
Assessing the Impact of AI Education on Hispanic Healthcare Professionals’ Perceptions and Knowledge

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Course Description and Participant Selection
2.2. Surveys
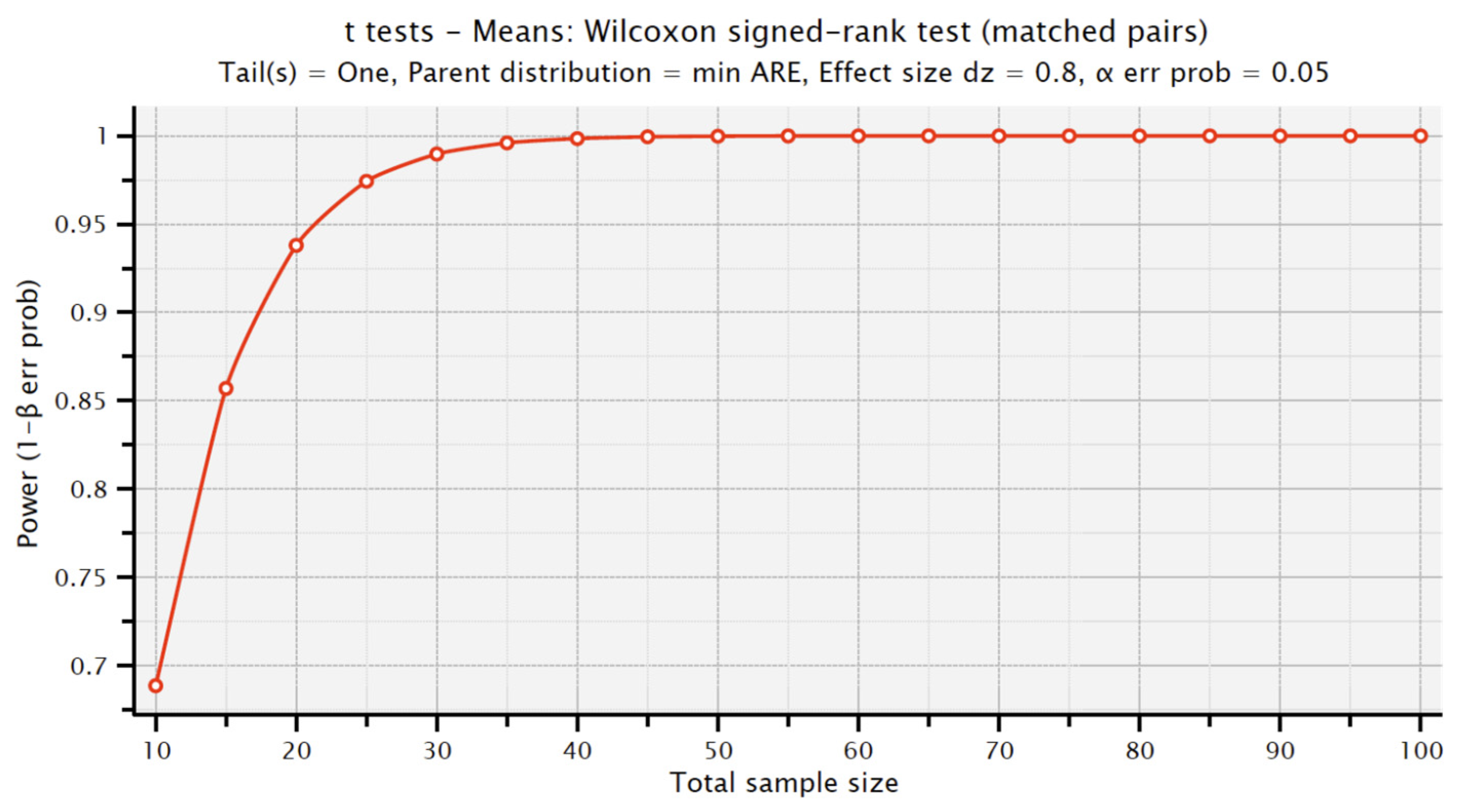
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
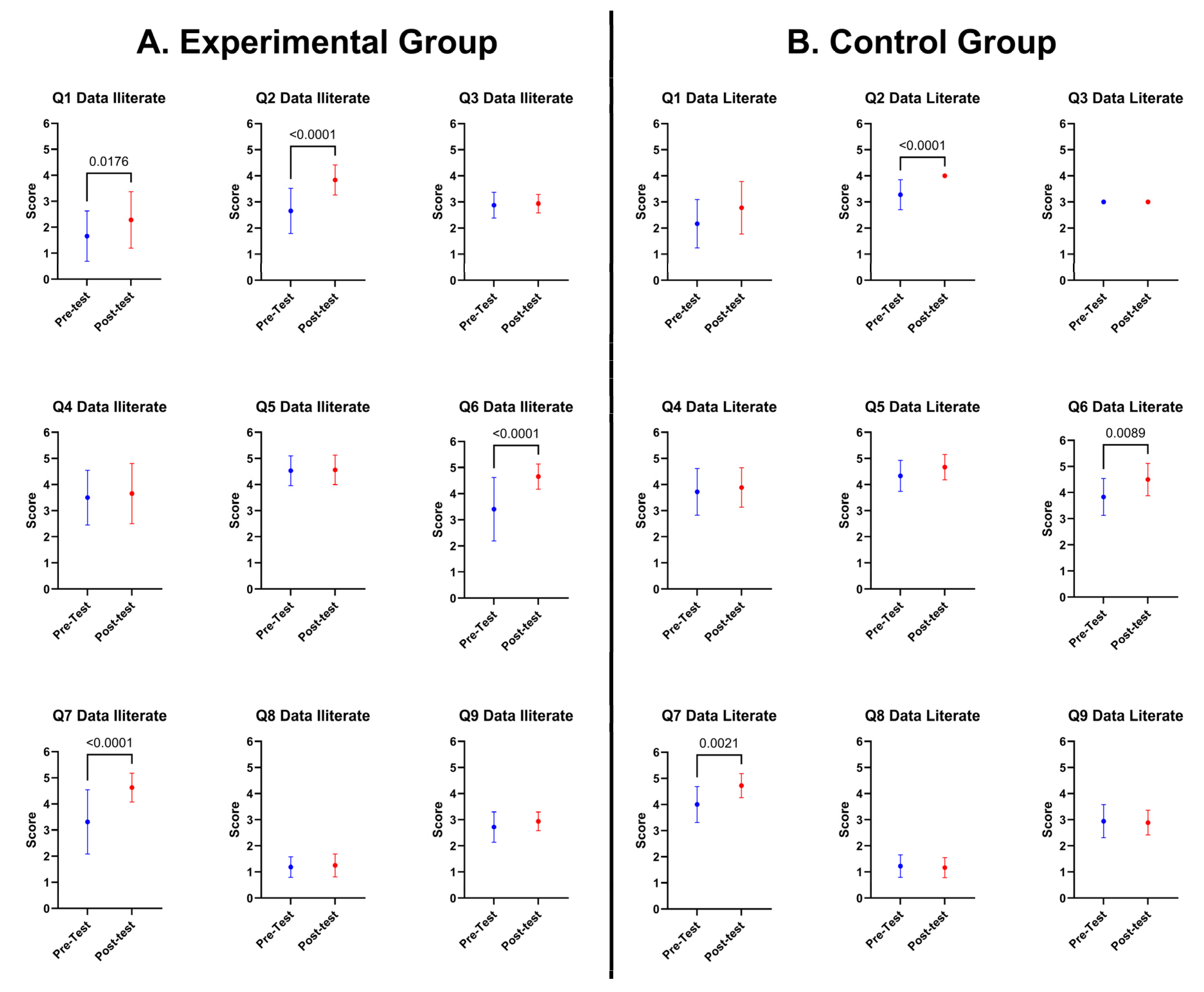
3.2. Comparison of Experimental versus Control Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ngiam, K.Y.; Khor, I.W. Big Data and Machine Learning Algorithms for Health-Care Delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Kocoń, J.; Cichecki, I.; Kaszyca, O.; Kochanek, M.; Szydło, D.; Baran, J.; Bielaniewicz, J.; Gruza, M.; Janz, A.; Kanclerz, K.; et al. ChatGPT: Jack of All Trades, Master of None. Inf. Fusion 2023, 99, 101861. [Google Scholar] [CrossRef]
- Abdullah, M.; Madain, A.; Jararweh, Y. ChatGPT: Fundamentals, Applications and Social Impacts. In Proceedings of the 2022 Ninth International Conference on Social Networks Analysis, Management and Security (SNAMS), Milan, Italy, 29 November 2022; pp. 1–8. [Google Scholar]
- Shaheen, M.Y. Applications of Artificial Intelligence (AI) in Healthcare: A Review; ScienceOpen: Berlin, Germany, 2021. [Google Scholar]
- Ali, O.; Abdelbaki, W.; Shrestha, A.; Elbasi, E.; Alryalat, M.A.A.; Dwivedi, Y.K. A Systematic Literature Review of Artificial Intelligence in the Healthcare Sector: Benefits, Challenges, Methodologies, and Functionalities. J. Innov. Knowl. 2023, 8, 100333. [Google Scholar] [CrossRef]
- Lee, D.; Yoon, S.N. Application of Artificial Intelligence-Based Technologies in the Healthcare Industry: Opportunities and Challenges. Int. J. Environ. Res. Public. Health 2021, 18, 271. [Google Scholar] [CrossRef] [PubMed]
