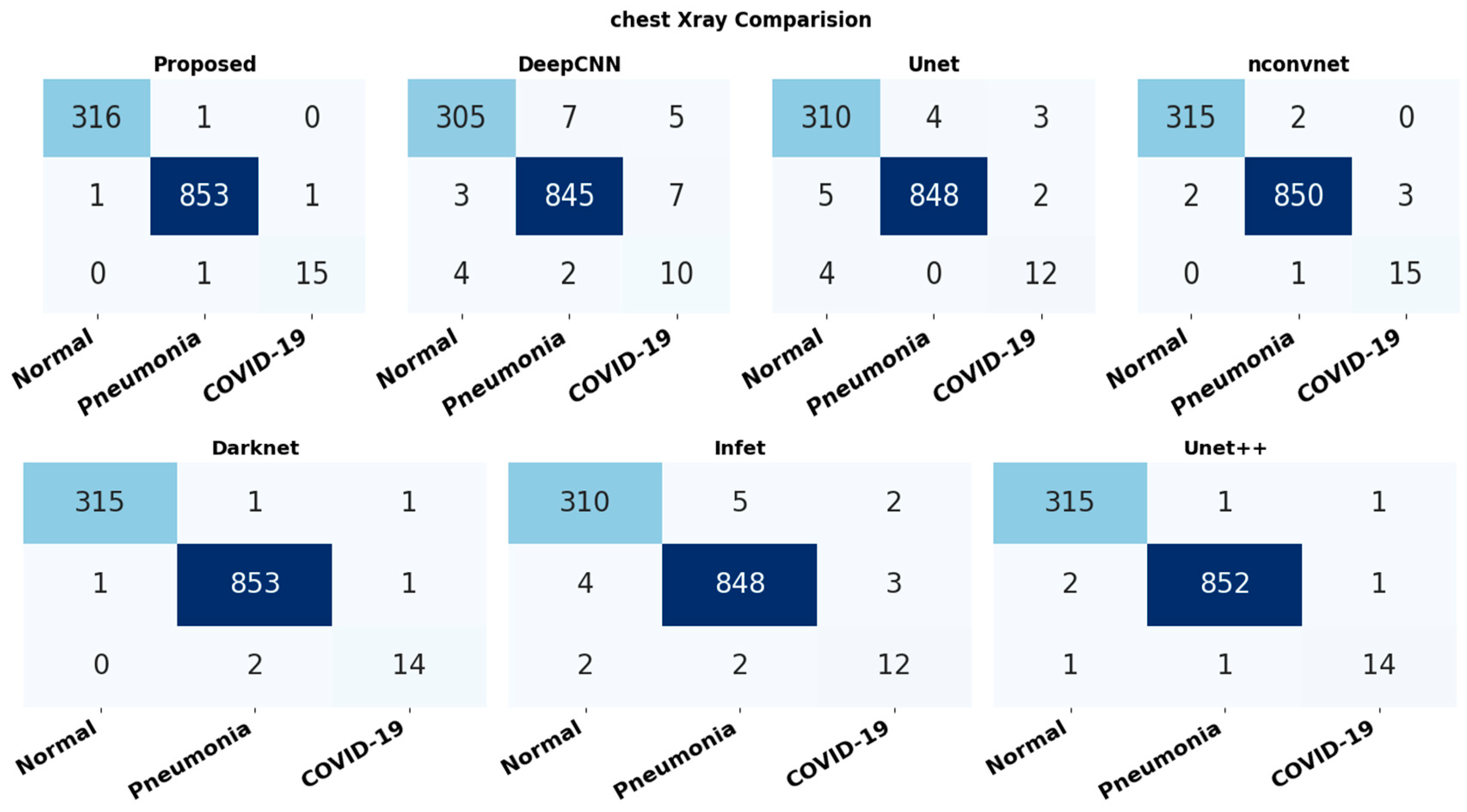
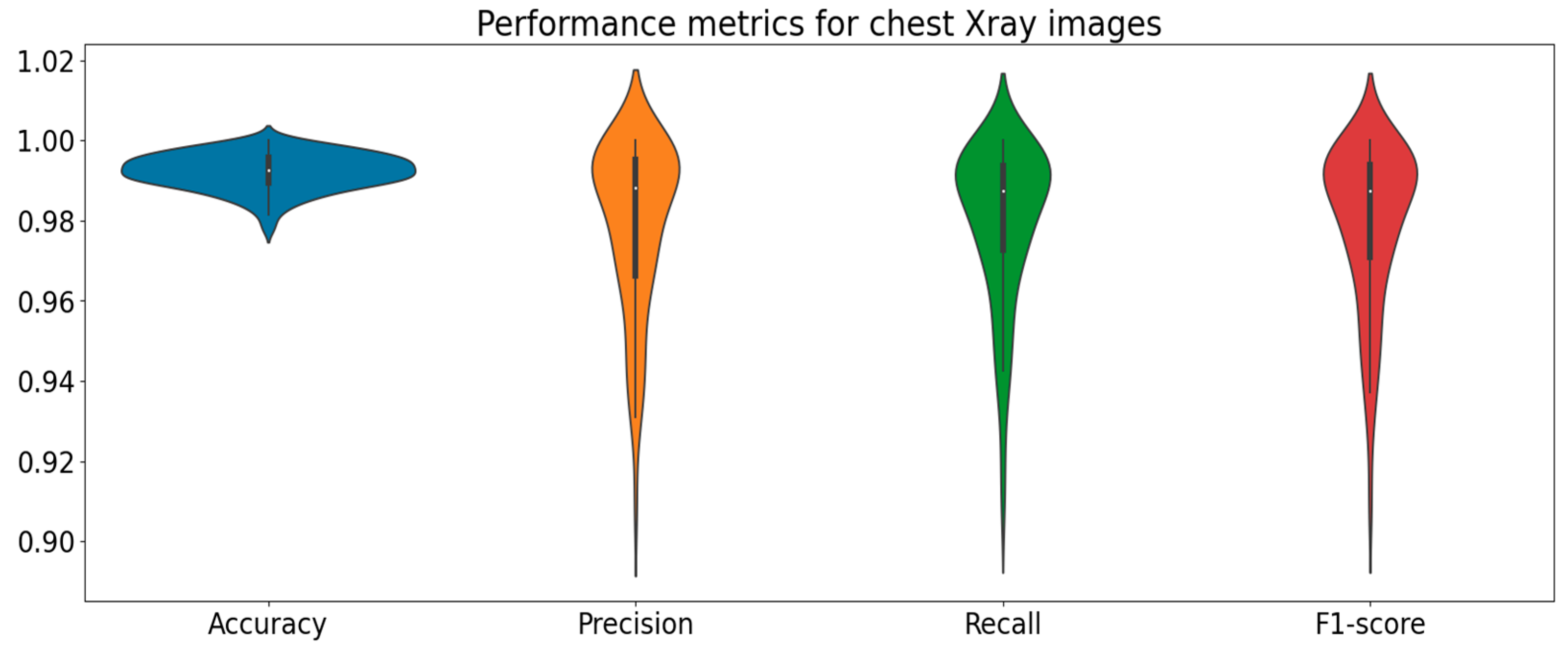
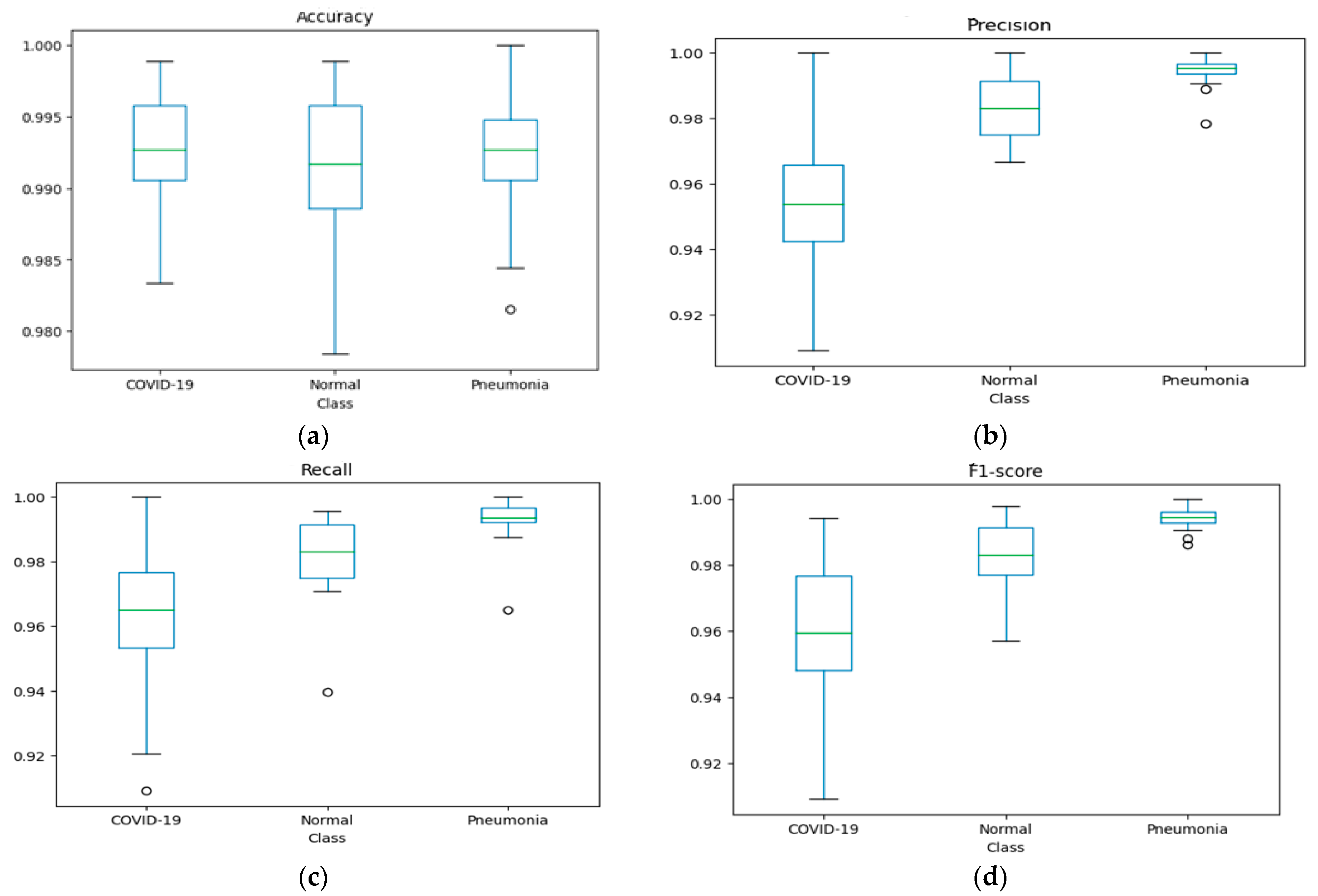
3.1. Evaluation of Chest X-ray Dataset
3.2. Evaluation of CT Scan Dataset
3.3. Performance Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanchez, C.A.; Rivera-Lozada, O.; Lozada-Urbano, M.; Best-Bandenay, P. Herd immunity in older adults from a mid-dle-income country: A time-series trend analysis of community-acquired pneumonia mortality 2003–2017. Health Sci. Rep. 2023, 6, e1224. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Tian, Z.; Lu, D.; Huang, J.; Zhang, Z.; Li, X.; Li, J. Impact of pneumonia and lung cancer on mortality of women with hypertension. Sci. Rep. 2016, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Moses, D.A. Deep learning applied to automatic disease detection using chest X-rays. J. Med. Imaging Radiat. Oncol. 2021, 65, 498–517. [Google Scholar] [CrossRef]
- Ahuja, S.; Panigrahi, B.K.; Dey, N.; Rajinikanth, V.; Gandhi, T.K. Deep transfer learning-based automated detection of COVID-19 from lung CT scan slices. Appl. Intell. 2021, 51, 571–585. [Google Scholar] [CrossRef]
- Bharati, S.; Podder, P.; Mondal, M.R.H.; Podder, P.; Kose, U. A review on epidemiology, genomic characteristics, spread, and treatments of COVID-19. Data Sci. COVID-19 2022, 2, 487–505. [Google Scholar]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.-B.; Wang, D.-C.; Mei, J.; et al. Performance of radiologists in differentiating COVID-19 from non-COVID-19 viral pneumonia at chest CT. Radiology 2020, 296, E46–E54. [Google Scholar] [CrossRef]
