Abstract
Youth Mental Health First Aid (YMHFA) is a widely adopted professional development tool that helps educators across the United States improve their mental health literacy. Data from a pretest/posttest evaluation of the YMHFA training delivered at five schools are used to explore whether various YMHFA outcomes differ for teachers who have and have not received previous mental health training. Specifically, the current study compares scores on confidence, knowledge, negative attitudes, and intentions to intervene prior to completing the YMHFA program (i.e., at baseline), the rate of change in each measure, and satisfaction with the training across teachers with and without previous mental health prevention training. Our findings showed that teachers with previous training scored higher on confidence, mental health knowledge, and intentions to intervene at baseline and experienced different patterns of change after completion of the YMHFA training program, compared to teachers without prior training. Negative attitudes and training satisfaction did not reveal differences across training experiences. Study findings offer important program and policy implications about teachers’ training experiences, as well as the value of implementing YMHFA as a universal training in educational settings.
1. Introduction
Over the last two decades, mental health challenges among children and adolescents have escalated, as several studies have identified rising rates of psychological distress, mental health diagnoses, and suicide risk (Bommersbach et al., 2023; Gili et al., 2019). These trends indicate growing public health concern, as more youth struggle with conditions that impact their educational outcomes, developmental trajectory, and overall quality of life, especially post COVID-19 (Piao et al., 2022). In response, federal and state initiatives to support the coordination, integration, and delivery of mental health programs and services within educational systems are currently underway around the United States. Examples of these efforts include Project AWARE (Advancing Wellness and Resilience in Education, Substance Abuse and Mental Health Services Administration), Every Student Succeeds Act (ESSA, U.S. Department of Education), and the Students, Teachers, and Officers Preventing (STOP) School Violence Grant Program (Bureau of Justice Assistance). These efforts aim to promote healthy development in schools and other youth-focused systems. An important component of these initiatives is strengthening the ability of professionals (such as teachers and other school staff) to support young people’s mental health needs.
One ongoing approach to building this capacity among teachers is through delivering professional development programs, such as Youth Mental Health First Aid (YMHFA), to all school staff. YMHFA is designed to equip professionals with the skills to recognize and respond to mental health challenges experienced by youth. Prior studies that have evaluated the effectiveness of YMHFA have generally found improvements in participants’ knowledge, attitudes, and confidence regarding youth mental health issues (Aakre et al., 2016; Noltemeyer et al., 2020). However, less is known about whether training effectiveness varies across individual or work-related factors. This raises questions about the need to “scale up” YMHFA within schools and/or school districts, making it a universal or mandatory training for all teachers, or whether schools’ available resources for professional development (e.g., teachers’ time out of the classroom, substitute teachers’ pay to cover the classroom, and YMHFA instructor and curriculum fees) would be better utilized through a tiered implementation system based on identifiable individual or work-related characteristics, such as prior training experiences.
The purpose of the current study is to explore the relationship between prior mental health training and YMHFA effectiveness/satisfaction among teachers. Using data from a pretest/posttest evaluation of the YMHFA training in five schools from a southeastern school district in the United States, three objectives guide the current study: (1) examine differences in training outcomes (i.e., confidence, knowledge, negative attitudes, help seeking intentions) between teachers that did and did not report completing mental health training sometime before participating in YMHFA, (2) assess how these dimensions change following YMHFA training based on prior mental health training experience, and (3) explore whether satisfaction with YMHFA training varies between teachers with and without prior mental health training.
1.1. Youth Mental Health First Aid Training
Mental Health First Aid (MHFA) was originally developed in Australia to address voids in first aid courses that typically ignored mental health problems and crises (Kitchener & Jorm, 2004). Through an 8-hour training program, one fundamental objective of MHFA is to educate participants on the common signs and risk factors linked to mental health challenges in adults, along with encouraging the use of evidence-based mental health services and other appropriate support systems. Central to the training is a five-step action plan known as ALGEE (Assess for risk of suicide or harm, Listen non-judgmentally, Give reassurance and information, Encourage appropriate professional help, and Encourage self-help and other support strategies). ALGEE is used to assist individuals during encounters with adults who are experiencing a mental health crisis or exhibiting signs of mental or emotional distress (Kitchener & Jorm, 2002). In the United States, MHFA has been recognized by both federal and state agencies as a universal, evidence-based training for helping professionals (Hadlaczky et al., 2014; Sagar & Pattanayak, 2016) responsible for recognizing mental health needs and facilitating connections to appropriate support services (Isaac et al., 2009).
