1. Introduction
Childhood trauma has generated considerable concern in the related education of Early Childhood Education and Care (ECEC) domain, both in Ireland [
1,
2,
3] and, indeed, on a global scale [
4,
5]. According to Peterson [
6] (n.p.), trauma is any “
frightening, dangerous, or violent event that poses a threat to a child’s life or bodily integrity”. Researchers have reported that trauma can take on various forms encompassing, but not limited to, single-incident trauma, complex trauma, developmental trauma (including Adverse Childhood Experiences (ACEs)), intergenerational trauma, historical trauma, and vicarious trauma [
7,
8,
9]. Essentially, trauma exposure alerts the stress response system and induces the production of cortisol in the body [
10]. In childhood, if this physiological reaction is prolonged and occurs without the buffer of a responsive adult, the stress can become toxic and, in turn, can lead to broader biological and environmental factors [
11,
12,
13]. This is an established observation among children who experience Adverse Childhood Experiences (ACEs) [
14,
15,
16] and is often the factor most cited as a significant predictor of poor life-course trajectories [
17,
18,
19].
The literature pertaining to developmental trauma, and particularly ACEs, is continually expanding. The concept of ACEs originated from a groundbreaking public health study conducted in the United States by the Centre for Disease Control and Prevention (CDC), and the Kaiser Permanente’s Health Appraisal Clinic [
8]. Derived from a large epidemiological survey, the term ‘ACEs’ is widely utilised to describe traumatic experiences that occur before the age of 18, including sexual abuse, emotional abuse, physical neglect, emotional neglect, exposure to domestic violence, household substance abuse, household mental illness, incarcerated household member, parental separation, bereavement, or divorce. The ACE study found that more than half of respondents in a cohort of 17,337 reported at least one ACE, and one-quarter experienced ≥2 ACEs [
8]. The ACE study documented a graded relationship between the prevalence of early adversity and increased risk of negative outcomes throughout the lifespan including (i) substance misuse and addiction, (ii) mental illness, (iii) adolescent pregnancy and increased risk of sexually transmitted disease, (iv) poor educational performance and success, and (v) chronic pulmonary and respiratory disease [
8]. Subsequent research has reported a ‘dose–response’ relationship, deducing that as ACE scores increase, so too does the risk of poor health and wellbeing outcomes [
16,
20]. Moreover, numerous studies suggest that ACEs tend to cluster (multiple ACEs co-occurring) [
21,
22], and that exposure to four or more ACEs is regarded as a threshold for increased health-related complications across all diagnostic categories [
19,
23]. Evidentially, it is unsurprising that in 2018 the World Health Organisation (WHO) [
24] identified ACEs as a major public health concern affecting up to 250 million people each year.
While the groundbreaking findings of the ACEs study brought the concern of childhood trauma into the public sphere, notable limitations exist within the parameters and psychometric properties of the original study [
25,
26]. Despite admirations that the ACE study is “incredibly robust” [
27] (p. 30), Turner et al. [
26] highlight a structural flaw suggesting that the ACE study is narrow in scope and only considers ten possible adversities, whilst an array of other toxic environments also threaten children’s sense of safety. Notably, the ACE study model omits certain domains of systemic oppression, which have been subsequently expanded upon to represent the multifaceted and expansive nature of traumatic experiences [
24,
25]. Previously overlooked areas such as poverty, racism, homelessness, direct provision, life-threatening natural disaster, peer violence (bullying), witnessing community violence, witnessing collective violence (exposure to war), and acts or threat of terrorism now appear in the scientific literature as factors that can also contribute to trauma and adverse health outcomes [
28,
29].
In addition, the initial ACE study used a relatively homogeneous sample consisting of 70% Caucasian and 70% college-educated, middle-class citizens receiving healthcare services in San Diego [
27]. This indicates a lack of participant diversity and, further, limits the generalisability of the findings to other populations and/or stratified demographic and geographically dispersed cohorts. Further, the original ACE study is retrospective in nature, and is therefore limited by design in terms of potential recall bias [
30], whereby experiences contingent upon social inequalities, pre-study mental illness, teenage pregnancies, and parental country of origin make it difficult to determine cause and effect [
19,
31]. Finally, some concerns have been raised about the potential stigmatisation and labelling of individuals based on their ACE score [
32], which could have negative psychological reverberations.
1.1. Theoretical Framework and Literature Review
Trauma exposure is common in early childhood [
33,
34,
35] and can be a causation for a plethora of developmental complexities including emotional regulation [
36], memory capacities [
37], distressed behaviour [
38], and difficulty with logical reasoning [
39,
40]. Extant literature has established that Trauma-Informed Practice (TIP) and targeted training interventions can be leveraged to improve the aforementioned teaching and learning constraints caused by trauma exposure [
5,
41,
42].
1.2. Trauma-Informed Practice
In many cases, trauma can penetrate deep into the lives of individuals [
43], which can be supported through an evidence-based intervention, namely Trauma-Informed Practice (TIP) [
44,
45]. TIP is a strengths-based framework underpinned by six universal principles that relate to, and include, (i) safety, (ii) trustworthiness and transparency, (iii) peer support, (iv) collaboration and mutuality, (v) empowerment: voice and choice, and (vi) cultural, historical, and gender issues [
46]. Menschner and Maul [
47] assert that TIP comprises four main areas, which include recognising the impact of trauma and pathways for recovery, recognising the signs and symptoms of trauma, integrating trauma-informed policies and practices, and seeking to actively resist re-traumatisation.
Extant research demonstrates that children impacted by trauma require professional supports sensitive to their needs [
47,
48]. Although trauma-sensitive practice is a relatively new concept in ECEC settings [
49], there is ample evidence of international efforts to alter the educational milieu in the United States [
50,
51,
52,
53,
54], Canada [
55], Scotland [
56], Wales [
57], Australia [
58,
59], and South Africa [
60]. However, there is a paucity of research that has examined the facilitation of a context-specific trauma awareness training programme for the ECEC profession in Ireland.
1.3. Early Childhood Education and Care in Ireland: Contextual Understanding
The Early Childhood Education and Care (ECEC) profession, and, indeed, early learning and care systems across the world, have undergone a rapid transformation [
61]. Notably, the current study is situated within the context of the ECEC profession in Ireland. Evidence of organised preschool education in Ireland has dated back to the 19th century [
62], with the proliferation of this discourse evidenced through policy and framework developments [
63,
64,
65,
66] as well as sector-wide pay and condition advancements [
67]. According to the Annual Early Years Sector Service Report [
68], a total of 180,149 children are enrolled in at least one Government subsidy programme, demonstrating the high volume of children seeking early education and care nationwide. The provision of professional practice in ECEC is guided by the National Curriculum and Quality Frameworks, namely, Aistear [
64] and Siolta [
63]. While this is the case, the fact remains that there is no specific policy or training regulation that explicitly addresses trauma and Adverse Childhood Experiences for ECEC professionals in Ireland [
69], despite several Irish researchers advocating for the application of trauma-sensitive approaches in ECEC services [
1,
2,
70]. This concern is arguably compounded by the fact that trauma awareness education is not acknowledged as a core educational component in the Professional Award Criteria and Guidelines for Initial Professional Education in the ECEC profession in Ireland [
71]. As a critical context in which Trauma- Informed Practice (TIP) can be delivered, investigating the trauma-related knowledge, strategies, and training of ECEC professionals in Ireland is the overarching matter that the current study serves to address.
