
Evaluating the Potential of Immersive Virtual Reality-Based Serious Games Interventions for Autism: A Pocket Guide Evaluation Framework


Abstract
:1. Introduction
- (i)
- The peculiar characteristics of the disorder, i.e., it is considered not only a disability, but also an example of human neurological variation—neurodiversity—that defines the identity of a person’s cognitive assets and challenges [46]; in fact, ASD can significantly impact the quality of life, leading to social isolation, employment difficulties, and mental health issues for individuals and their families [47,48];
- (ii)
- (iii)
2. Background
2.1. Research Method
2.1.1. Data Source and Source Strategy
(“autism spectrum disorder” OR “autism” OR “ASD”) AND (“immersive virtual reality” OR “immersive virtual environment” OR “virtual reality” OR “HMD” OR “CAVE”) AND (“serious game” OR “educational game”)
- Scopus (https://www.scopus.com, accessed on 2 April 2024)
- ACM digital library (https://dl.acm.org, accessed on 2 April 2024)
- IEEE Xplore Digital Library (https://ieeexplore.ieee.org, accessed on 2 April 2024)
- Science Direct (https://www.sciencedirect.com, accessed on 2 April 2024)
- Web of Science (http://apps.webofknowledge.com, accessed on 2 April 2024)
- PubMed (https://pubmed.ncbi.nlm.nih.gov, accessed on 2 April 2024)
- Semantic Scholar (https://www.semanticscholar.org, accessed on 2 April 2024)
- Google Scholar (https://scholar.google.com, accessed on 2 April 2024)
2.1.2. Study Selection and Quality Assessment
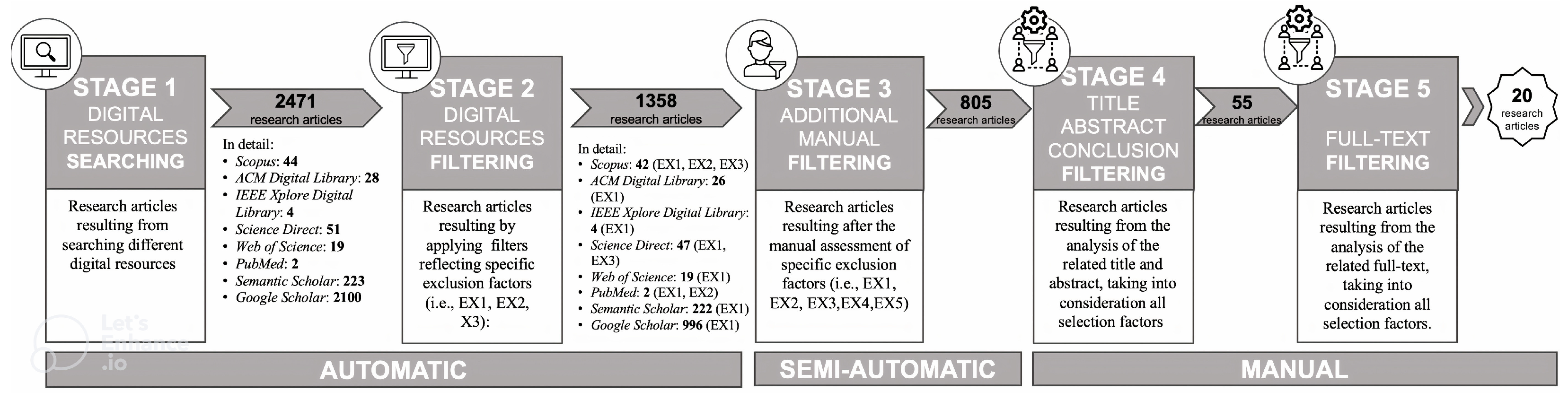
- Stage 1: Digital Resource Searching— The search string has been applied to digital resources. The search string reported in the previous subsection has been adapted in “Autism”, “Immersive Virtual Reality”, and “Serious Game” only for Semantic Scholar since it is an AI-powered digital resource that does not allow the usage of Boolean operators.
- Stage 2: Digital Resource Filtering—Filters have been applied to the output of stage 1. Filters reflected the exclusion factors of Table 3, for example, publication year (EX1) or the chosen language (EX2). According to the functionalities of digital resources, selection factors have been adequately applied (for details, see specifications under the arrow between stage 2 and stage 3 in Figure 1).
- Stage 3: Additional Semi-Automatic Filtering—The research articles obtained as output from stage 2 were collected in a unique electronic sheet by reporting the related authors’ list, title, year of publication, and source (e.g., name of the journal or conference proceedings where it was published). If there was missing information (e.g., sources), it was retrieved manually and inserted in the electronic sheet. Since many digital libraries do not provide automatic filters related to all the listed exclusion factors in Table 3, in this stage, they were applied semi-automatically. For example, many research papers that survived stage 2 were often archived twice or even three times; in stage 3, these duplicates were removed (according to EX4). Furthermore, research articles that were semi-automatically excluded were those not published in peer-reviewed journals or conference proceedings and presenting reviews or similar contributions (according to EX3). This activity was conducted by analysing the titles and sources of the retrieved research articles. Additionally, in this stage, corresponding authors of those research articles not fully available were contacted (according to EX5).
- Stage 4: Title, Abstract, and Conclusion Filtering—The 805 research articles filtered from stage 3 were, in stage 4, randomly divided into two sets of 402 and 403 research articles (denoted as StA and StB). A manual filter was applied to these two sets by analysing titles, abstracts, and conclusions. To guarantee a high quality of this manual filter, two couples composed of experts (denoted as Cp1 and Cp2) dealt with the analysis of the two sets using a cross-referenced procedure. At the end of this stage, 55 research articles survived. Cohen Kappa Statistic was performed [79] to allow for the reliability of the inclusion decision [70]. The results of Cohen K (0.90) showed an agreement of 98% among experts (Cp1 and Cp2) about the inclusion of the 55 surviving research articles.
- Stage 5: Full-text Filtering—When the research articles filtered became 55, in stage 5, they were randomly divided into two new sets of 27 and 28 research articles (denoted as StC and StD). An additional manual filter was applied by Cp1 and Cp2, analysing full texts of the research articles using a cross-referenced procedure.
2.1.3. Data Extraction
2.1.4. Data Synthesis
2.1.5. Limitations
2.2. Systematic Review Outcomes
- I1
- Multidisciplinary team. The analysis showed that 40% out of the total 20 research articles (8 of them) had a multidisciplinary team that collaborated on the design, development, and evaluation. None of them also specify the roles of each involved person on the team.
- I2
- Sample Characteristics. This involves seven sub-issues, which are:
- sI2a
- Sample size. The analysis showed that out of the total sample of 20 research articles, only 10% (2 of them) had a sample size sufficient to ensure minimum generalisability of the results (>10).
- sI2b
- Age of participants. The analysis showed that 75% of a total of 20 research articles (14 of them) specified the age of the participants.
- sI2c
- Ratio M:F. The analysis showed that 0% out of the total 20 research articles (none of them) met this ratio.
- sI2d
- ASD as the Control group. The analysis showed that only 20% out of the total 20 research articles examined (4 of them) used individuals with ASD as a control group.
- sI2e
- With or without intellectual disability. The analysis showed that 50% of the 20 research articles (10 of them) specified this cognitive characteristic of the sample. In detail, among this 50% of research articles, 80% include individuals without intellectual disabilities, and the remaining 20% include individuals with intellectual disabilities.
- sI2f
- Level of Severity. According to the DSM-5, the analysis showed that only 10% of the 20 research articles (2 of them) specified this information.
- sI2g
- Exclusion or inclusion. The analysis showed that only 10% of the 20 research articles (2 of them) specified this information.
- I3
- Experimental Design. This involves three sub-issues, which are:
- sI3a
- Statistical Design. The analysis showed that 75% out of the 20 research articles (15 of them) specified the kind of statistical design.
- sI3b
- Testing method for psychological variables. The analysis showed that 35% out of the 20 research articles (7 of them) used this sub-criterion.
- sI3c
- Testing method for technological measures. The analysis showed that 40% out of the 20 research articles (8 of them) used this sub-issue.
- I4
- Intervention. This involves five sub-issues, which are:
- sI4a
- Level of Immersion. The analysis showed that all 20 research articles do not have this sub-issue since all specified it (100%). Unfortunately, none of them used the level of immersion to verify the correlation between it and the outcome of the proposed interventions.
- sI4b
- Kind of ability. The analysis showed that all 20 research articles do not have this sub-issue since all specified it (100%). Unfortunately, none of them used a classifier to define the kind of ability. In the present systematic review, the classifier called American Association on Intellectual and Developmental Disabilities [80] was used. In this way, a more detailed analysis regarding the kind of ability addressed by the 20 research articles is provided. Specifically, 25% of them covered two types of skills, including social and conceptual skills: 45% social skills, 50% conceptual skills, and, finally, 30% practical skills.