- Boeken, T.; Feydy, J.; Lecler, A.; Soyer, P.; Feydy, A.; Barat, M.; Duron, L. Artificial Intelligence in Diagnostic and Interventional Radiology: Where Are We Now? Diagn. Interv. Imaging 2023, 104, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.S.; Judge, C.; Bollard, S.M.; Clifford, S.M.; Healy, G.M.; Aziz, A.; Mathur, P.; Islam, S.; Yeom, K.W.; Lawlor, A.; et al. Radiology Artificial Intelligence: A Systematic Review and Evaluation of Methods (RAISE). Eur. Radiol. 2022, 32, 7998–8007. [Google Scholar] [CrossRef] [PubMed]
- Najjar, R. Redefining Radiology: A Review of Artificial Intelligence Integration in Medical Imaging. Diagnostics 2023, 13, 2760. [Google Scholar] [CrossRef] [PubMed]
- Yassin, N.I.R.; Omran, S.; El Houby, E.M.F.; Allam, H. Machine Learning Techniques for Breast Cancer Computer Aided Diagnosis Using Different Image Modalities: A Systematic Review. Comput. Methods Programs Biomed. 2018, 156, 25–45. [Google Scholar] [CrossRef] [PubMed]
- Rehman, A.; Iqbal, M.A.; Xing, H.; Ahmed, I. COVID-19 Detection Empowered with Machine Learning and Deep Learning Techniques: A Systematic Review. Appl. Sci. 2021, 11, 3414. [Google Scholar] [CrossRef]
- Montemayor, C.; Halpern, J.; Fairweather, A. In Principle Obstacles for Empathic AI: Why We Can’t Replace Human Empathy in Healthcare. AI Soc. 2022, 37, 1353–1359. [Google Scholar] [CrossRef]
- Chen, M.; Zhang, B.; Cai, Z.; Seery, S.; Gonzalez, M.J.; Ali, N.M.; Ren, R.; Qiao, Y.; Xue, P.; Jiang, Y. Acceptance of Clinical Artificial Intelligence among Physicians and Medical Students: A Systematic Review with Cross-Sectional Survey. Front. Med. 2022, 9, 990604. [Google Scholar] [CrossRef]
- Kempt, H.; Nagel, S.K. Responsibility, Second Opinions and Peer-Disagreement: Ethical and Epistemological Challenges of Using AI in Clinical Diagnostic Contexts. J. Med. Ethics 2022, 48, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Sezgin, E. Artificial Intelligence in Healthcare: Complementing, Not Replacing, Doctors and Healthcare Providers. Digit. Health 2023, 9, 20552076231186520. [Google Scholar] [CrossRef]