1.4. Relational Pedagogy
Trauma-sensitive approaches, essentially a relational regulatory approach [
72,
73], align well with ECEC guidelines for good practice as advocated by Ireland’s National Curriculum Framework, ‘Aistear’ [
64]. For example, building trusting and responsive relationships lie at the heart of ECEC practice [
64,
74], while these same values are a fundamental strand of trauma-sensitive environments [
75]. A similar thread of characteristics is present in the work of Page [
76] who conceptualises the reciprocal pedagogical relationship between the early educator and child as ‘Professional Love’, which is an attachment-based approach to cultivate positive interactions among early years discourse. Arguably, the five-step prospectus for developing professional love, which includes (i) thinking about professional love, (ii) de-centre, (ii) emotional literacy, (iv) reciprocal relationship, and (v) professional love, could reinforce and perpetuate the provision of trauma-sensitive ECEC environments. Further parallelisms can be drawn from Grimmer [
77], who advocates for a ‘Loving Pedagogy’ in the early years, a practice underpinned by relationships and attachment. In addition to conceptual considerations, researchers have emphasised the importance of both theoretical and practical knowledge for Early Childhood Education and Care (ECEC) professionals to effectively address childhood trauma in ECEC environments [
1,
2,
78]. The variables necessary for engaging in trauma discourse within ECEC include, but are not limited to, (i) theoretical understanding of children’s behaviour, (ii) use of trauma-sensitive language, (iii) implementation of neuro-informed practices, (iv) familiarity with polyvagal theory, attunement, and co-regulation, (v) evidence of the key person approach, and (vi) facilitation of supported transitions. Integrating the conceptual, theoretical, and practical aspects of ‘current pedagogical literature’ and ‘trauma-sensitive practice’ could establish a unified framework for supporting children impacted by trauma.
To date, there have been numerous studies that theorise trauma as a primary driver of negative outcomes across children’s behaviour [
60], educational skills [
79], and practitioner wellbeing [
5,
55,
80]. However, there is little evidence to suggest that any trauma-related curriculum is offered to Irish ECEC students during Initial Practitioner Education (IPE) and/or to ECEC professionals via Continuous Professional Development (CPD) opportunities [
81]. Anecdotal evidence suggests that in an Irish context, the current provision of trauma education for ECEC professionals fails to adequately address this discourse, necessitating a more thorough investigation of this matter [
81]. While addressing trauma education for ECEC professionals is well documented across international literature, e.g., [
5,
42,
55], there has been comparatively little research to rigorously quantify the provision of same in an Irish context. In the current study, such a quantification is provided by data obtained through a comprehensive online survey instrument.
The primary aim of the current study was to explore the presence, if any, and prevalence, of trauma-related knowledge, strategies, and training of ECEC professionals in Ireland. The secondary aim was to examine the uptake of said offerings, and, indeed, the impact of same on subsequent professional practice.
3. Results
The first domain of the survey instrument, ‘General Information’, incorporated 10 areas of inquiry, namely, (i) Gender, (ii) Age, (iii) Role, (iv) Years of Experience, (v) Setting Type, (vi) Age-group of children, (vii) Available Schemes, (viii) Services Provided, (ix) Curricular Approach, and (x) Experience.
Table 1 presents the demographic characteristics of the participants. Within the study sample, 97.9% (
n = 1025) identified as female, 1.8% (
n = 19) identified as male, 0.2% (
n = 2) identified as nonbinary, and 0.2% (
n = 2) preferred not to say. Other participant characteristics revealed that the most frequent response across the age, setting type, and role-based questions were (i) 26–45 years, (ii) working in a private setting, and (iii) working in a managerial-based role.
To illustrate ECEC professionals’ experience of working with childhood trauma in Ireland, participants were asked whether they had experience of working with children from diverse family circumstances (
Table 2).
Findings revealed that the most prevalent social context and family characteristics that participants work with are children from a one-parent family (89.6%, n = 857). Across all 13 variables, the largest response with a range ≥ 80% was experience of working with children from ‘one-parent families’, ‘low-income families’, ‘families with English as an Additional Language (EAL)’, and/or children with a ‘diagnosed disability or additional need’. Notwithstanding the lower percentage of ECEC professionals found working with children living in foster care, direct provision, homeless services, or who lost a parent to deportation, within the constraints of the current study parameters, future research could interrogate perspectives related to bias, discrimination, and diversity.
3.1. Trauma-Related Knowledge
Results pertaining to trauma-related knowledge, strategies, and training were inter-related, with latent factors emerging across these respective areas of investigation. The results obtained from Domain Two of the survey instrument, which explored the domains of prior education, trauma awareness, Initial Practitioner Education (IPE), and Continuous Professional Development (CPD), revealed an interconnected relationship between these factors. With regard to the participants’ highest level of education in the field of ECEC, results ranged across all education levels on the National Framework for Qualification (NFQ) (
Table 3).
Domain Three of the survey instrument, ‘Personal Experience’, contained both theoretical and practical-based questions. When participants were asked if during their employment, they had ever attended to a child who experienced trauma or adversity, 59.3% (
n = 480) answered ‘Yes’, 27.6% (
n = 223) answered ‘No’, while 13.1% (
n = 106) answered ‘Unsure’. In a follow-up question, participants were asked if they had experience of working with children from an 18-item list, with a 6-point Likert type ranging from ‘Unsure’ to ‘Very Often’. Responses in the ‘Never’ and ‘Rarely’ category were grouped and recoded as a new classification: ‘Did Not Experience’, while responses in the ‘Often’ and ‘Very-Often’ category followed the same process and were recoded into the ‘Experienced Frequently’ classification.
Table 4 illustrates the ‘Yes’ responses of attending to children who experienced trauma with the 18-item list of adverse events.
Further interrogation of the initial (i) ‘Yes/No’ responses of attending to children experiencing trauma, with (ii) working with children who have experienced specific events, revealed that out of the 223 participants who initially answered ‘No’ to the former, 59% had selected at least one variable across the 18 trauma-related items, while 22% answered ‘Unsure’ to one or more variables on the itemed list. The highest response was among the ‘Parental Separation, Divorce, or Bereavement’ category, with 52% of the initial ‘No’ response subsequently claiming to work with children within this ecological circumstance (
Figure 2).
Participants were subsequently asked in the ‘Personal Experience’ domain about the areas of child development that they feel are impacted by trauma. Across a 10-item developmental list, the ‘Impacted’ category was heavily weighted with responses > 85% for each developmental classification, with the highest response rate of 97.1% accounting for ‘Distressing Behaviour’. Results related to the ‘Not Impacted’ category indicate that ‘Physical Development’ is the highest variable not impacted by trauma (6.1%) (
Table 5).
Participants were also asked if they had experienced children impacted by trauma presenting with diverse symptoms across a 20-item list with a 6-point Likert type ranging from ‘Unsure’ to ‘Very Often’. Responses in the ‘Never’ and ‘Rarely’ category were grouped and recoded as a new classification: ‘Did Not Experience’, responses in the ‘Sometimes’, ‘Often’, and ‘Very Often’ category followed the same process and were recoded into the ‘Experienced’ classification, and the ‘Unsure’ responses were classified as such (
Table 6). The 20-item list was informed by extant trauma theory [
86,
87,
88] and expert knowledge [
8,
89] on the adverse effects of childhood trauma. The results highlight that >50% of participants experienced children impacted by trauma-related behaviours across 18 of the 20 variables presented in the question.