- sI4c
- Engagement. The analysis showed that 35% of the 20 research articles (7 of them) considered this sub-issue.
- sI4d
- Acceptability. The analysis showed that 35% of the 20 research articles (7 of them) considered this sub-issue.
- sI4e
- Usability. The analysis showed that 20% out of the total 20 research articles (4 of them) considered this sub-issue.
- I5
- Level of Aversion or Negative Effect of IVR technology. The analysis showed that 15% out of the total 20 research articles (3 of them) reported the presence of these effects.
- I6
- Ethical aspects. The analysis showed that 40% out of the total 20 research articles (exactly 8 of them) disclosed that their study was approved by an ethics committee. The latter result is worrisome since it was predictable that this criterion obtains a score of 100% to safeguard both the individuals with ASD and the research team.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Issues and Sub-Issues | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
I1 (Multidisc. Team) | I2 (Sample Characteristics) |
I3 (Experimental Design) | I4 (Intervention) | I5 (Level of Aversion or Negative Effect) | I6 (Ethical Aspects) | ||||||||||||||
| sI2a | sI2b | sI2c | sI2d | sI2e | sI2f | sI2g | sI3a | sI3b | sI3c | sI4a | sI4b | sI4c | sI4d | sI4e | |||||
| References | [81] | x | x | x | x | x | x | x | x | x | |||||||||
| [82] | x | x | x | x | x | x | x | x | |||||||||||
| [83] | x | x | x | x | x | x | x | x | |||||||||||
| [84] | x | x | x | x | x | x | x | x | |||||||||||
| [85] | x | x | x | x | x | x | x | x | |||||||||||
| [86] | x | x | x | x | x | ||||||||||||||
| [87] | x | x | x | ||||||||||||||||
| [88] | x | x | x | x | x | x | x | x | |||||||||||
| [89] | x | x | x | x | x | x | x | x | x | x | |||||||||
| [90] | x | x | x | x | x | x | x | x | |||||||||||
| [91] | x | x | x | x | x | x | x | ||||||||||||
| [92] | x | x | x | x | x | x | x | ||||||||||||
| [93] | x | x | x | x | x | x | x | x | x | ||||||||||
| [94] | x | x | x | x | x | x | x | x | |||||||||||
| [95] | x | x | x | ||||||||||||||||
| [96] | x | x | |||||||||||||||||
| [97] | x | x | x | x | x | x | x | x | x | ||||||||||
| [98] | x | x | x | x | x | x | x | x | |||||||||||
| [99] | x | x | x | x | x | ||||||||||||||
| [100] | x | x | x | x | x | x | x | x | x | ||||||||||
| % Coverage | 40% | 10% | 75% | 0% | 20% | 50% | 10% | 10% | 75% | 35% | 40% | 20% | 20% | 35% | 35% | 20% | 15% | 40% | |
| ID | Methodological Issue | Methodological Sub-Issue | Existing | To Add |
|---|---|---|---|---|
| I1 | Multidisciplinary Team | x | x* | |
| I2 | Sample Characteristics | |||
| sI2a | Sample Size | x | x* | |
| sI2b | Age of Participants | x | x* | |
| sI2c | Ratio Male:Female | — | x** | |
| sI2d | ASD as the Control Group | x | x* | |
| sI2e | With or Without Intellectual Disability | x | x⌃ | |
| sI2f | Level of Severity according to DSM-5 | x | x* | |
| sI2g | Excluded/Included CR | x | x* | |
| I3 | Experimental Design | |||
| sI3a | Statistical Design | x | x* | |
| sI3b | Testing Methods- Psychological Variables | x | x* | |
| sI3c | Testing Methods- Technological Measures | x | x* | |
| I4 | Intervention | |||
| sI4a | Level of Immersion | x | — | |
| sI4b | Kind of Ability | x | x* | |
| sI4c | Engagement | x | x* | |
| sI4d | Acceptability | x | x* | |
| sI4e | Usability | x | x* | |
| I5 | Level of Aversion or Negative Effects of IVR Technology | x | x* | |
| I6 | Ethical Aspects | x | x* |
3. Results and Research Implications
3.1. From Methodological Issues to Methodological Criteria
- C1
- Multidisciplinary team. It is recommended to have a multidisciplinary team that collaborates on the design, implementation, and evaluation of an IVR-based SG intervention for ASD. The team should include domain experts, such as experienced autism spectrum disorder psychologists, educators, and information and communication technology experts. The multidisciplinary team is particularly crucial when the technological system targets a clinical population, such as individuals with autism spectrum disorder [30,32,33,34]. It is desirable that in the design and development stages of technologies for ASD (e.g., [10,102,103]), end users and other stakeholders (e.g., family and caregivers) are also involved in making decisions about what is developed and how. This approach follows an inclusive and participatory methodology that is ethically more appropriate for designers and end products. Indeed, end users and other stakeholders are involved from the beginning of the process rather than being product testers [104,105,106,107]. Likewise, an inclusive and participatory methodology provides superior protection of the ethical aspects for autism spectrum disorder individuals [108,109,110].
- C2
- Sample Characteristics. This methodological criterion involves seven sub-criteria:
- sC2a
- Sample size. In order to ensure the discrete generalisability of the results, a sample size of at least ≥30 is recommended since it allows the distribution to be nearly identical to the normal curve. The need for a normal curve derives from the fact that it is the most common curve in nature if it assumes that the influences on the results are truly random. However, when the sample consists of clinical subjects, such as autism spectrum disorder individuals, it is much more complicated to ensure an adequate sample size. In order to overcome this issue, it is recommended to use a statistical test known as Power Analysis [111] at the beginning of the study to determine the appropriate sample size according to the research question.
- sC2b
- Age of participants. It is recommended to conduct studies with clustered age groups according to a universal age classification system, for instance, the one proposed by the World Health Organization, since most abilities are age-dependent.
- sC2c
- Ratio M:F. It is recommended that the sample under a study respects the male-to-female ratio of around 3:1 [57] since completely neglecting a component of the autism spectrum disorder population, even with a lower prevalence, could constitute a notable methodological issue.
- sC2d
- ASD as the control group. It is recommended that the entire experimental and control sample under a study consists of individuals with autism spectrum disorder. It is necessary to check the methodological criterion of inter-group comparability [112,113] by ensuring that the experimental intervention is the only discriminating variable between the two samples.
- sC2e
- With or without intellectual disability. It is recommended that studies provide information on the presence or absence of intellectual disability tested by specific and standardised tests since this information is essential for all aspects of research, from technology design to the type of skill to be treated.
- sC2f
- Level of severity according to DSM-5 It is recommended that studies published post-2013 define the level of autism spectrum disorder severity according to the DSM-5 [60] instead of using outdated diagnostic classifications, such as Asperger’s Syndrome. It would allow for appropriate and current diagnostic uniformity.
- sC2g
- Exclusion or inclusion. It is recommended to use both inclusion and exclusion sub-criteria. The first since ensuring that key characteristics of a target population are selected; the second since ensuring that potential participants that met the inclusion sub-criteria but have additional characteristics that could interfere with the success of the study are excluded [114,115]. Having inclusion and exclusion sub-criteria for clinical study participants is a standard, required practice for designing high-quality research protocols to ensure the generalisability of the results [115].
- C3
- Experimental Design. This methodological criterion involves three sub-criteria:
- sC3a
- Statistical Design. At the beginning of a study, it is recommended that studies plan the statistical analysis according to the specific research question. This planning allows for a methodologically controlled definition of the variables being studied. Likewise, all studies should always include a follow-up since it is necessary to verify the efficacy and effectiveness of an intervention over time [116,117,118].
- sC3b
- sC3c
- C4
- Intervention. This methodological criterion involves five sub-criteria:
- sC4a
- Level of Immersion. Immersive virtual reality can have low, moderate, or high levels of immersion. It is recommended that studies specify the level of immersion and that they specify how much the level of immersion goes into impacting the outcome of the intervention.
- sC4b
- Kind of ability. It is recommended to define the type of ability focus of the research based on a known classifier, for example, the one proposed by the American Association on Intellectual and Developmental Disabilities [80], ensuring standard definitions enjoyable by different professional profiles.
- sC4c
- Engagement. It is recommended to evaluate engagement because if the study participants are not involved enough, they will not continue to use the system. Specifically, it is recommended to use objective measures to evaluate engagement, such as standardised tests and questionnaires that ensure replicable results (see, e.g., [9,24]).