Introduced in 2012 in the United States, a revised version of MHFA was designed to educate adults on supporting youth who encounter mental health difficulties (Jorm et al., 2010). The same objectives and five-step action plan from MHFA are utilized in Youth Mental Health First Aid (YMHFA), although the strategies are contextualized to address the needs of youth (ages 10 to 18) instead of adults. The curriculum covers fundamental topics, including the prevalence of mental health disorders in children and adolescents, warning signs and symptoms, and the connection between trauma and adolescent development, suicide prevention and intervention, and strategies for de-escalation. Over the last decade, YMHFA has gained substantial recognition and has been widely adopted (Ng et al., 2021; Sánchez et al., 2021). Since its inception, over 1.8 million individuals have been trained in YMHFA in the United States (Mental Health First Aid, n.d.).
Studies of the effectiveness of YMHFA have found the training program to be promising in improving the skills needed to work with at-risk youth and those with current mental health needs (Haggerty et al., 2019; Noltemeyer et al., 2020; Sánchez et al., 2021). These findings are especially true regarding increases in key YMHFA constructs such as confidence (Elligson et al., 2021; Haggerty et al., 2019; Soderstrom et al., 2024), knowledge (Marsico et al., 2022; Noltemeyer et al., 2020), attitudes (Gryglewicz et al., 2018; Jorm et al., 2010), help-seeking intentions (Kelly et al., 2011; Rose et al., 2019), and preparedness (Childs et al., 2020). These training outcomes highlight the potential value in building mental health competencies among trainees. However, prior YMHFA research has not fully addressed possible group differences in training outcomes. Personal characteristics of training participants are important aspects that can shape an individual’s knowledge, belief systems, and confidence in their ability to effectively intervene with youth (Burnette et al., 2015). For example, some recent studies have found differences in training outcomes across participants’ demographic characteristics, such as race/ethnicity and sex (Gryglewicz et al., 2018; Soderstrom et al., 2024), and work-related characteristics such as educational attainment, experience, and employment sector (Childs et al., 2020; Haggerty et al., 2019). Although these findings have not been consistent across outcomes or samples, these results indicate a need to account for both demographic and work-related characteristics when assessing the YMHFA training. Understanding if and how trainee characteristics may moderate the relationship between pre- and post-training mental health literacy and satisfaction with YMHFA is important in maximizing the training’s impact.
1.2. Prior Mental Health Training and YMHFA Outcomes
The personal characteristics of training participants are important aspects that can shape their knowledge, belief systems, and confidence in their ability to intervene with youth effectively (Burnette et al., 2015), which are key YMHFA training outcomes. One work-related aspect that warrants closer attention is prior mental health training, which may impact how teachers engage with and benefit from participating in YMHFA. Some studies have included prior mental health training experiences as a control variable in their analyses (see Elligson et al., 2021; Geierstanger et al., 2024; Brady & Childs, 2023), which offers preliminary insights into its potential influence on training outcomes.
Of these studies, and although mental health training experiences were not the primary focus, the findings are mixed. Central to our current investigation was one of the primary findings from Gryglewicz et al. (2018), who examined the effectiveness of the YMHFA training in a sample of educators (teachers, administrators, and school staff). At the bivariate level, educators without prior mental health and/or substance use training reported greater levels of improvement on the domains of mental health knowledge, confidence, and intentions to engage in help-seeking behaviors. These findings continued to emerge even in multivariate analyses, when controlling for various demographic and other work-related factors. Based on the results discussed above, we expand on Gryglewicz et al. (2018) by utilizing a sample of only teachers, focusing specifically on the role of prior mental health prevention training, utilizing a repeated measures analytic technique, and examining mean differences in YMHFA outcomes across prior mental health training experiences.