The overall self-perceived trauma-related knowledge of the participants was assessed using a numeric slider scale. Participants were asked to rate their current knowledge in addressing the complexity of childhood trauma on a scale of 1 to 10, with 10 representing the highest level of knowledge. The participants’ self-reported results yielded a mean score of 5.05 ± 2.1, with a range of 10.
3.2. Trauma-Based Strategies
Domain Four of the survey instrument, ‘Service Policy and Procedures’, was designed to explore the practical modalities of how ECEC professionals in Ireland respond to children experiencing trauma. Twelve expansive trauma-based strategies were measured using a Likert type question, which illustrated that the ‘Very Often’ category presented with the highest frequency of responses across 10 of the 12 strategies (
Table 7).
Findings indicate that in the ‘Often’ and ‘Very Often’ combined sub-domain, there is a response rate >75% across nine of the 12 variables. In total, there are only two strategies that do not have the highest response rate in the ‘Very Often’ category: trauma-sensitive/non-triggering language and understanding trauma-response behaviour. Additionally, 26.2 (n = 173) of participants reported that their service had a policy in place designed to support children experiencing trauma, a larger 49.2% (n = 325) of settings did not, while 24.7% (n = 163) were unsure. There was no statistically significant relationship found between the existence of a trauma-focused policy and the setting type (i.e., private or community) (p = 0.654).
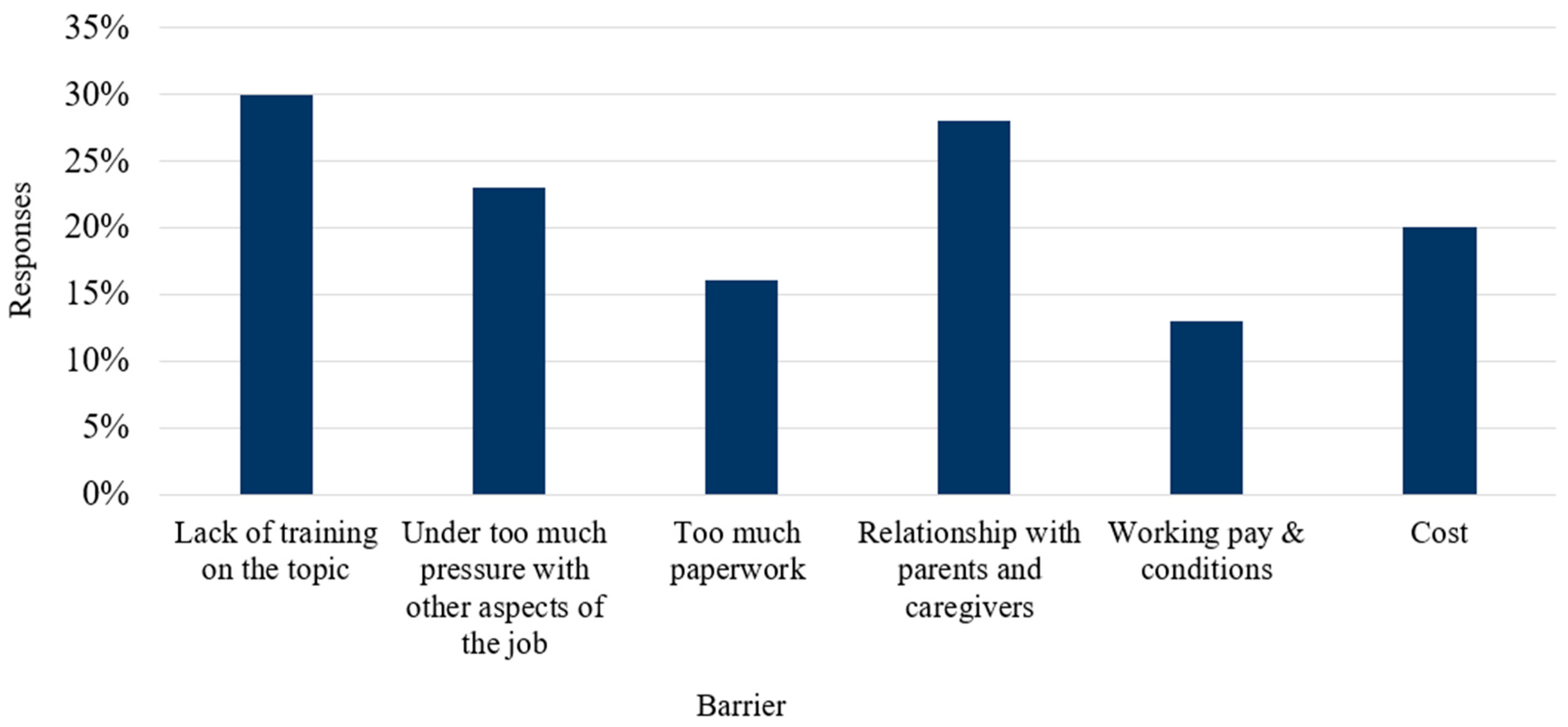
Data pertaining to organisational barriers to implementing trauma-sensitive practice was also obtained. Results revealed that 31.9% (
n = 197) of participants agreed that they are presented with barriers to trauma-sensitive practice, 32.7% (
n = 202) answered ‘Sometimes’, 19.8% (
n = 122) answered ‘Unsure’, while 15.6% (
n = 96) reported ‘No’ existing barriers. To elicit a more detailed account of potential barriers, display logic conditions were applied to the ‘Yes’ and ‘Sometimes’ response categories, with the respective data presented in
Figure 3.
3.3. Trauma-Related Training and Education
3.3.1. Initial Practitioner Education (IPE)
The exploration of trauma-related education and training for ECEC professionals included both Initial Professional Education (IPE) and Continuous Professional Development (CPD). To evaluate trauma education during IPE, a 12-item (i.e., specific educational constructs), topic-oriented question was utilised. This comprehensive question measured the extent of educational attainment across the inter-related domains of psychology, neuroscience, and holistic wellbeing, with a response scale ranging from ‘None’ to ‘Very In-Depth’. The prevalence of trauma education for participants during IPE ranged from 3.8% to 30.3% (
Table 8).
Further analysis of the data revealed that the largest proportion of responses in the ‘None’ category (i.e., those who received no formal education in respective educational constructs) were trauma-sensitive approaches, trauma-sensitive language, polyvagal theory, and trauma-informed practice, with a range of responses from 31.9 to 58.7%. The highest volume of responses was observed in the ‘Some, but Not Much’ category, which accounted for 8 of the 12 educational constructs. Across all 12 constructs, the ‘Very In-Depth’ category yielded the lowest proportional response with a range from 1.4 to 13.4%. Neither the ‘Quite In-Depth’ nor the ‘Very In-Depth’ constructs marked any of the highest responses for the level of training received.