- sC4d
- Acceptability. It is recommended, at the beginning of an intervention, to evaluate the acceptability for the success of it. For example, if an individual with severe autism spectrum disorder does not tolerate the use of HMD, an intervention implemented through an HMD may not be carried out. Specifically, evaluating the acceptability using standardised tests and questionnaires (e.g., Simulator Sickness Questionnaire [121]) that ensure replicable results is recommended (see, e.g., [9,24]).
- sC4e
- Usability. It is recommended to evaluate the usability since it is essential for proper human–computer interaction during the intervention. Specifically, it is recommended to use objective measures to evaluate usability, such as standardised tests and questionnaires that ensure replicable results (see, e.g., [9,122]).
- C5
- Level of Aversion or Negative Effect of IVR technology. It is recommended to consider this criterion since it is critical for the success of the intervention, especially for the clinical populations (e.g., [9,123,124]). Indeed, the intervention may be marred by several negative effects that are related to the use of immersive virtual reality [125]. These include cybersickness [125,126,127]. Cybersickness refers to a set of symptoms that can affect people when using immersive virtual reality technologies. These symptoms are like motion sickness and can include dizziness, headaches, eye fatigue, vertigo, and disorientation. Factors that can cause and exacerbate cybersickness include prolonged exposure to an immersive virtual reality-based experience, rapid movement in the field of view, lack of control over the immersive virtual environment, poor frame rate, and graphics quality [128]. Therefore, negative effects and recommendations for the use of such technology must necessarily be taken into account.
- C6
- Ethical aspects. It is recommended to have ethics committee approval before starting a study (for more detail, see [129]). An ethics committee must be declared within a study. Before starting the study, the study protocol must undergo evaluation and approval from an accredited research ethics committee [130,131,132,133,134]. This committee must maintain impartiality and transparency, free from conflicts of interest with researchers or sponsoring institutions. Protocol breaches or adverse events during the study should be reported promptly to the committee following established regulations [130,131,132,133,134]. Clinical studies must evaluate potential risks and benefits for participants. Researchers should minimise risks, monitor them continuously, and record risk factors. Participants should be fully informed about the study, voluntarily provide informed consent, and receive comprehensive information about the research, including purpose, method, expected benefits and risks, and conflicts of interest [130,131,132,133,134]. If a participant cannot provide consent, it must be obtained through a legally authorised representative (informed consent) [130,131,132,133,134].
- (i)
- It is the result of a rigorous research method related to planning, conducting, and inferring the results of a systematic review, i.e., Kitchenam’s method [70];
- (ii)
- Kitchenam’s rigorous method [70] was, in our case, enriched by the study of recent literature on this topic (e.g., [61,63,64,65,66]) and by the hard work conducted by a balanced multidisciplinary team of two psychologists with expertise in autism and research methodology and two ICT experts, especially in designing and developing IVR-based systems and SG;
- (iii)
- The indications or suggestions provided for addressing each of the six methodological criteria and their sub-criteria are supported by established scientific evidence. For example, it is known from the relevant scientific literature [60,113] that the diagnosis of ASD as well as the indication of the level of severity of the disorder should be by the Diagnostic and Statistical Manual of Mental Disorders-5th (DSM-5). Therefore, to meet the Level of severity according to DSM-5 sub-criterion of the Sample Size methodological criterion, it is suggested to refer to DSM-5 and not to old diagnostic labels, such as Asperger’s Syndrome. Along these lines, we have suggested what is most scientifically established for all methodological criteria and sub-criteria.
3.2. Research and Practitioners Implications: A Pocket Guide Evaluation Framework
- Concerning the final users who will use the proposed Evaluation Framework, they are psychologists who are experts in research methodology but generally not experts in using technological devices. Likewise, they are confident with traditional, not advanced, easy-to-use technological devices and tools, such as computers and PowerPoint presentations, that are used from the very early years of university and clinical training.
- In relation to the context of use in which the Evaluation Framework will be used, it is generally an indoor environment, and we do not expect it to be equipped with specific advanced technological equipment, such as high-performance network connectivity or robust internet access, as well as head-mounted displays. However, since this environment is still a highly professionalising context of use (e.g., academia or clinics), we guess there is, in the worst case, at least a computer.
- Static Part—The PowerPoint Presentation incorporates a dedicated slide for each methodological criterion and sub-criterion. Each slide includes the following elements: (1) the name of the methodological criterion/sub-criterion, (2) a description of the methodological criterion/sub-criterion, (3) a visual representation of the methodological criterion/sub-criterion in the form of an icon to enhance understanding and retention, and (4) a TO-DO list of practical actions to address the associated methodological criterion/sub-criterion. Additionally, the PowerPoint presentation includes a brief overview of the Evaluation Framework and instructions on how to use and interact with it. Furthermore, a 6-colour rainbow palette is employed, with each colour corresponding to a specific methodological criterion.
- Dynamic Part—The PowerPoint presentation offers two distinct approaches in browsing the Evaluation Framework. The first approach involves traditional linear navigation, where users can browse through the PowerPoint presentation using mouse clicks, the space bar, or arrow keys. This method is commonly familiar to the final users of the proposed Evaluation Framework. The second approach incorporates more interactive and nonlinear navigation, resembling the browsing found on websites. In fact, a main navigation menu is located at the top of each slide, allowing final users to quickly access different methodological criteria included in the Evaluation Framework. This navigation menu consists of seven items: an “Introduction” item and six items, each representing a specific methodological criterion. By clicking on a particular item, the corresponding slide is displayed (see, for example, Figure 2). Notably, when final users click on an item related to a methodological criterion that includes sub-criteria, a contextual sub-menu appears beneath the main navigation menu (see, for example, Figure 3 and Figure 4). This sub-menu enables final users to explore and interact with all the associated methodological sub-criteria.
3.3. Utilising the Pocket Guide Evaluation Framework: An Example of Its Application
- Research Question: Is an Immersive Virtual Reality-based Serious Game intervention more effective than a traditional non-technology mediated approach in enhancing social cognition skills in adolescents with ASD?
- Research Hypothesis: Researchers anticipate that employing an Immersive Virtual Reality-based Serious Game, with its immersive technology and serious game learning strategy, will be more effective in enhancing social cognition skills among adolescents with ASD compared to traditional interventions (e.g., Multimodal Anxiety and Social Skill Intervention for Adolescents with Autism Spectrum Disorder [140]).
- C1
- Multidisciplinary team. We plan to engage psychologists with a background in ASD interventions for social cognition, as well as experts in ICT, SG, and IVR from the early stages of the study.
- C2
- Sample Characteristics.
- sC2a
- Sample size. To determine the sample size for our future study, we will employ power analysis [111], given the challenge of recruiting adolescents with ASD, particularly for the IVR-mediated experimental condition. We guess, as a result of our power analysis, that we will have to reach a minimum total sample size of 55 individuals to ensure that the study has adequate statistical power to detect significant effects or differences.
- sC2b
- Age of participants. The study will be conducted on a group of 55 ASD adolescents with a range of ages 13–15.
- sC2c
- Ratio M:F. The sample of 55 adolescents with ASD will be composed of 41 males and 12 females to reflect the male-to-female ratio around 3:1 [57].
- sC2d
- ASD as the control group. To check the methodological criterion of inter-group comparability [112,113], the control group will consist of adolescents with autism. Therefore, the sample of 55 persons will be randomly divided as follows: the experimental group (SG intervention based on IVR) will contain 28 adolescents with ASD (20 males and 8 females); the control group (traditional non-technology mediated intervention) will contain 27 adolescents with ASD (20 males and 7 females).
- sC2e
- With or without intellectual disability. All 55 participants in the study will not have an intellectual disability.
- sC2f
- Level of severity according to DSM-5 All 55 study participants will have a diagnosis of ASD with severity level 1 (support needed), i.e., the least impaired condition.
- sC2g
- Exclusion or inclusion. The following exclusion criteria will be set: (1) all individuals with an intellectual disability; (2) all individuals with psychiatric disorders in comorbidity; (3) all individuals who have had previous negative experiences with IVR; (4) all individuals who have a history of epileptic seizures; (5) all individuals who suffer from emotional sickness; (6) all individuals with a diagnosis of autism with a severity level other than 1; (7) all individuals who are adolescents but not in the age range 13–15.
- C3
- Experimental Design.
- sC3a
- Statistical design. The statistical design of the study will be a between-group comparison. A follow-up will also be planned to monitor the effects of both interventions.
- sC3b
- sC3c
- Testing method for technological measures. Usability, acceptability, and negative effects will be assessed by means of standardised questionnaires (e.g., Virtual Reality Usability Questionnaire [144] and Simulator Sickness Questionnaire [121]). In addition, the engagement of participants will also be assessed through selected behavioural observation measures [9,24].
- C4
- Intervention.