Relatedly, other research has shown that participants without prior mental health training showed large gains in certain areas, such as increased confidence following YMHFA (Geierstanger et al., 2024). In contrast, participants with prior mental health or suicide prevention training entered YMHFA training with higher baseline scores on knowledge, confidence, and intentions to intervene, making prior training history the most consistent predictor of mental health literacy before YMHFA (Elligson et al., 2021). These participants did not show improvement in their knowledge of mental health post-training, but this finding is not surprising given their higher pre-training scores. Other studies have found no significant impact of prior training on YMHFA outcomes, including among key constructs such as confidence, help-seeking intentions to intervene, preparedness, and knowledge (Childs et al., 2020; Soderstrom et al., 2024). These mixed findings indicate a need to continue to explore the role of prior training on YMHFA constructs, before and after completion of the training.
1.3. Rationale for the Current Study
Over the last decade, YMHFA has been rapidly adopted across the United States and has garnered widespread support from both federal and state policymakers. Despite the widespread implementation of this program (Ng et al., 2021; Sánchez et al., 2021), less is known about specific trainee characteristics, particularly prior mental health training, that may help explain differences in YMHFA outcomes. This gap is especially relevant for teachers, who have daily interaction with students. The ability to recognize early signs and respond to students’ mental health needs not only improves overall student outcomes but also results in a more inclusive and supportive school environment that promotes student well-being and academic success (see Adelman & Taylor, 2009, 2012; Atkins et al., 2010). Given the central role that teachers play in supporting students, it is important to clarify how prior mental health training experiences influence YMHFA outcomes.
For instance, teachers who demonstrate above-average proficiency in key areas, such as mental health knowledge or help-seeking intentions, before undergoing YMHFA training may not be the most suitable candidates for such programs. Specifically, allocating resources to teachers who are already well-equipped to address youth mental health needs could lead to inefficient uses of training resources and teachers’ time. Teachers do not have unlimited opportunities for professional development, and schools do not have unlimited resources for mental health prevention training. Therefore, ensuring that teachers attend the appropriate training programs that meet their educational and professional skill level is essential. Additionally, failing to account for teachers’ pre-training proficiencies may lead to an underestimation of the training’s actual impact. As the goal of training programs is to enact change in its participants, teachers who score high on pretest measures do not have much room (if any) to improve. What results in this situation is a ceiling effect, where teachers with prior training produce low rates of change from pretest to posttest. This is not because the training was ineffective, but because there was no room for improvement due to high baseline scores.
The current study builds upon prior research in two important ways. First, this study directly examines YMHFA outcomes and satisfaction among a sample of teachers. Existing YMHFA studies, to date, tended to include broader samples of school personnel (e.g., combined samples of teachers, administrators, and other school staff) and/or social service professionals outside of the educational setting (see Childs et al., 2020; Gryglewicz et al., 2018). Second, while most prior evaluations of YMHFA relied on bivariate assessments of change (e.g., Aakre et al., 2016; Noltemeyer et al., 2020), our study examines change across multiple YMHFA outcomes while accounting for the impact of some individual and work-related covariates. As such, the findings from the current study have important implications for future research expanding on existing YMHFA studies, guiding decisions on professional development requirements for teachers, and tailoring YMHFA implementation strategies to maximize training effectiveness and resource allocations. Three research questions guide the current study: (1) Do teachers with and without prior mental health training differ across key YMHFA constructs (confidence, knowledge, negative attitudes, and help-seeking intentions) prior to YMHFA training?, (2) After completion of YMHFA, how do changes in these constructs differ between teachers with and without prior mental health training?, and (3) Does satisfaction with the YMHFA training differ between teachers with and without prior mental health training?
2. Methods
2.1. Data and Sample
Data for the current study were based on a larger school-based research initiative, funded by the National Institute of Justice, that sought to improve school climate and safety (see Childs et al., 2019). The overall initiative was a comprehensive mental health program that addressed the emotional and behavioral needs of high-risk students through practitioner training (e.g., professional development), needs assessment, student-focused emotional regulation instruction, and connections to community-based services. The program was implemented in five public schools from one school district. The schools participating in the initiative were chosen by the school board based on the prevalence of student and family challenges both within the school environment (identified by high discipline and low school attendance rates) and in the broader community (characterized as having high poverty and crime rates). At the time of implementation, the five schools served over 4000 primary and secondary students.