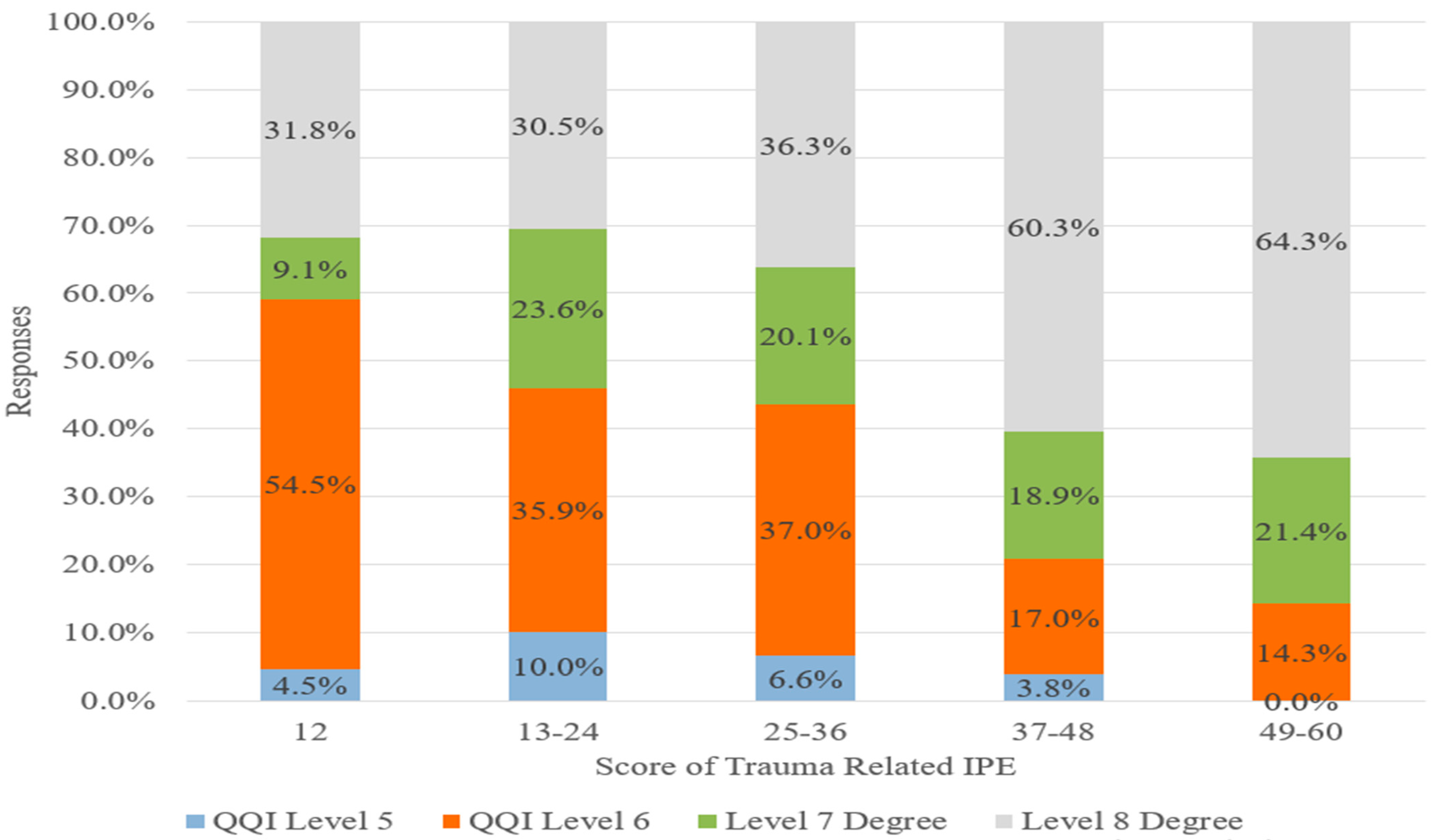
Across the 12 educational constructs, an aggregate score was generated to assess the relationship (if any) of trauma education during IPE with participants’ highest level of education. The IPE-related question utilised a 5-point Likert type response and assigned numerical codes to each response category (i.e., None = 1; Very Little = 2; Some, but Not Much = 3; Quite In-Depth = 4; Very In-Depth = 5), which were summed across the 12 areas of study for each participant. Potential scores ranged from 12 to 60, which were then recoded into five distinct numerical classifications (i.e., 12, 13–24; 25–36; 37–48; 49–60). The classifications were purposefully chosen to ensure (i) an equal distribution of scoring ranges per classification (i.e., 12), and (ii) a single numerical score that captured data relating to the ‘no education’ responses across all educational constructs (i.e., a score of 12). The results revealed a statistically significant association between participant level of educational attainment and total IPE score (
p = 0.000), with a downward linear pattern evident, indicating that those with a lower level of educational attainment generally scored lower across the 12 educational constructs (
Figure 4). A further analysis was conducted to examine trends between ‘College of Further Education’ Awards (i.e., Level 5 and 6 Awards collapsed together) and ‘University’ Awards (i.e., Level 7 and 8 Awards collapsed together). An unequivocal trend emerged, whereby there was a linear increase in the prevalence of those participants with University Awards scoring consistently higher across the 5 response rate options (i.e., ‘None’ to ‘Very In-Depth)—Category 1: ‘None’ (59.1% QQI Level 5 and 6 vs. 40.9% Level 7 and 8 Degree); Category 2: ‘Some’ (45.9% QQI Level 5 and 6 vs. 54.1% Level 7 and 8 Degree); Category 3: ‘Some, but Not Much (43.6% QQI Level 5 and 6 vs. 56.4% Level 7 and 8 Degree); Category 4: ‘Quite In-Depth’ (20.8% QQI Level 5 and 6 vs. 79.2% Level 7 and 8 Degree); and Category 5: ‘Very In-Depth’ (14.3% QQI Level 5 and 6 vs. 85.7% Level 7 and 8 Degree). The two highest numerical classification categories (i.e., Category 4: 37–48 and Category 5: 49–60) also contained the highest proportion of Level 8 Degree holders, almost double that of Categories 1 and 2, and 40% greater than Level 8 Degree holders in Category 3. Inversely, the lowest numerical category revealed that 31.8% of participants possess a Level 8 Degree, and a further 9.1% hold a Level 7 Degree, which illustrates that the remaining 59.1% cumulative score in this classification (i.e., a score of 12) relates to participants with either a QQI Level 5 or 6 Award. This numerical category also identified that there were more participants with a Level 8 Degree that reported receiving no education than participants with a Level 7 or QQI Level 5 Award. Within the highest numerical category, only 5.9% (
n = 42) of participants who answered the question summed a score in this classification (i.e., 49–60).
To assess the extent to which Ireland’s National Curriculum Framework—Aistear [
64] and the National Quality Framework—Síolta [
63] supported participants in understanding the importance of fostering and maintaining key relationships in an ECEC context, participants were asked to respond to a 5-point Likert type question. The scale ranged from ‘Quite well’ to ‘Not well at all’, and out of the 703 responses received, 24%, (
n = 254) of participants reported feeling prepared ‘Quite well’ by Aistear [
64] and Síolta [
63]. Only 2% (
n = 20) of participants answered ‘Not well at all’. Additionally, 15.3% (
n = 161) of participants expressed feeling ‘Somewhat’ prepared by Aistear [
63] and Síolta [
80] to maintain key relationships in ECEC settings. There was no statistically significant association between participants’ level of education and the extent to which Aistear [
63] and Síolta [
80] helped in their understanding of key relationships (
p = 0.176).