- sC4a
- sC4b
- Kind of ability. In this future study, the target abilities will be those of social cognition, which, according to the American Association on Intellectual and Developmental Disabilities [80], fall under the category of social skills.
- sC4c
- Engagement. For the assessment of engagement, several metrics will be set according to a Likert scale (e.g., 1–5) in terms of emotional participation, suspension of disbelief (i.e., the extent to which the virtual world is temporarily accepted as reality); bodily participation (i.e., the extent of body movement during the immersive experience); virtual world exploration [9,24]).
- sC4d
- Acceptability. Acceptability will be measured by means of the standardised Simulator Sickness Questionnaire test [121]. In addition, acceptability for the use of HMD will be examined in terms of readiness for use and a number of factors related to possible unpleasant physiological effects or discomfort (e.g., motion sickness and digital eye fatigue) measured as dichotomous values (i.e., yes or no).
- sC4e
- Usability. Usability will be measured using the Virtual Reality Usability Questionnaire [144]. In addition, we assessed usability by looking at the following aspects: autonomy in handling the device (e.g., support required from operators during the study).
- C5
- Level of aversion or negative effect of IVR technology. All factors that could increase the risk of cybersickness (e.g., rapid movement in the field of view and poor frame rate) will be considered in the design process. In addition, the standardised Simulator Sickness Questionnaire [121] will be used to assess the level of cybersickness experienced by users. All participants will be instructed to stop the study if they experience symptoms of cybersickness.
- C6
- Ethical aspects. Participants will have been tested individually in a quiet room according to the principles established by the Declaration of Helsinki. The pre-departure investigation will be approved by the Ethics Committee of Hospital XXX (report the number code), which will approve the experimental protocol before participants are recruited, according to the principles established by the Declaration of Helsinki. Written informed consent will be obtained from all accompanying persons of participants prior to the study.
4. Conclusions and Future Work
- (i)
- Methodological issues were transformed into methodological criteria necessary to conduct a rigorous evaluation. The quality of the transformation process from methodological issues to methodological criteria was ensured by at least three aspects. First, they are the results of a rigorous research methodology approach in planning, conducting, and inferring the results of a systematic review, i.e., Kitchenam’s method [70]. Secondly, Kitchenam’s method [70] was enhanced by the study of recent literature on this topic, e.g., [61,62,63,64,65,66,67,68] and by the strenuous efforts of a well-balanced multidisciplinary team, consisting of two psychologists skilled in autism and research methodology and two ICT experts specialising in designing and developing IVR-based systems and SG. Lastly, the guidelines to address the methodological criteria and their sub-criteria are firmly rooted in established scientific evidence.
- (ii)
- A usable tool was proposed for the methodological criteria to become an Evaluation Framework. The quality of the process involved in designing and developing the Evaluation Framework is assured by adopting a user-centred approach [136], which places particular emphasis on the end-users, such as psychologists experienced in research methodology, and the context of use, typically research centres, hospitals, and clinics [30,32,33,34]. The dedicated efforts of our multidisciplinary team further enriched this user-centred approach: the decision to select a usable tool for disseminating the Evaluation Framework resulted from the joining of different professional profiles proficient in all the necessary aspects for creating and using such a framework.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASD | Autism Spectrum Disorders |
| ICT | Information and Communication Technologies |
| STEM | Science, Technology, Engineering, and Mathematics |
| IVR | Immersive Virtual Reality |
| SG | Serious Game |
| HMD | Head-Mounted Display |
| CAVE | Cave Automatic Virtual Environment |
| AI | Artificial Intelligence |
References
- Karami, B.; Koushki, R.; Arabgol, F.; Rahmani, M.; Vahabie, A.H. Effectiveness of virtual/augmented reality–based therapeutic interventions on individuals with autism spectrum disorder: A comprehensive meta-analysis. Front. Psychiatry 2021, 12, 665326. [Google Scholar] [CrossRef] [PubMed]
- Billard, A.; Robins, B.; Nadel, J.; Dautenhahn, K. Building Robota, a mini-humanoid robot for the rehabilitation of children with autism. Assist. Technol. 2007, 19, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Dautenhahn, K. Roles and functions of robots in human society: Implications from research in autism therapy. Robotica 2003, 21, 443–452. [Google Scholar] [CrossRef]
- DiPietro, J.; Kelemen, A.; Liang, Y.; Sik-Lanyi, C. Computer-and robot-assisted therapies to aid social and intellectual functioning of children with autism spectrum disorder. Medicina 2019, 55, 440. [Google Scholar] [CrossRef] [PubMed]
- Moghadas, M.; Moradi, H. Analyzing human-robot interaction using machine vision for autism screening. In Proceedings of the 2018 6th RSI international conference on robotics and mechatronics (IcRoM), Tehran, Iran, 23–25 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 572–576. [Google Scholar] [CrossRef]
- Bozgeyikli, L.; Raij, A.; Katkoori, S.; Alqasemi, R. A survey on virtual reality for individuals with autism spectrum disorder: Design considerations. IEEE Trans. Learn. Technol. 2017, 11, 133–151. [Google Scholar] [CrossRef]
- Valentine, A.Z.; Brown, B.J.; Groom, M.J.; Young, E.; Hollis, C.; Hall, C.L. A systematic review evaluating the implementation of technologies to assess, monitor and treat neurodevelopmental disorders: A map of the current evidence. Clin. Psychol. Rev. 2020, 80, 101870. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ding, H.; Naumceska, M.; Zhang, Y. Virtual reality technology as an educational and intervention tool for children with autism spectrum disorder: Current perspectives and future directions. Behav. Sci. 2022, 12, 138. [Google Scholar] [CrossRef] [PubMed]
- Di Mascio, T.; Tarantino, L.; De Gasperis, G.; Pino, M.C. Immersive virtual environments: A comparison of mixed reality and virtual reality headsets for ASD treatment. Adv. Intell. Syst. Comput. 2020, 1007, 153–163. [Google Scholar] [CrossRef]
- Di Mascio, T.; Tarantino, L.; Cirelli, L.; Peretti, S.; Mazza, M. Designing a personalizable ASD-oriented AAC tool: An action research experience. Adv. Intell. Syst. Comput. 2019, 804, 200–209. [Google Scholar] [CrossRef]
- Mazza, M.; Pino, M.C.; Vagnetti, R.; Peretti, S.; Valenti, M.; Marchetti, A.; Di Dio, C. Discrepancies between explicit and implicit evaluation of aesthetic perception ability in individuals with autism: A potential way to improve social functioning. BMC Psychol. 2020, 8, 74. [Google Scholar] [CrossRef]
- Baron-Cohen, S. Autism and the technical mind. Sci. Am. 2012, 307, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Yu, J.W.; Shattuck, P.; McCracken, M.; Blackorby, J. Science, technology, engineering, and mathematics (STEM) participation among college students with an autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Di Mascio, T.; Laura, L.; Temperini, M. A framework for personalized competitive programming training. In Proceedings of the 2018 17th International Conference on Information Technology Based Higher Education and Training (ITHET), Olhao, Portugal, 26–28 April 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1–8. [Google Scholar] [CrossRef]
- Glaser, N.; Schmidt, M.; Schmidt, C.; Palmer, H.; Beck, D. The centrality of interdisciplinarity for overcoming design and development constraints of a multi-user virtual reality intervention for adults with Autism: A design case. In Intersections Across Disciplines: Interdisciplinarity and Learning; Springer: Berlin/Heidelberg, Germany, 2021; pp. 157–171. [Google Scholar] [CrossRef]
- Drigas, A.; Vlachou, J.A. Information and communication technologies (ICTs) and autistic spectrum disorders (ASD). Int. J. Recent Contrib. Eng. Sci. IT iJES 2016, 4, 4–10. [Google Scholar] [CrossRef]
- Høeg, E.R.; Povlsen, T.M.; Bruun-Pedersen, J.R.; Lange, B.; Nilsson, N.C.; Haugaard, K.B.; Faber, S.M.; Hansen, S.W.; Kimby, C.K.; Serafin, S. System immersion in virtual reality-based rehabilitation of motor function in older adults: A systematic review and meta-analysis. Front. Virtual Real. 2021, 2, 647993. [Google Scholar] [CrossRef]
- Glaser, N.; Schmidt, M. Systematic Literature Review of Virtual Reality Intervention Design Patterns for Individuals with Autism Spectrum Disorders. Int. J. Hum.-Comput. Interact. 2021, 38, 753–788. [Google Scholar] [CrossRef]