- Sit, C.; Srinivasan, R.; Amlani, A.; Muthuswamy, K.; Azam, A.; Monzon, L.; Poon, D.S. Attitudes and Perceptions of UK Medical Students towards Artificial Intelligence and Radiology: A Multicentre Survey. Insights Imaging 2020, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Bisdas, S.; Topriceanu, C.-C.; Zakrzewska, Z.; Irimia, A.-V.; Shakallis, L.; Subhash, J.; Casapu, M.-M.; Leon-Rojas, J.; Pinto dos Santos, D.; Andrews, D.M.; et al. Artificial Intelligence in Medicine: A Multinational Multi-Center Survey on the Medical and Dental Students’ Perception. Front. Public Health 2021, 9, 795284. [Google Scholar] [CrossRef] [PubMed]
- Heredia-Negron, F.; Alamo-Rodriguez, N.; Oyola-Velazquez, L.; Nieves, B.; Carrasquillo, K.; Hochheiser, H.; Fristensky, B.; Daluz-Santana, I.; Fernandez-Repollet, E.; Roche-Lima, A. Evaluation of AIML + HDR-A Course to Enhance Data Science Workforce Capacity for Hispanic Biomedical Researchers. Int. J. Environ. Res. Public. Health 2023, 20, 2726. [Google Scholar] [CrossRef] [PubMed]
- Chew, H.S.J.; Achananuparp, P. Perceptions and Needs of Artificial Intelligence in Health Care to Increase Adoption: Scoping Review. J. Med. Internet Res. 2022, 24, e32939. [Google Scholar] [CrossRef] [PubMed]
- Castagno, S.; Khalifa, M. Perceptions of Artificial Intelligence Among Healthcare Staff: A Qualitative Survey Study. Front. Artif. Intell. 2020, 3, 578983. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Oh, S.; Kim, J.H.; Choi, S.-W.; Lee, H.J.; Hong, J.; Kwon, S.H. Physician Confidence in Artificial Intelligence: An Online Mobile Survey. J. Med. Internet Res. 2019, 21, e12422. [Google Scholar] [CrossRef]