3.3.2. Continuous Professional Development (CPD)
In the Continuous Professional Development (CPD) domain of the survey instrument, 45.4% (
n = 319) of participants reported engaging in a trauma-related CPD programmes during their career. The highest response rate (38.7%,
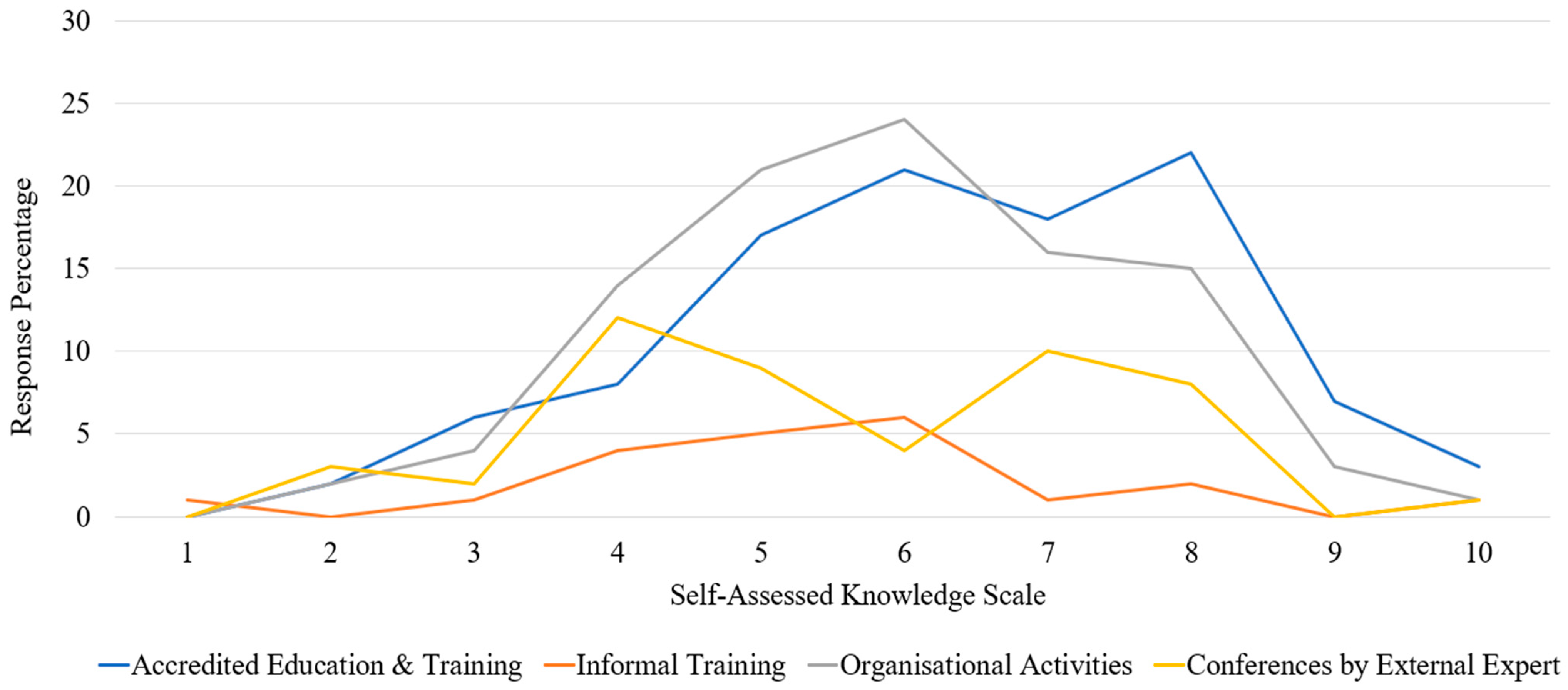
n = 120) for the type of CPD obtained was among the ‘Accredited Education and Training’ (short courses, and/or formal on-the-job training). In addition to being asked to state the CPD style, participants were also provided with a slider scale to rate their current trauma knowledge on a numerical scale from 1–10, with 10 representing the best score.
Figure 5 illustrates the participants’ self-assessed perceptions against these two axes.
Out of the 383 respondents (54.6%) who did not attend trauma-focused CPD only, 83.2% (n = 317) reported being interested in receiving targeted CPD training. In line with their current knowledge, participants were asked whether they thought a tailored training programme focusing on how to support children impacted by trauma would be beneficial, with 95.5% (n = 588) answering ‘Yes’. Of these responses, 31.9% (n = 187) recommended that this training should be during Initial Practitioner Education (IPE), while 60% (n = 352) favoured CPD style training outside of formal education settings. Over 40% of participants (42.1%, n = 256) stated that this training should be delivered via a blended format (i.e., onsite and online), with 50.9% (n = 309) believing that the duration of this programme should be a training module over a 6-month period. Data indicated that a ‘One day’ duration is favoured by 16.5% (n = 100) of participants (onsite, n = 37; online, n =33; blended, n = 30), while 10.7% (n = 65) would like this training over ‘One week’ (onsite, n = 27; online, n = 19; blended, n = 19).
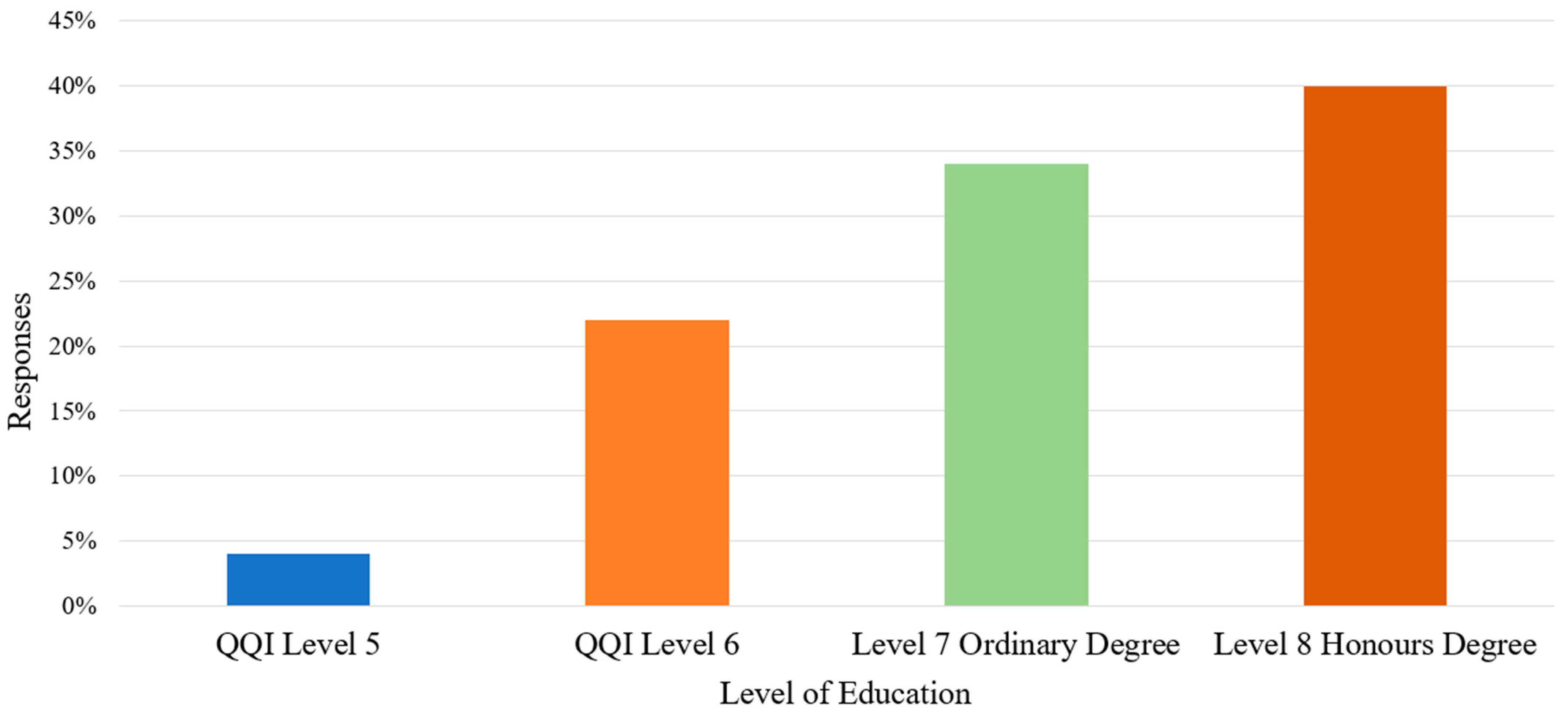
3.4. The Role of Formal Education
Data revealed a linear progression of CPD completion from QQI Level 5 to Level 8 Honours Degree, with the percentage of participants completing trauma-based CPD rising for each cohort on the National Framework of Qualifications (NFQ). A chi-square test for association revealed that participants with a higher level of education (i.e., QQI Level 5–Level 8 Degree) were found to have statistically engaged more with trauma-focused CPD (
p = 0.039) (
Figure 6).