- Caruso, F.; Peretti, S.; Barletta, V.S.; Pino, M.C.; Di Mascio, T. Recommendations for developing Immersive Virtual Reality Serious Game for Autism: Insights from a Systematic Literature Review. IEEE Access 2023, 11, 74898–74913. [Google Scholar] [CrossRef]
- Meadan, H.; Ostrosky, M.M.; Triplett, B.; Michna, A.; Fettig, A. Using visual supports with young children with autism spectrum disorder. Teach. Except. Child. 2011, 43, 28–35. [Google Scholar] [CrossRef]
- Schmidt, M.; Schmidt, C.; Glaser, N.; Beck, D.; Lim, M.; Palmer, H. Evaluation of a spherical video-based virtual reality intervention designed to teach adaptive skills for adults with autism: A preliminary report. Interact. Learn. Environ. 2021, 29, 345–364. [Google Scholar] [CrossRef]
- Peretti, S.; Caruso, F.; Pino, M.C.; Di Mascio, T. A systematic review to know how interventions realized with immersive virtual reality-based serious games for individuals with autism are evaluated. In Proceedings of the 5th Biannual Conference of the Italian SIGCHI Chapter: Crossing HCI and AI, CHItaly 2023, Torino, Italy, 20–22 September 2023; pp. 1–14. [Google Scholar] [CrossRef]
- Miller, H.L.; Bugnariu, N.L. Level of immersion in virtual environments impacts the ability to assess and teach social skills in autism spectrum disorder. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 246–256. [Google Scholar] [CrossRef]
- Tarantino, L.; De Gasperis, G.; Di Mascio, T.; Pino, M.C. Immersive applications: What if users are in the autism spectrum? In Proceedings of the 17th International Conference on Virtual-Reality Continuum and Its Applications in Industry, VRCAI ’19, Brisbane, QLD, Australia, 14–16 November 2019. [Google Scholar] [CrossRef]
- Camargo, M.C.; Barros, R.M.; Brancher, J.D.; Barros, V.T.; Santana, M. Designing gamified interventions for autism spectrum disorder: A systematic review. In Proceedings of the Joint International Conference on Entertainment Computing and Serious Games, Arequipa, Peru, 11–15 November 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 341–352. [Google Scholar] [CrossRef]
- Tsikinas, S.; Xinogalos, S. Studying the effects of computer serious games on people with intellectual disabilities or autism spectrum disorder: A systematic literature review. J. Comput. Assist. Learn. 2019, 35, 61–73. [Google Scholar] [CrossRef]
- Maria Kellidou, P.; Kotzageorgiou, M.; Voulgari, I.; Nteropoulou Nterou, E. A review of digital games for children with autism spectrum disorder. In Proceedings of the 9th International Conference on Software Development and Technologies for Enhancing Accessibility and Fighting Info-Exclusion, Online, Portugal, 2–4 December 2020; pp. 227–234. [Google Scholar] [CrossRef]
- Valencia, K.; Rusu, C.; Quiñones, D.; Jamet, E. The impact of technology on people with autism spectrum disorder: A systematic literature review. Sensors 2019, 19, 4485. [Google Scholar] [CrossRef]
- Whyte, E.M.; Smyth, J.M.; Scherf, K.S. Designing serious game interventions for individuals with autism. J. Autism Dev. Disord. 2015, 45, 3820–3831. [Google Scholar] [CrossRef] [PubMed]
- Caruso, F.; Di Mascio, T. Designing IVR Serious Games for People with ASD: An innovative Approach. Adv. Intell. Syst. Comput. 2021, 1236 AISC, 291–295. [Google Scholar] [CrossRef]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.A.; Gil-Gómez, J.A. Effectiveness of virtual reality for children and adolescents with autism spectrum disorder: An evidence-based systematic review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef] [PubMed]
- Barletta, V.S.; Caruso, F.; Di Mascio, T.; Piccinno, A. Serious games for autism based on immersive virtual reality: A lens on methodological and technological challenges. In Lecture Notes in Networks and Systems; Springer: Berlin/Heidelberg, Germany, 2023; Volume 580, pp. 181–195. [Google Scholar] [CrossRef]
- Dechsling, A.; Orm, S.; Kalandadze, T.; Sütterlin, S.; Øien, R.A.; Shic, F.; Nordahl-Hansen, A. Virtual and augmented reality in social skills interventions for individuals with autism spectrum disorder: A scoping review. J. Autism Dev. Disord. 2021, 52, 4692–4707. [Google Scholar] [CrossRef] [PubMed]
- Grossard, C.; Grynspan, O.; Serret, S.; Jouen, A.L.; Bailly, K.; Cohen, D. Serious games to teach social interactions and emotions to individuals with autism spectrum disorders (ASD). Comput. Educ. 2017, 113, 195–211. [Google Scholar] [CrossRef]
- Godwin, M.; Ruhland, L.; Casson, I.; MacDonald, S.; Delva, D.; Birtwhistle, R.; Lam, M.; Seguin, R. Pragmatic controlled clinical trials in primary care: The struggle between external and internal validity. BMC Med. Res. Methodol. 2003, 3, 28. [Google Scholar] [CrossRef] [PubMed]
- Gartlehner, G.; Hansen, R.; Nissman, D.; Lohr, K.; Carey, T. Criteria for distinguishing effectiveness from efficacy trials in systematic reviews. Agency Healthc. Res. Qual. 2006.
- Hoagwood, K.; Hibbs, E.; Brent, D.; Jensen, P. Introduction to the special section: Efficacy and effectiveness in studies of child and adolescent psychotherapy. J. Consult. Clin. Psychol. 1995, 63, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.D.; Steele, R.G. Beyond efficacy and effectiveness: A multifaceted approach to treatment evaluation. Prof. Psychol. Res. Pract. 2006, 37, 389–397. [Google Scholar] [CrossRef]
- Lachin, J.M. The role of measurement reliability in clinical trials. Clin. Trials 2004, 1, 553–566. [Google Scholar] [CrossRef] [PubMed]
- Mohajan, H.K. Two criteria for good measurements in research: Validity and reliability. In Annals of Spiru Haret University, Economic Series; Editura Fundaţiei România de Mâine: Romania, Bucharest, 2017; Volume 17, pp. 59–82. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Reproducibility and Replicability in Science; National Academies Press: Washington, DC, USA, 2019. [Google Scholar]
- Wade, D.T.; Smeets, R.J.; Verbunt, J.A. Research in rehabilitation medicine: Methodological challenges. J. Clin. Epidemiol. 2010, 63, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.E.; Karmarkar, A.M.; Ottenbacher, K.J. Small sample research designs for evidence-based rehabilitation: Issues and methods. Arch. Phys. Med. Rehabil. 2012, 93, S111–S116. [Google Scholar] [CrossRef] [PubMed]
- Monge, J.; Ribeiro, G.; Raimundo, A.; Postolache, O.; Santos, J. AI-Based Smart Sensing and AR for Gait Rehabilitation Assessment. Information 2023, 14, 355. [Google Scholar] [CrossRef]
- Engle, R.L.; Mohr, D.C.; Holmes, S.K.; Seibert, M.N.; Afable, M.; Leyson, J.; Meterko, M. Evidence-based practice and patient-centered care: Doing both well. Health Care Manag. Rev. 2021, 46, 174–184. [Google Scholar] [CrossRef]
- Lai, M.C.; Anagnostou, E.; Wiznitzer, M.; Allison, C.; Baron-Cohen, S. Evidence-based support for autistic people across the lifespan: Maximising potential, minimising barriers, and optimising the person–environment fit. Lancet Neurol. 2020, 19, 434–451. [Google Scholar] [CrossRef] [PubMed]
- Eaves, L.C.; Ho, H.H. Young adult outcome of autism spectrum disorders. J. Autism Dev. Disord. 2008, 38, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Bellani, M.; Fornasari, L.; Chittaro, L.; Brambilla, P. Virtual reality in autism: State of the art. Epidemiol. Psychiatr. Sci. 2011, 20, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Autism and Developmental Disabilities Monitoring Network Surveillance Year 2002 Principal Investigators; Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders–autism and developmental disabilities monitoring network, 14 sites, United States, 2002. In MMWR. Surveillance Summaries: Morbidity and Mortality Weekly Report. Surveillance Summaries/CDC; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2007; Volume 56. [Google Scholar]
- Centers for Disease Control and Prevention. Brief update: Prevalence of autism spectrum disorders (ASDs) — autism and developmental disabilities monitoring (ADDM) network, United States, 2004. In Morbidity and Mortality Weekly Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2009; Volume 58. [Google Scholar]
- Centers for Disease Control and Prevention. Morbidity and mortality weekly report prevalence of autism spectrum disorders—Autism and developmental disabilities monitoring network, United States, 2006. In Morbidity and Mortality Weekly Report. Surveillance Summaries. (Washington, DC: 2009); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2009; Volume 58. [Google Scholar]
- Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders—Autism and developmental disabilities monitoring network, 14 sites, United States, 2008. In Morbidity and Mortality Weekly Report: Surveillance Summaries; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2012; Volume 61, pp. 1–19. [Google Scholar]
- Centers for Disease Control and Prevention. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2010. In MMWR Surveillance Summaries; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2014; Volume 63. [Google Scholar]