- Rajaraman, S.; Candemir, S.; Thoma, G.; Antani, S. Visualizing and explaining deep learning predictions for pneumonia de-tection in pediatric chest radiographs. In Proceedings of the Medical Imaging 2019: Computer-Aided Diagnosis, San Diego, CA, USA, 17–20 February 2019; Volume 10950, pp. 200–211. [Google Scholar] [CrossRef]
- Fan, D.-P.; Zhou, T.; Ji, G.-P.; Zhou, Y.; Chen, G.; Fu, H.; Shen, J.; Shao, L. Inf-net: Automatic COVID-19 lung infection seg-mentation from ct images. IEEE Trans. Med. Imaging 2020, 39, 2626–2637. [Google Scholar] [CrossRef]
- Müller, D.; Soto-Rey, I.; Kramer, F. Robust chest CT image segmentation of COVID-19 lung infection based on limited data. Inform. Med. Unlocked 2021, 25, 100681. [Google Scholar] [CrossRef]
- Ranjbarzadeh, R.; Jafarzadeh Ghoushchi, S.; Bendechache, M.; Amirabadi, A.; Ab Rahman, M.N.; Baseri Saadi, S.; Aghamo-hammadi, A.; Kooshki Forooshani, M. Lung infection segmentation for COVID-19 pneumonia based on a cascade convolu-tional network from CT images. BioMed Res. Int. 2021, 2021, 5544742. [Google Scholar] [CrossRef]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: Evaluation of the diagnostic accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef]