4. Discussion
This study sought to examine the trauma awareness knowledge, strategies, and training in Ireland’s Early Childhood Education and Care (ECEC) profession. The findings across these inter-related domains have generated novel quantitative data concerning trauma education among the ECEC profession in Ireland.
4.1. Trauma-Related Knowledge
Initially, participants were requested to confirm if they had ever worked with children who had experienced trauma or ACEs. A subsequent question with an extensive list of 18 traumatic events was then presented to participants to ascertain which experience(s) (if any) they had experience of working with among children in their care. In the first instance, 59% of participants (
n = 480:
n = 259 in private settings;
n = 207 in public settings) stated that they have experience of working with childhood trauma. This demographic characteristic is interesting as it exposes not only the existence of childhood trauma in private ECEC settings in Ireland, but also the concerning prevalence of same. Although there is widespread agreement among researchers that vulnerable and marginalised communities are at a higher risk of experiencing trauma [
29,
90], including members of the travelling community [
91,
92], members of the homeless community [
93], children in poverty [
94], children impacted by migration [
95], and children in direct provision/refugees [
96,
97], trauma is also exhibited by children attending private settings, which challenges the preconception that trauma only exists within the parameters of marginalised and disadvantaged communities. Within the acknowledgement of the Early Childhood Care and Education scheme, which is a free preschool year available to all children in Ireland, of those who answered ‘Yes’ to working with childhood trauma, they performed their daily roles in a facility that offered multiple additional services (i.e., part time day-care service (37.3%), after-school club (34.0%), full day-care service (32.5%), breakfast club (24.0%), drop-in centre (1.0%)). Arguably, working with children outside the scope of the ECCE scheme could increase the likelihood of ECEC professionals encountering childhood trauma in private settings. Although social class seldom features in data pertaining to trauma exposure [
98], which makes it difficult to disentangle the cause and effect of class stratification and traumatic experiences, previous literature has conceptualised this discourse as ‘affluent neglect’ [
99,
100]. Notably, there was no statistically significant relationship between the dichotomous variables (i.e., Yes/No experience of trauma and Private/Community setting type) (
p = 0.729), which underscores the widespread occurrence of childhood trauma in ECEC environments in Ireland regardless of setting type.
Knowledge-based results (i.e., understanding of trauma) revealed that out of the initial ‘No’ responses (n = 223) of encountering childhood trauma at work (i.e., in ECEC settings), 59% of participants subsequently declared working (to some degree) with children who have experienced trauma and early adversity in Irish ECEC services. This discrepancy indicates that there is a lack of trauma awareness among ECEC professionals, and further, a fundamental misunderstanding as to what constitutes trauma, which is concerning. It is worth noting that while 59% (n = 480) of participants answered ‘Yes’ and explicitly reported working with childhood trauma, there is reasonable evidence to suggest that this figure could be much higher. Given both the direct and indirect examples of working with children with trauma histories, it is likely that >75% (n = 611) of respondents are currently working with, or have worked with, children exposed to some classification of trauma. In addition, 13% (n = 106) of participants were ‘Unsure’ if they had worked with children from the 18-item list, further highlighting participants’ uncertainty as to the composition of trauma. Hence, it is unsurprising that a high volume of participants expressed their desire for increased trauma awareness training (n = 588).
Knowledge related to the barriers of implementing a trauma-sensitive approach in ECEC settings constituted a breadth of educational-, practical-, and regulatory-based challenges at both local and national level. Results revealed that 30% of participants (
n = 316) who answered the respective question believe that a ‘lack of training on the topic’ hinders the achievement of trauma-sensitive ECEC environments, which corresponds with extant research of low trauma education during both Initial Practitioner Education (IPE) [
52] and Continuous Professional Development (CPD) [
5,
101]. Additionally, findings pertaining to parental-based barriers demonstrated that 16% of participants (
n = 168) expressed how a lack of communication with parents and caregivers is a notable challenge, while 12.4% (
n = 131) attribute a difficulty in building relationships with parents and caregivers to the same trajectory. It emerges, then, that ‘partnerships with primary caregivers’ should feature as a core component of trauma-related training; further, efforts to provide ECEC professionals with the requisite skills of effective partnership should be evident among IPE and CPD provisions. Whitaker et al. [
80] evaluated the Enhancing Trauma Awareness (ETA) Course among 96 preschool teachers in the United States and reported a positive impact on the quality of teacher-parent relationships as a consequence of a culmination of increased trust, greater empathy, and mindfulness of parent histories post intervention. Due to the unique position of ECEC professionals in supporting children and families impacted by trauma [
50,
51,
102], it is critical that those working in the profession are adequately trained to understand the intricacies of intergenerational trauma and how effective partnerships are situated within a trauma-sensitive context.
4.2. Trauma-Related Strategies
The literature in the broad field of education has called attention to the role of relationship-building strategies in trauma-informed frameworks [
103,
104], particularly in an ECEC context [
34,
105,
106]. A latent factor that emerged from the ‘Strategies’ component of Domain Four of the survey instrument (i.e., Service Policy and Procedures) illustrated that the ‘Never’ and ‘Rarely’ response categories accounted for 12.7% (
n = 78) for the 3R’s Model, 5.9% (
n = 36) for Co-regulation, and 4.5% (
n = 28) for Unconditional Positive Regard. Although these figures are not exceedingly high, this finding is particularly worrying, given that researchers have collaboratively emphasised the relational nature of trauma-informed practice [
103,
104,
107]. Therefore, it is concerning that any percentage of Irish ECEC professionals would report to ‘Never’ or ‘Rarely’ engage in these relationship-based approaches. Scholarly consensus affirms that responsive and nurturing relationships are the primary means of achieving healing and recovery from trauma [
108,
109,
110]. On a practical level, relationship-building techniques have been linked with practices that foster compassion, kind listening, and unconditional positive regard; all processes that have been benchmarked to naturally curtail re-traumatisation [
49,
111]. It gives rise to concern that the kernel of trauma healing does not feature in the practice of some ECEC professionals in Ireland, substantiating the need for reform in this component of IPE and CPD education, to support both ECEC professionals and the children in their care.