- Anorson, N.; Male, I.; Farr, W.; Memon, A. Prevalence of autism in Europe, North America and Oceania, 2000–2020: A systematic review. Eur. J. Public Health 2021, 31, ckab164.786. [Google Scholar] [CrossRef]
- Buescher, A.V.; Cidav, Z.; Knapp, M.; Mandell, D.S. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatr. 2014, 168, 721–728. [Google Scholar] [CrossRef]
- Bieleninik, Ł.; Gold, C. Estimating components and costs of standard care for children with autism spectrum disorder in Europe from a large international sample. Brain Sci. 2021, 11, 340. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef] [PubMed]
- Aday, L.A. Evaluating the Healthcare System: Effectiveness, Efficiency, and Equity; Health Administration Press: Washington, DC, USA, 2004. [Google Scholar]
- Institute of Medicine (US); Committee on Health and Practice and Policy. Health and Behavior: The Interplay of Biological, Behavioral, and Societal Influences; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Minissi, M.E.; Landini, G.A.R.; Maddalon, L.; Torres, S.C.; Giglioli, I.A.C.; Sirera, M.; Abad, L.; Gómez-García, S.; Alcañiz, M. Virtual reality-based serious games to improve motor learning in children with autism spectrum disorder: An exploratory study. In Proceedings of the 2023 IEEE 11th International Conference on Serious Games and Applications for Health (SeGAH), Athens, Greece, 28–30 August 2023; IEEE: Piscataway, NJ, USA, 2023; pp. 1–6. [Google Scholar] [CrossRef]
- Tan, Q.P.; Huang, L.; Xu, D.; Cen, Y.; Cao, Q. Serious Game for VR Road Crossing in Special Needs Education. Electronics 2022, 11, 2568. [Google Scholar] [CrossRef]
- Alvarado, Y.; Guerrero, R.; Serón, F. Inclusive Learning through Immersive Virtual Reality and Semantic Embodied Conversational Agent: A case study in children with autism. J. Comput. Sci. Technol. 2023, 23, e09. [Google Scholar] [CrossRef]
- Parkinson, S.; Schumann, S.; Taylor, A.; Fenton, C.; Kearney, G.; Garside, M.; Johnston, D. SoundFields: A Virtual Reality Home-Based Intervention for Auditory Hypersensitivity Experienced by Autistic Children. Appl. Sci. 2023, 13, 6783. [Google Scholar] [CrossRef]
- Carneiro, T.; Carvalho, A.; Frota, S.; Filipe, M.G. Serious Games for Developing Social Skills in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review. Healthcare 2024, 12, 508. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, G.G.; Newbutt, N.N.; Lorenzo-Lledó, A.A. Designing virtual reality tools for students with Autism Spectrum Disorder: A systematic review. Educ. Inf. Technol. 2023, 28, 9557–9605. [Google Scholar] [CrossRef]
- Contreras-Ortiz, M.S.; Marrugo, P.P.; Cesar Rodríguez Ribón, J. E-Learning Ecosystems for People With Autism Spectrum Disorder: A Systematic Review. IEEE Access 2023, 11, 49819–49832. [Google Scholar] [CrossRef]
- De Carvalho, A.P.; Braz, C.S.; dos Santos, S.M.; Ferreira, R.A.; Prates, R.O. Serious Games for Children with Autism Spectrum Disorder: A Systematic Literature Review. Int. J. Human-Comput. Interact. 2023, 1–28. [Google Scholar] [CrossRef]
- Flay, B.R.; Biglan, A.; Boruch, R.F.; Castro, F.G.; Gottfredson, D.; Kellam, S.; Mościcki, E.K.; Schinke, S.; Valentine, J.C.; Ji, P. Standards of evidence: Criteria for efficacy, effectiveness and dissemination. Prev. Sci. 2005, 6, 151–175. [Google Scholar] [CrossRef]
- Kitchenham, B. Guidelines for performing systematic literature reviews in software engineering—Version 2.3. In Technical Report EBSE-2007-01; Keele University: Keele, UK, 2007. [Google Scholar]
- Systematic Literature Review—GitHub Repository. 2023. Available online: https://gitfront.io/r/UnivaqRepository/Ld1cG22q1AKd/SystematicReview/ (accessed on 2 April 2024).
- Lorenzo, G.; Lledó, A.; Arráez-Vera, G.; Lorenzo-Lledó, A. The application of immersive virtual reality for students with ASD: A review between 1990–2017. Educ. Inf. Technol. 2019, 24, 127–151. [Google Scholar] [CrossRef]
- Becker, K. What’s the difference between gamification, serious games, educational games, and game-based learning. Acad. Lett. 2021, 209. [Google Scholar] [CrossRef]
- Brereton, P.; Kitchenham, B.A.; Budgen, D.; Turner, M.; Khalil, M. Lessons from applying the systematic literature review process within the software engineering domain. J. Syst. Softw. 2007, 80, 571–583. [Google Scholar] [CrossRef]
- Gusenbauer, M.; Haddaway, N.R. Which academic search systems are suitable for systematic reviews or meta-analyses? Evaluating retrieval qualities of Google Scholar, PubMed, and 26 other resources. Res. Synth. Methods 2020, 11, 181–217. [Google Scholar] [CrossRef] [PubMed]
- Drubin, D.G.; Kellogg, D.R. English as the universal language of science: Opportunities and challenges. Mol. Biol. Cell 2012, 23, 1399. [Google Scholar] [CrossRef] [PubMed]
- Morrison, A.; Polisena, J.; Husereau, D.; Moulton, K.; Clark, M.; Fiander, M.; Mierzwinski-Urban, M.; Clifford, T.; Hutton, B.; Rabb, D. The effect of English-language restriction on systematic review-based meta-analyses: A systematic review of empirical studies. Int. J. Technol. Assess. Health Care 2012, 28, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Castañeda, V. Disadvantages in preparing and publishing scientific papers caused by the dominance of the English language in science: The case of Colombian researchers in biological sciences. PLoS ONE 2020, 15, e0238372. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Weighted kappa: Nominal scale agreement provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.R.; Vannest, K.J.; Fletcher, E. Encyclopedia of Special Education: A Reference for the Education of Children, Adolescents, and Adults with Disabilities and Other Exceptional Individuals; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Bozgeyikli, L.; Bozgeyikli, E.; Raij, A.; Alqasemi, R.; Katkoori, S.; Dubey, R. Vocational rehabilitation of individuals with autism spectrum disorder with virtual reality. ACM Trans. Access. Comput. 2017, 10, 5. [Google Scholar] [CrossRef]
- Simões, M.; Bernardes, M.; Barros, F.; Castelo-Branco, M. Virtual travel training for autism spectrum disorder: Proof-of-concept interventional study. JMIR Serious Games 2018, 6, e8428. [Google Scholar] [CrossRef]
- Naranjo, C.A.; Ortiz, J.S.; Álvarez, V.M.; Sánchez, J.S.; Tamayo, V.M.; Acosta, F.A.; Proaño, L.E.; Andaluz, V.H. Teaching process for children with autism in virtual reality environments. In Proceedings of the 9th International Conference on Education Technology and Computers, Barcelona, Spain, 20–22 December 2017; pp. 41–45. [Google Scholar] [CrossRef]
- Mora-Guiard, J.; Crowell, C.; Pares, N.; Heaton, P. Lands of fog: Helping children with autism in social interaction through a full-body interactive experience. In Proceedings of the 15th International Conference on Interaction Design and Children, Manchester, UK, 21–24 June 2016; pp. 262–274. [Google Scholar]
- Garzotto, F.; Gelsomini, M.; Occhiuto, D.; Matarazzo, V.; Messina, N. Wearable immersive virtual reality for children with disability: A case study. In Proceedings of the 16th International Conference on Interaction Design and Children, Stanford, CA, USA, 27–30 June 2017; pp. 478–483. [Google Scholar]
- Rojo, D.; Mayor, J.; Rueda, J.J.G.; Raya, L. A virtual reality training application for adults with Asperger’s syndrome. IEEE Comput. Graph. Appl. 2019, 39, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Thordarson, A.; Vilhjálmsson, H.H. SoCueVR: Virtual reality game for social cue detection training. In Proceedings of the ACM International Conference on Intelligent Virtual Agents, Paris, France, 2–5 July 2019; pp. 46–48. [Google Scholar]
- Takahashi, I.; Oki, M.; Bourreau, B.; Suzuki, K. Designing interactive visual supports for children with special needs in a school setting. In Proceedings of the International Conference on Designing Interactive Systems, Hong Kong, China, 9–13 June 2018; pp. 265–275. [Google Scholar]
- Herrero, J.F.; Lorenzo, G. An immersive virtual reality educational intervention on people with autism spectrum disorders (ASD) for the development of communication skills and problem solving. Educ. Inf. Technol. 2019, 25, 1689–1722. [Google Scholar] [CrossRef]
- Finkelstein, S.; Barnes, T.; Wartell, Z.; Suma, E.A. Evaluation of the exertion and motivation factors of a virtual reality exercise game for children with autism. In Proceedings of the 1st Workshop on Virtual and Augmented Assistive Technology (VAAT), Lake Buena Vista, FL, USA, 17 March 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 11–16. [Google Scholar]
- Lu, A.; Chan, S.; Cai, Y.; Huang, L.; Nay, Z.T.; Goei, S.L. Learning through VR gaming with virtual pink dolphins for children with ASD. Interact. Learn. Environ. 2018, 26, 718–729. [Google Scholar] [CrossRef]