- Gu, X.; Pan, L.; Liang, H.; Yang, R. Classification of bacterial and viral childhood pneumonia using deep learning in chest radiography. In Proceedings of the 3rd International Conference on Multimedia and Image Processing, Guiyang, China, 16–18 March 2018; pp. 88–93. [Google Scholar] [CrossRef]
- Mazurowski, M.A.; Buda, M.; Saha, A.; Bashir, M.R. Deep learning in radiology: An overview of the concepts and a survey of the state of the art with focus on MRI. J. Magn. Reson. Imaging 2019, 49, 939–954. [Google Scholar] [CrossRef]
- Milletari, F.; Ahmadi, S.A.; Kroll, C.; Plate, A.; Rozanski, V.; Maiostre, J.; Levin, J.; Dietrich, O.; Ertl-Wagner, B.; Bötzel, K.; et al. Hough-CNN: Deep learning for segmentation of deep brain regions in MRI and ultrasound. Comput. Vis. Image Underst. 2017, 164, 92–102. [Google Scholar] [CrossRef]
- Lee, S.; Lee, Y.H. Improving emergency department efficiency by patient scheduling using deep reinforcement learning. Healthcare 2020, 8, 77. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xie, Y.; Li, Y.; Shen, C.; Xia, Y. COVID-19 screening on chest X-ray images using deep learning based anomaly detection. arXiv 2020, arXiv:2003.12338. [Google Scholar]
- Apostolopoulos, I.D.; Mpesiana, T.A. COVID-19: Automatic detection from x-ray images utilizing transfer learning with convolutional neural networks. Phys. Eng. Sci. Med. 2020, 43, 635–640. [Google Scholar] [CrossRef]
- Xia, X.; Xu, C.; Nan, B. Inception-v3 for flower classification. In Proceedings of the 2017 2nd International Conference on Image, Vision and Computing (ICIVC), Chengdu, China, 2–4 June 2017; IEEE: New York, NY, USA, 2017; pp. 783–787. [Google Scholar]