Interestingly, a qualitative study conducted by Brunzell and colleagues [
59], that evaluated the Trauma-Informed Positive Education (TIPE) training programme with primary and secondary school teachers in Australia (
N = 18), reported an increased awareness of unconditional positive regard and co-regulation strategies in attending to students’ needs in a responsive and relational manner. Although data were obtained in a primary school environment, the fact remains that trauma-based training can positively inform pedagogical practice to align with strategies that promote healing and recovery [
112,
113]. Furthermore, in an ECEC context, there are numerous examples of increased utilisation of relationship-based approaches as a direct result of trauma-informed training [
4,
34,
42,
101]. Commonalities can be drawn from several studies that examined the effectiveness of trauma-based training interventions, namely, the statistically significant increase in ECEC professionals (i) confidence in providing supportive relationships (
p = 0.01) [
101], (ii) use of relationship-building strategies (
p < 0.001) [
4], and (iii) confidence in providing trauma-informed strategies and providing supportive relationships (
p = 0.01) [
42]. It could be argued that in order to ameliorate the current shortfall of trauma-sensitive strategies demonstrated in Ireland (refer to
Table 6), IPE and CPD provision should establish a connection between the intrinsically relational aspect of (i) the ECEC professional role, (ii) trauma-sensitive practice, and (iii) Ireland’s National Curriculum Framework for Early Childhood–Aistear [
64], as a mandatory component of ECEC curriculum. Arguably, in Ireland, there is significant scope to (re)align Aistear’s core position of key relationships in conjunction with trauma-sensitive approaches to illustrate a greater degree of the conceptual and practical commonalities between ‘extant trauma literature’ and ‘national policy’.
4.3. Trauma-Related Training
The integration of two key components of professional training, namely, IPE and CPD, served as a central focus of the current study. By examining the provision of trauma awareness training within the framework of both educational pathways, the study examined a range of interconnected yet distinct findings.
4.3.1. Initial Practitioner Education (IPE)
Evidence pertaining to existing trauma education among ECEC professionals presented as low across the (i) type, (ii) depth, and (iii) level of training received (if any). The main tenets of trauma theory are central to ECEC programmes [
114], yet the data from the current study points to a dearth of trauma education experienced by the participants. The inquiry into participants’ exposure to the 12 trauma-related educational constructs during IPE revealed that a lack of trauma awareness is prevalent among ECEC professionals in Ireland, which was hypothesised based on previous research that identified a scarcity of trauma theory in IPE programmes globally [
52,
59,
81]. This was substantiated in the current study, with a mere 5.9% (
n = 42) of participants achieving scores in the highest numerical category of the 12 item IPE question (i.e., 49–60), which reflects the concerningly low proportion of ECEC professionals in Ireland receiving adequate trauma education. Additional findings revealed a trend across the numerical categories in that out of those with a higher aggregate score, there was a higher prevalence of Level 7 and 8 Degree respondents per category, evidencing the progressive trajectory of trauma education among undergraduate learning pathways (i.e., from QQI Level 5 to Level 8 Degree). Similarly, related findings indicated that those with a higher level of educational attainment also demonstrated significantly more engagement with trauma-based CPD (
p = 0.039).
In essence, ECEC professionals in Ireland with lower educational attainment display (i) lower baseline education in trauma awareness (e.g., IPE) and (ii) lower trauma-related CPD endeavours. However, a latent factor that emerged from the data revealed that out of those who reported having received no training across any of the 12 educational constructs, 31.8% possessed a Level 8 Degree. However, upon further analysis of the cohort size presenting in this numerical category, this percentage score relates to only 7 participants, which reflects 1% of the total cohort that answered this question in full. Nonetheless, of the participants who reported receiving no trauma education during IPE, it potentially draws attention to the absence of core teaching and learning constructs of trauma awareness in some IPE programmes in Ireland. Butler et al. [
1] highlight the key components associated with a trauma-sensitive approach in ECEC, which coincide with many of the educational constructs outlined in the 12-item IPE question, including (i) Attachment, (ii) Relationship-Based Approaches (i.e., Attunement, Compassion, and the Key Person Approach), (iii) Neuro-informed, (v) Co-regulation, (vi) Wellbeing, and (vii) Polyvagal Theory. It could be argued that if the trauma-related IPE knowledge required to cultivate a trauma-sensitive environment is not offered to, and obtained by, prospective ECEC practitioners, irrespective of the educational level on the NFQ, the practices integral to the provision of same will remain insufficiently addressed in ECEC discourse.
A further compounding factor is that if there is no culture of trauma education among lower levels of education on the NFQ, QQI Level 5 and Level 6 programmes are not only at risk of inadequate trauma education provision, but respective cohorts could be categorised as a ‘hard-to-reach’ population in advancing the provision of trauma awareness within the profession. Given that 65% of those working in the ECEC profession in Ireland possess a QQI Level 5 or 6 Award as their highest qualification [
68], it is problematic and highly concerning if prospective students on these programmes are systematically diverted from opportunities to advance their trauma-related knowledge and skills. Therefore, to address this critically important finding form the current research, efforts must be made by Further Education and Training (FET) Institutes, related CPD organisations, and/or ECEC representative bodies to establish/prioritise trauma education at these specific educational levels (i.e., QQI Level 5 and 6). This could apportion trauma-based offerings across all ECEC professionals and potentially counter the existing imbalance of qualification-based trauma education exposure. If efforts to reform this fragmented training structure are not acted upon by the aforementioned institutes and organisations, it could jeopardise ECEC professionals’ knowledge and confidence to effectively attend to children with trauma histories, both now and in the future.
An additional IPE-related concern emerged in the current study with regard to the role of Aistear [
64] in preparing ECEC professionals for engaging in key relationships in professional practice. Findings suggest that participants’ level of education did not statistically relate with how well Aistear [
64] and Síolta [
63] assisted in the understanding of key relationships (
p = 0.176). Surprisingly, participants possessing a Level 8 Honours Degree qualification did not have an increased understanding of Aistear’s advocacy for building and maintaining relationships than lower qualification grades, which is a point of concern. Arguably, there is a need for trauma-related IPE to (re)focus on the relational components of Aistear [
64] and Siolta [
63] to (i) harmonise the commonalities of both frameworks with trauma-sensitive principles, and (ii) ensure that ECEC-based trauma awareness training is contextually appropriate and situated within the parameters of the National Curriculum and Quality Framework for Early Childhood in Ireland. If the amalgamation of trauma theory and national policy could render greater trauma-related outputs, it seems, then, that IPE content should integrate provisions to reflect this discourse. By the same logic, extending this knowledge to CPD programmes would yield promising outcomes for ECEC professionals working in the profession post-qualification.