- Elgarf, M.; Abdennadher, S.; Elshahawy, M. I-interact: A virtual reality serious game for eye contact improvement for children with social impairment. In Proceedings of the Joint International Conference on Serious Games, Valencia, Spain, 23–24 November 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 146–157. [Google Scholar]
- De Luca, R.; Naro, A.; Colucci, P.V.; Pranio, F.; Tardiolo, G.; Billeri, L.; Le Cause, M.; De Domenico, C.; Portaro, S.; Rao, G. Improvement of brain functional connectivity in autism spectrum disorder: An exploratory study on the potential use of virtual reality. J. Neural Transm. 2021, 128, 371–380. [Google Scholar] [CrossRef]
- Shahab, M.; Taheri, A.; Mokhtari, M.; Shariati, A.; Heidari, R.; Meghdari, A.; Alemi, M. Utilizing social virtual reality robot (V2R) for music education to children with high-functioning autism. Educ. Inf. Technol. 2021, 27, 819–843. [Google Scholar] [CrossRef]
- Rahmadiva, M.; Arifin, A.; Fatoni, M.H.; Baki, S.H.; Watanabe, T. A design of multipurpose virtual reality game for children with autism spectrum disorder. In Proceedings of the International Conference on Biomedical Instrumentation and Technology, Special Region of Yogyakarta, Indonesia, 23–24 October 2019; IEEE: Piscataway, NJ, USA, 2019; Volume 1, pp. 1–6. [Google Scholar]
- Alharbi, A.; Aloufi, S.; Assar, R.; Meccawy, M. Virtual reality street-crossing training for children with autism in Arabic language. In Proceedings of the International Conference on Innovation and Intelligence for Informatics, Computing and Technologies, Sakheer, Bahrain, 20–21 December 2020; pp. 1–6. [Google Scholar]
- Tsai, W.T.; Lee, I.J.; Chen, C.H. Inclusion of third-person perspective in CAVE-like immersive 3D virtual reality role-playing games for social reciprocity training of children with an autism spectrum disorder. Univers. Access Inf. Soc. 2020, 20, 375–389. [Google Scholar] [CrossRef]
- Winoto, P.; Xu, C.N.; Zhu, A.A. “Look to Remove”: A Virtual Reality Application on Word Learning for Chinese Children with Autism. In Proceedings of the International Conference on Universal Access in Human-Computer Interaction, Toronto, ON, Canada, 17–22 June 2016; Springer: Berlin/Heidelberg, Germany, 2016; pp. 257–264. [Google Scholar]
- Adjorlu, A.; Serafin, S. Head-mounted display-based virtual reality as a tool to teach money skills to adolescents diagnosed with autism spectrum disorder. In Interactivity, Game creation, Design, Learning, and Innovation; Springer: Berlin/Heidelberg, Germany, 2018; pp. 450–461. [Google Scholar]
- Vona, F.; Silleresi, S.; Beccaluva, E.; Garzotto, F. Social MatchUP: Collaborative games in wearable virtual reality for persons with neurodevelopmental disorders. In Proceedings of the Joint International Conference on Serious Games, Stoke-on-Trent, UK, 19–20 November 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 49–65. [Google Scholar]
- Nordahl-Hansen, A.; Dechsling, A.; Sütterlin, S.; Børtveit, L.; Zhang, D.; Øien, R.A.; Marschik, P.B. An overview of virtual reality interventions for two neurodevelopmental disorders: Intellectual disabilities and autism. In Proceedings of the International Conference on Human-Computer Interaction, Copenhagen, Denmark, 19–24 July 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 257–267. [Google Scholar]
- Parsons, S.; Cobb, S. Reflections on the role of the ‘users’: Challenges in a multi-disciplinary context of learner-centred design for children on the autism spectrum. Int. J. Res. Method Educ. 2014, 37, 421–441. [Google Scholar] [CrossRef]
- Pellicano, E.; Dinsmore, A.; Charman, T. What should autism research focus upon? Community views and priorities from the United Kingdom. Autism 2014, 18, 756–770. [Google Scholar] [CrossRef]
- Abascal, J.; Nicolle, C. Moving towards inclusive design guidelines for socially and ethically aware HCI. Interact. Comput. 2005, 17, 484–505. [Google Scholar] [CrossRef]
- Di Mascio, T.; Gennari, R.; Melonio, A.; Vittorini, P. The user classes building process in a TEL project. In Proceedings of the International Workshop on Evidence-Based Technology Enhanced Learning, Salamanca, Spain, 28–30 March 2012; Springer: Berlin/Heidelberg, Germany, 2012; pp. 107–114. [Google Scholar] [CrossRef]
- Bleumers, L.; All, A.; Marien, I.; Schurmans, D.; van Looy, J.; Jacobs, A.; Willaert, K.; de Grove, F. State of Play of Digital Games for Empowerment and Inclusion: A Review of the Literature and Empirical Cases; JRC Publications Repository: Luxembourg, 2013. [Google Scholar] [CrossRef]
- Lally, V.; Sharples, M.; Tracy, F.; Bertram, N.; Masters, S. Researching the ethical dimensions of mobile, ubiquitous and immersive technology enhanced learning (MUITEL): A thematic review and dialogue. Interact. Learn. Environ. 2012, 20, 217–238. [Google Scholar] [CrossRef]
- Brosnan, M.; Parsons, S.; Good, J.; Yuill, N. How can participatory design inform the design and development of innovative technologies for autistic communities? J. Assist. Technol. 2016, 10, 115–120. [Google Scholar] [CrossRef]
- Parsons, S. Authenticity in Virtual Reality for assessment and intervention in autism: A conceptual review. Educ. Res. Rev. 2016, 19, 138–157. [Google Scholar] [CrossRef]
- Seale, J.; Nind, M.; Parsons, S. Inclusive research in education: Contributions to method and debate. Int. J. Res. Method Educ. 2014, 37, 347–356. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- American Psychological Association. Template for Developing Guidelines: Interventions for Mental Disorders and Psychosocial Aspects of Physical Disorders; American Psychological Association: Washington, DC, USA, 1995. [Google Scholar]
- American Psychological Association. Criteria for evaluating treatment guidelines. Am. Psychol. 2002, 57, 1052–1059. [Google Scholar] [CrossRef]
- Hulley, S.B.; Cummings, S.R.; Newman, T.B.; Browner, W.; Grady, D. Designing Cross-Sectional and Cohort Studies; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; Volume 85. [Google Scholar]
- Patino, C.M.; Ferreira, J.C. Inclusion and exclusion criteria in research studies: Definitions and why they matter. J. Bras. Pneumol. Publicacao Soc. Bras. Pneumol. Tisilogia 2018, 44, 84. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn-Bennett, R.; Bowman, L.; Bulbulia, R. Post-trial follow-up methodology in large randomized controlled trials: A systematic review protocol. Syst. Rev. 2016, 5, 214. [Google Scholar] [CrossRef]
- Moher, D.; Schulz, K.F.; Altman, D.G.; Consort Group. The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomized trials. Lancet 2001, 357, 40–45. [Google Scholar] [CrossRef]
- Zweben, A.; Fucito, L.M.; O’Malley, S.S. Effective strategies for maintaining research participation in clinical trials. Drug Inf. J. 2009, 43, 459–467. [Google Scholar] [CrossRef]
- Keyworth, C.; Hart, J.; Armitage, C.J.; Tully, M.P. What maximizes the effectiveness and implementation of technology-based interventions to support healthcare professional practice? A systematic literature review. BMC Med. Inform. Decis. Mak. 2018, 18, 1–21. [Google Scholar] [CrossRef]
- Poston, J.M.; Hanson, W.E. Meta-analysis of psychological assessment as a therapeutic intervention. Psychol. Assess. 2010, 22, 203. [Google Scholar] [CrossRef]
- Sevinc, V.; Berkman, M.I. Psychometric evaluation of Simulator Sickness Questionnaire and its variants as a measure of cybersickness in consumer virtual environments. Appl. Ergon. 2020, 82, 102958. [Google Scholar] [CrossRef]
- Di Mascio, T.; Gennari, R.; Melonio, A.; Tarantino, L. Supporting children in mastering temporal relations of stories: The TERENCE learning approach. Int. J. Distance Educ. Technol. IJDET 2016, 14, 44–63. [Google Scholar] [CrossRef]
- Schmidt, M.; Newbutt, N.; Schmidt, C.; Glaser, N. A process-model for minimizing adverse effects when using head mounted display-based virtual reality for individuals with autism. Front. Virtual Real. 2021, 2, 611740. [Google Scholar] [CrossRef]
- Valencia, K.; Rusu, C.; Botella, F. A preliminary methodology to evaluate the user experience for people with autism spectrum disorder. In Proceedings of the 23rd International Conference on Human-Computer Interaction, Washington, DC, USA, 24–29 July 2021; Springer: Berlin/Heidelberg, Germany, 2021; pp. 538–547. [Google Scholar] [CrossRef]
- Simón-Vicente, L.; Rodríguez-Cano, S.; Delgado-Benito, V.; Ausín-Villaverde, V.; Delgado, E.C. Cybersickness. A systematic literature review of adverse effects related to virtual reality. Neurología 2022. [Google Scholar] [CrossRef]
- Oh, H.; Son, W. Cybersickness and its severity arising from virtual reality content: A comprehensive study. Sensors 2022, 22, 1314. [Google Scholar] [CrossRef]
- Ramaseri Chandra, A.N.; El Jamiy, F.; Reza, H. A systematic survey on cybersickness in virtual environments. Computers 2022, 11, 51. [Google Scholar] [CrossRef]
- Interaction Design Foundation-IxDF. What Is Cybersickness in Virtual Reality? 2024. Available online: https://www.interaction-design.org/literature/topics/cybersickness-in-virtual-reality (accessed on 2 April 2024).