- Wang, C.; Chen, D.; Hao, L.; Liu, X.; Zeng, Y.; Chen, J.; Zhang, G. Pulmonary image classification based on inception-v3 transfer learning model. IEEE Access 2019, 7, 146533–146541. [Google Scholar] [CrossRef]
- Tsiknakis, N.; Trivizakis, E.; Vassalou, E.E.; Papadakis, G.Z.; Spandidos, D.A.; Tsatsakis, A.; Sánchez García, J.; López González, R.; Papanikolaou, N.; Karantanas, A.H.; et al. Interpretable artificial intelligence framework for COVID 19 screening on chest X rays. Exp. Ther. Med. 2020, 20, 727–735. [Google Scholar] [CrossRef]
- Sethy, P.K.; Behera, S.K.; Rath a, P.K.; Biswas, P. Detection of coronavirus disease (COVID-19) based on deep features and support vector machine. Int. J. Math. Eng. Manag. Sci. 2020, 5, 643–651. [Google Scholar] [CrossRef]
- Saha, P.; Sadi, M.S.; Islam, M.M. EMCNet: Automated COVID-19 diagnosis from X-ray images using convolutional neural network and ensemble of machine learning classifiers. Inform. Med. Unlocked 2021, 22, 100505. [Google Scholar] [CrossRef]
- Horry, M.J.; Chakraborty, S.; Paul, M.; Ulhaq, A.; Pradhan, B.; Saha, M.; Shukla, N. X-ray image based COVID-19 detection using pre-trained deep learning models. eng rXiv 2020. [Google Scholar] [CrossRef]
- SARS- CoV-2 Ct-Scan Dataset. Available online: https://www.kaggle.com/datasets/plameneduardo/sarscov2-ctscan-dataset (accessed on 20 May 2023).