4.3.2. Continuous Professional Development (CPD)
Various types of CPD styles may provide an indication of the level and depth of training received; therefore, it was hypothesised that participants who attended training that is longer in duration, and more formally accredited, would rate themselves higher on the numeric scale of trauma knowledge. Data pertaining to the ‘Accredited Education and Training’ CPD style revealed a mean score of 6.3. Interestingly, the data supported the aforementioned hypothesis that those with more formal training self-reported higher rates of trauma knowledge. However, there is a ubiquitous trend among the Domain Two ‘Training and Education’, as well as the Domain Three ‘Personal Experience’, datasets, which indicates a poverty of trauma awareness with regard to (i) what experiences constitute trauma, (ii) the implementation of trauma-sensitive strategies, and (iii) the establishment of a trauma-focused policy or targeted intervention for children experiencing trauma. These findings highlight the lack of practical application of CPD-acquired knowledge within ECEC environments, at least to some degree, and the existing disconnect between theory and practice. This could be due, in part, to the absence of context-specific ECEC-based content within current trauma awareness training, which Nicholson et al. [
83] highlight as a necessity for the ECEC profession. Consequently, it is unsurprising that >95% of participants (
n = 588) advocated for a bespoke trauma awareness training intervention, with anecdotal research suggesting that this trajectory is currently unaddressed, and indeed under-researched, in the Irish ECEC sphere [
81].
4.4. The Role of Formal Education
Findings related to the role of formal education bisected both IPE and CPD educational pathways. Interestingly, results from the current study indicated that participants with a higher level of IPE education statistically engaged more with trauma-related CPD (
p < 0.05). Contrastingly, in a study linking trauma training content to trauma-informed attitudes and stress in preschool teachers and staff, Loomis and Felt [
5] found that out of 111 preschool teachers in the USA, participants with a higher-education degree revealed no statistically significant relationship in receiving trauma-informed training. This demonstrates that although there may be no differentiation or graded levels of trauma education across various CPD interventions in the USA, the theoretical structure of CPD engagement on the NFQ in Ireland appears to integrate a progressive model of trauma education from QQI Level 5 to Level 8 Degrees. However, despite the demonstrated relationship between higher qualification levels and CPD engagement,
Figure 5 denotes that on a scale of 1 to 10 of trauma-related knowledge (10 being the best), data revealed a mean score of 6.3 ± 3.7. While it can be considered a positive that participants who engaged in CPD rated themselves an average of 6/10, there is ample scope to advance this trajectory to a higher figure with a narrower distribution spread. Furthermore, within the IPE domain,
Table 6 depicts that current training across the 12 educational constructs lacks depth. Arguably, this may compromise the adequacy, and indeed prosperity, of ECEC-student training, highlighting the capacity to progress the highest response rate from the ‘Some but Not Much’ to the ‘Quite In-Depth—Very In-Depth’ category.
4.5. Limitations
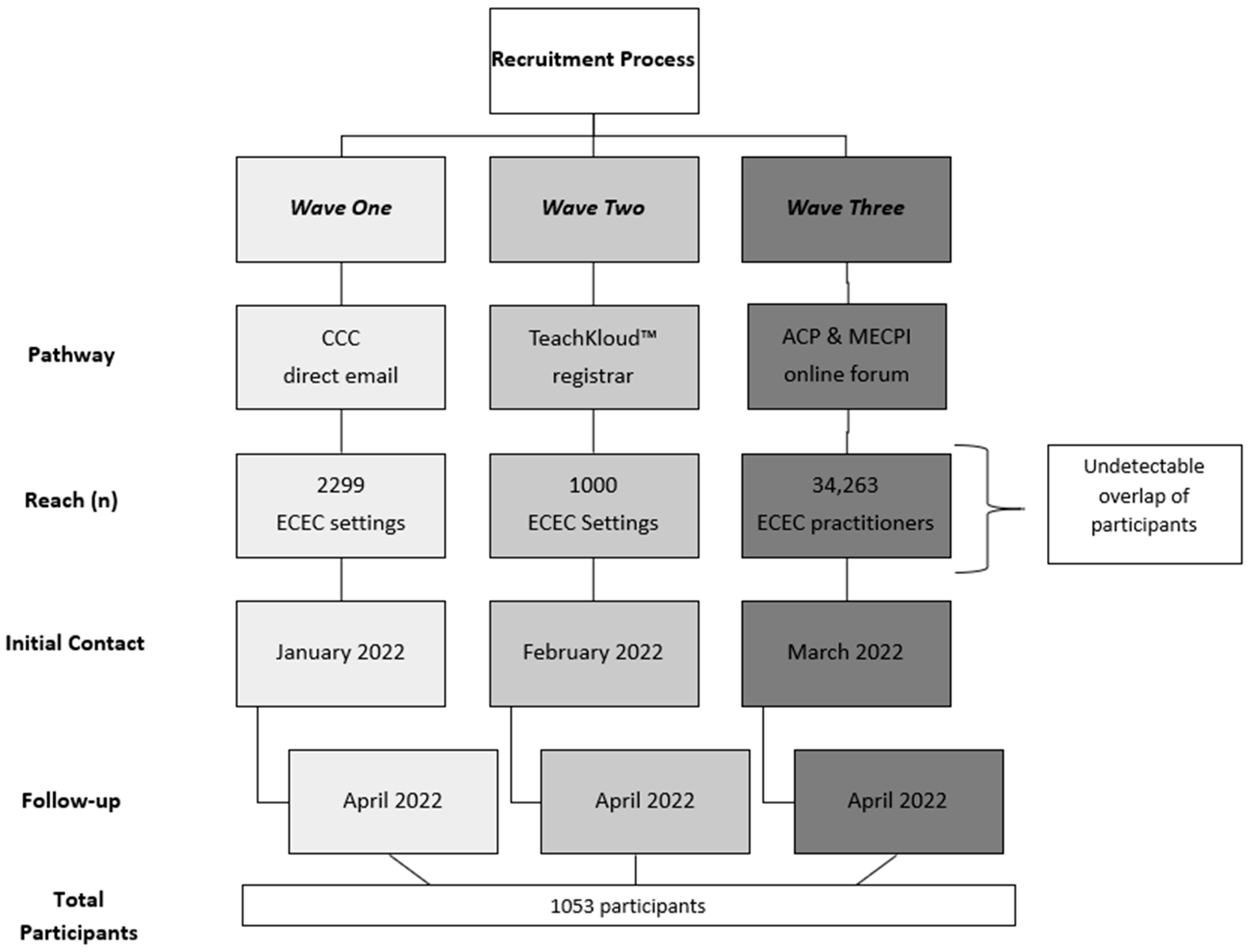
There are several limitations associated with the current study. With regard to the recruitment pathway, given that there was no universal database for those working in the ECEC profession in Ireland at the time of the research design process, a tripartite approach of carefully considered routes (i.e., CCC, TeachKloud™, ACP/MECPI) was selected to maximise participation rates nationwide. Further, the intricate dissemination process that incorporated both direct emails to ECEC settings (via the CCC and TeachKloud™) and the online forum exposure (ACP and MECPI) makes it impossible to calculate the extent of potential participant overlap in receipt of the survey instrument, thereby rendering the response rate indeterminable. While the initial hyperlink was accessed by 1373 participants, the precise range of survey instrument distribution is numerically unknown. A further limitation relates to the linear decline in response rates as the survey instrument progressed from Domain 1 to 5, which evidences the survey fatigue that occurred. However, survey fatigue is a phenomenon documented as an accepted norm in related research methodology [
115]. Finally, this study has produced novel data regarding trauma education associated with the ECEC profession in Ireland, and, further, is pioneering in its findings related to the wider context of childhood trauma and ACEs in ECEC environments in Ireland.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}