- Mahajan, A.; Vaidya, T.; Gupta, A.; Rane, S.; Gupta, S. Artificial Intelligence in Healthcare in Developing Nations: The Beginning of a Transformative Journey. Cancer Res. Stat. Treat. 2019, 2, 182. [Google Scholar] [CrossRef]
- Yang, J.; Luo, B.; Zhao, C.; Zhang, H. Artificial Intelligence Healthcare Service Resources Adoption by Medical Institutions Based on TOE Framework. Digit. Health 2022, 8, 205520762211260. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.S.; Sawyer, J.; Luna, A.; Aoun, J.; Wang, J.; Boachie, L.; Halabi, S.; Joe, B. Perceptions of US Medical Students on Artificial Intelligence in Medicine: Mixed Methods Survey Study. JMIR Med. Educ. 2022, 8, e38325. [Google Scholar] [CrossRef] [PubMed]
- Sassis, L.; Kefala-Karli, P.; Sassi, M.; Zervides, C. Exploring Medical Students’ and Faculty’s Perception on Artificial Intelligence and Robotics. A Questionnaire Survey. J. Artif. Intell. Med. Sci. 2021, 2, 76–84. [Google Scholar] [CrossRef]
- Weidener, L.; Fischer, M. Artificial Intelligence in Medicine: Cross-Sectional Study Among Medical Students on Application, Education, and Ethical Aspects. JMIR Med. Educ. 2024, 10, e51247. [Google Scholar] [CrossRef] [PubMed]
- Kimmerle, J.; Timm, J.; Festl-Wietek, T.; Cress, U.; Herrmann-Werner, A. Medical Students’ Attitudes Toward AI in Medicine and Their Expectations for Medical Education. J. Med. Educ. Curric. Dev. 2023, 10, 23821205231219346. [Google Scholar] [CrossRef]
- Swan, B.A. Assessing the Knowledge and Attitudes of Registered Nurses about Artificial Intelligence in Nursing and Health Care. Nurs. Econ. 2021, 39, 139–143. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Knowledge | Number of Participants |
|---|---|
| Experimental Group (Data-illiterate) | 32 |
| Control Group (Data-literate) | 18 |
| Total | 50 |
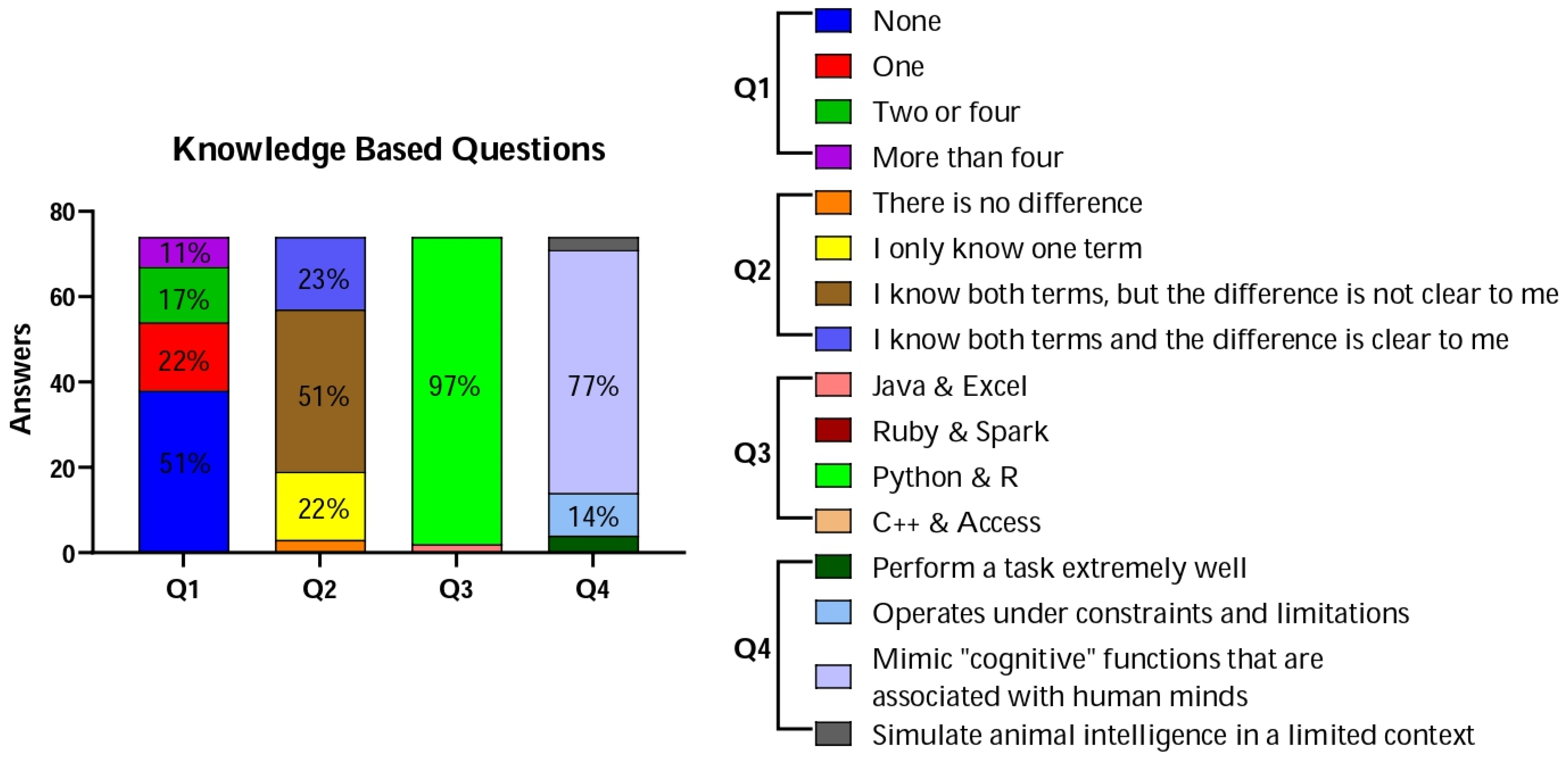
| Sections | Questions | Answers |