- COVID-CT. Available online: https://github.com/UCSD-AI4H/COVID-CT (accessed on 20 May 2023).
- Rahimzadeh, M.; Attar, A.; Sakhaei, S.M. A fully automated deep learning-based network for detecting COVID-19 from a new and large lung CT scan dataset. Biomed. Signal Process. Control 2021, 68, 102588. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.; Abdelsamea, M.M.; Gaber, M.M. Classification of COVID-19 in chest X-ray images using DeTraC deep convolu-tional neural network. Appl. Intell. 2021, 51, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Panwar, H.; Gupta, P.K.; Siddiqui, M.K.; Morales-Menendez, R.; Singh, V. Application of deep learning for fast detection of COVID-19 in X-rays using nCOVnet. Chaos Solitons Fractals 2020, 138, 109944. [Google Scholar] [CrossRef]
- Bhuiyan, M.R.; Khushbu, S.A.; Islam, M.S. A deep learning based assistive system to classify COVID-19 face mask for human safety with YOLOv3. In Proceedings of the 2020 11th International Conference on Computing, Communication and Networking Technologies (ICCCNT), Kānpur, India, 1–3 July 2020; pp. 1–5. [Google Scholar] [CrossRef]
- Shan, F.; Gao, Y.; Wang, J.; Shi, W.; Shi, N.; Han, M.; Xue, Z.; Shen, D.; Shi, Y. Lung infection quantification of COVID-19 in CT images with deep learning. arXiv 2020, arXiv:2003.04655. [Google Scholar]
- Ross, A.; Willson, V.L. Paired samples T-test. In Basic and Advanced Statistical Tests; Brill: Leiden, The Netherlands, 2017; pp. 17–19. [Google Scholar]
- Hammoudi, K.; Benhabiles, H.; Melkemi, M.; Dornaika, F.; Arganda-Carreras, I.; Collard, D.; Scherpereel, A. Deep learning on chest X-ray images to detect and evaluate pneumonia cases at the era of COVID-19. J. Med. Syst. 2021, 45, 75. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.U.; Ozsoz, M.; Serte, S.; Al-Turjman, F.; Yakoi, P.S. Pneumonia classification using deep learning from chest X-ray images during COVID-19. Cogn. Comput. 2021, 1, 1–13. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Chest X-ray | CT Scan | ||
|---|---|---|---|---|
| Training | Testing | Training | Testing | |
| Normal | 1266 | 317 | 266 | 67 |
| Pneumonia | 3418 | 855 | 287 | 72 |
| COVID-19 | 63 | 16 | 281 | 70 |
| Total | 4747 | 1188 | 834 | 209 |
| Model | p-Value |
|---|---|
| DeepCNN | 0.01201 |
| Unet | 0.01818 |
| NCONVnet | 0.01217 |
| Darknet | 0.00402 |
| Infet | 0.00395 |
| Unet++ | 0.00245 |
| Proposed (chest X-ray) | 0.00135 |
| Proposed (CT scan) | 0.00129 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhimavarapu, U.; Chintalapudi, N.; Battineni, G. Multi-Classification of Lung Infections Using Improved Stacking Convolution Neural Network. Technologies 2023, 11, 128. https://doi.org/10.3390/technologies11050128
Bhimavarapu U, Chintalapudi N, Battineni G. Multi-Classification of Lung Infections Using Improved Stacking Convolution Neural Network. Technologies. 2023; 11(5):128. https://doi.org/10.3390/technologies11050128
Chicago/Turabian StyleBhimavarapu, Usharani, Nalini Chintalapudi, and Gopi Battineni. 2023. "Multi-Classification of Lung Infections Using Improved Stacking Convolution Neural Network" Technologies 11, no. 5: 128. https://doi.org/10.3390/technologies11050128
APA StyleBhimavarapu, U., Chintalapudi, N., & Battineni, G. (2023). Multi-Classification of Lung Infections Using Improved Stacking Convolution Neural Network. Technologies, 11(5), 128. https://doi.org/10.3390/technologies11050128