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Muthuswamy, V. Ethical issues in clinical research. Perspect. Clin. Res. 2013, 4, 9–13. [Google Scholar] [CrossRef]
- Kass, N.E.; Hyder, A.A.; Ajuwon, A.; Appiah-Poku, J.; Barsdorf, N.; Elsayed, D.E.; Mokhachane, M.; Mupenda, B.; Ndebele, P.; Ndossi, G.; et al. The structure and function of research ethics committees in Africa: A case study. PLoS Med. 2007, 4, e3. [Google Scholar] [CrossRef]
- Lee, H.S. Ethical issues in clinical research and publication. Kosin Med. J. 2022, 37, 278–282. [Google Scholar] [CrossRef]
- Masic, I.; Hodzic, A.; Mulic, S. Ethics in medical research and publication. Int. J. Prev. Med. 2014, 5, 1073. [Google Scholar]
- Guraya, S.Y.; London, N.; Guraya, S.S. Ethics in medical research. J. Microsc. Ultrastruct. 2014, 2, 121–126. [Google Scholar] [CrossRef]
- ISO 9241-11:2018; Ergonomics of Human-System Interaction—Part 11: Usability: Definitions and Concepts. 2018. Available online: https://www.iso.org/standard/63500.html (accessed on 8 February 2024).
- Norman, D.A.; Draper, S.W. User Centered System Design: New Perspectives on Human-computer Interaction; L.; Erlbaum Associates: Mahwah, NJ, USA, 1986. [Google Scholar]
- Di Mascio, T.; Spagnoletti, P.; Tarantino, L.; Za, S. Successful UCD practices under IT project constraints. In Proceedings of the IADIS International Conference Information Systems 2012, IS 2012, Berlin, Germany, 10–12 March 2012; pp. 433–437. [Google Scholar]
- Di Mascio, T.; Gennari, R.; Tarantino, L.; Vittorini, P. Designing visualizations of temporal relations for children: Action research meets HCI. Multimed. Tools Appl. 2017, 76, 4855–4893. [Google Scholar] [CrossRef]
- Collins Dictionaries. Collins English Dictionary; HarperCollins: London, UK; Glasgow, Scotland, 1982. [Google Scholar]
- White, S.W.; Ollendick, T.; Albano, A.M.; Oswald, D.; Johnson, C.; Southam-Gerow, M.A.; Kim, I.; Scahill, L. Randomized controlled trial: Multimodal anxiety and social skill intervention for adolescents with autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 382–394. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The “Reading the Mind in the Eyes” Test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry Allied Discip. 2001, 42, 241–251. [Google Scholar] [CrossRef]
- Jolliffe, D.; Farrington, D.P. Development and validation of the Basic Empathy Scale. J. Adolesc. 2006, 29, 589–611. [Google Scholar] [CrossRef]
- Albiero, P.; Matricardi, G.; Speltri, D.; Toso, D. The assessment of empathy in adolescence: A contribution to the Italian validation of the “Basic Empathy Scale”. J. Adolesc. 2009, 32, 393–408. [Google Scholar] [CrossRef]
- Kamińska, D.; Zwoliński, G.; Laska-Leśniewicz, A. Usability Testing of Virtual Reality Applications—The Pilot Study. Sensors 2022, 22, 1342. [Google Scholar] [CrossRef]
- Dillenburger, K.; Röttgers, H.R.; Dounavi, K.; Sparkman, C.; Keenan, M.; Thyer, B.; Nikopoulos, C. Multidisciplinary teamwork in autism: Can one size fit all? Educ. Dev. Psychol. 2014, 31, 97–112. [Google Scholar] [CrossRef]
- Chong, S.O.K.; Pedron, S.; Abdelmalak, N.; Laxy, M.; Stephan, A.J. An umbrella review of effectiveness and efficacy trials for app-based health interventions. npj Digit. Med. 2023, 6, 233. [Google Scholar] [CrossRef]




| Autism Spectrum Disorder | Immersive Virtual Reality | Serious Game |
|---|---|---|
| Autism | Immersive Virtual Environment | Educational Game |
| ASD | HMD | |
| CAVE | ||
| Virtual Reality |
| IN1 | Research articles published between January 2009 and July 2021 |
| IN2 | Research articles written in English |
| IN3 | Research articles published in peer-reviewed journals or conference proceedings |
| IN4 | Research articles having the full text available (not only title and abstract) |
| IN5 | Research articles focusing on the rehabilitation of individuals with ASD |
| IN6 | Research articles dealing with IVR-based SG rehabilitative interventions |
| IN7 | Research articles reporting the evaluation of the proposed rehabilitative interventions |
| EX1 | Research articles published before 2009 |
| EX2 | Research articles that are not written in English (e.g., Chinese) |
| EX3 | Research articles of the following types: surveys, reviews, systematic reviews, meta-analyses, editorials, dissertations, theses, technical reports, student reports, posters, and unpublished works |
| EX4 | Research articles that have duplicates |
| EX5 | Research articles whose full text is not available nor obtained after a precise request to authors |
| EX6 | Research articles that do not deal with the topics of the systematic review (e.g., learning environment for nurses education) |
| EX7 | Research articles focusing on other health conditions (e.g., motor disabilities) or mental disorders (e.g., dementia) |
| EX8 | Research articles presenting interventions for ASD caregivers (e.g., parents and therapists) and not for individuals with ASD |
| EX9 | Research articles with a different purpose than rehabilitation (e.g., diagnosis) |
| EX10 | Research articles presenting interventions not implemented as SG |
| EX11 | Research articles presenting interventions not realised with IVR (e.g., robots) |
| EX12 | Research articles that do not report the evaluation of the proposed rehabilitative interventions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peretti, S.; Pino, M.C.; Caruso, F.; Di Mascio, T. Evaluating the Potential of Immersive Virtual Reality-Based Serious Games Interventions for Autism: A Pocket Guide Evaluation Framework. Educ. Sci. 2024, 14, 377. https://doi.org/10.3390/educsci14040377
Peretti S, Pino MC, Caruso F, Di Mascio T. Evaluating the Potential of Immersive Virtual Reality-Based Serious Games Interventions for Autism: A Pocket Guide Evaluation Framework. Education Sciences. 2024; 14(4):377. https://doi.org/10.3390/educsci14040377
Chicago/Turabian StylePeretti, Sara, Maria Chiara Pino, Federica Caruso, and Tania Di Mascio. 2024. "Evaluating the Potential of Immersive Virtual Reality-Based Serious Games Interventions for Autism: A Pocket Guide Evaluation Framework" Education Sciences 14, no. 4: 377. https://doi.org/10.3390/educsci14040377