|---|---|---|
| Knowledge base | (Q1) How many applications of AI have you come across in your work? |
|
| (Q2) Do you know the difference between artificial intelligence, machine learning and deep learning? |
| |
| (Q3) Which of the following are two of the most important programs in Data Science? |
| |
| (Q4) The concept of artificial intelligence includes: |
| |
| Attitudes | (Q5) Do you think there may be serious ethical issues with the use of AI? |
|
| (Q6) Reasoning skills used to understand Artificial Intelligence/Data Science can be helpful to my everyday life. |
| |
| (Q7) I understand how the topic of Artificial intelligence and machine learning are applied in medicine: |
| |
| (Q8) I understand how the topic of Artificial intelligence and Machine Learning applies to Health Disparities: |
| |
| (Q9) How useful do you think AI could be in your area of work? |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heredia-Negrón, F.; Tosado-Rodríguez, E.L.; Meléndez-Berrios, J.; Nieves, B.; Amaya-Ardila, C.P.; Roche-Lima, A. Assessing the Impact of AI Education on Hispanic Healthcare Professionals’ Perceptions and Knowledge. Educ. Sci. 2024, 14, 339. https://doi.org/10.3390/educsci14040339
Heredia-Negrón F, Tosado-Rodríguez EL, Meléndez-Berrios J, Nieves B, Amaya-Ardila CP, Roche-Lima A. Assessing the Impact of AI Education on Hispanic Healthcare Professionals’ Perceptions and Knowledge. Education Sciences. 2024; 14(4):339. https://doi.org/10.3390/educsci14040339
Chicago/Turabian StyleHeredia-Negrón, Frances, Eduardo L. Tosado-Rodríguez, Joshua Meléndez-Berrios, Brenda Nieves, Claudia P. Amaya-Ardila, and Abiel Roche-Lima. 2024. "Assessing the Impact of AI Education on Hispanic Healthcare Professionals’ Perceptions and Knowledge" Education Sciences 14, no. 4: 339. https://doi.org/10.3390/educsci14040339