Study data included information collected from teachers who participated in a school-wide implementation of the YMHFA training. The original sample included 333 teachers, although seven respondents did not provide information about prior mental health training experiences. The final sample includes 326 teachers. Table 1 presents the coding and distribution of the sample characteristics across the entire sample. Sixty-five percent (n = 212) of the sample of teachers reported no prior mental health training, and 35% (n = 114) reported participating in a previous mental health or suicide prevention program. Approximately 84% of the sample were female, 72% were White, and 39% had a graduate degree. Forty-one percent of the sample had 10 years or less experience working with youth/students, while 51% reported talking to students about mental health problems at least once in the past 30 days.

Table 1.
Sample description for the full sample and broken down by prior training group.
2.2. Study Design and Procedure
YMHFA was facilitated by the school district social workers who had undergone YMHFA training through the National Council for Mental Wellbeing (NCWB). The training was conducted across two 4-hour sessions or in one 8-hour day at different points throughout the academic year and depending on school schedules. Each session accommodated a maximum of 30 participants, with the average class size ranging between 15 and 20 adults. Trainers adhered to the NCWB curriculum guidelines, as specified in the instructor manuals. The training covered fundamental topics, which included an overview of prevalent mental health difficulties in children and adolescents, such as behavioral disorders, mood disorders, anxiety disorders, eating disorders, and substance use disorders. Additionally, the training described prevalence rates, warning signs and symptoms, and risk factors to be aware of. Other key areas of instruction included general adolescent development, trauma, psychosis, suicide prevention and intervention, and strategies for de-escalation. Relatedly, all participants engaged in group-based activities to learn and apply the five-step ALGEE action plan.
Before participating in the training, teachers provided consent to take part in the evaluation of the YMHFA training, which was one component of the larger school-based research initiative. On the day of the training, teachers completed a pretest survey before the training began. Following the training session(s) on the same day, teachers were immediately asked to complete a posttest survey. Each survey took approximately 15 min to complete. All study protocols received approval from the university’s institutional review board.
2.3. Independent Variables
Various individual and work-related factors that could potentially influence mental health literacy and satisfaction with the training were included. Prior mental health training was identified by asking teachers if they have ever participated in training covering youth mental health and/or suicide prevention training. Those who responded that they had either or both types of training were categorized as having prior mental health training (coded as 1), compared to teachers who reported not having these types of previous training experiences (coded as 0). Demographic characteristics included a teacher’s sex (1 = male, 2 = female) and race/ethnicity (0 = Non-White, 1 = White). The Non-White category included Black, Other Race, and Hispanic participants. Educational attainment (graduate degree) was measured by asking teachers to report their highest degree or level of school completed, coded to differentiate between those who had a Bachelor’s degree or less (coded as 0) compared to those with a graduate degree (coded as 1). The number of years that teachers worked with students was also included (years worked with students), which was an ordinal measure differentiating between less than one year (coded as 1) to over twenty years (coded as 7). Teachers were also asked about past experiences speaking with students about mental health in the past 30 days (frequency of mental health interactions), coded ordinally as 0 = never, 1 = once, 2 = sometimes, 3 = frequently/often.
2.4. Dependent Variables
Four YMHFA constructs that represent different dimensions of mental health literacy (see Jorm, 2000; Kutcher et al., 2015, 2016) were measured: confidence, knowledge, negative attitudes, and help-seeking intentions to intervene. Confidence is the ability to identify mental health conditions and respond to mental health needs. Confidence or perceived behavioral control (PBC) was assessed using a 12-item Likert scale (α = 0.94), with the items adapted from Gryglewicz et al. (2015). Teachers rated their confidence in performing specific behaviors on a scale from 1 (“strongly disagree”) to 5 (“strongly agree”). Example items included statements about the ability to identify mental health symptoms, determine appropriate responses when interacting with a student experiencing a mental health issue, and the ability to find resources that could help a youth experiencing a mental health problem. The average of the items was used to generate an overall confidence score that ranged from 1 to 5 (representing the scale of the observed items). Higher scores indicated greater confidence (or PBC) in being able to assess the severity of a mental health problem and ability to find resources.
To assess knowledge of the ability to identify mental health conditions, teachers answered “true” or “false” to eight statements adapted from Davidson (2016). Some example items include “An individual with bipolar disorder is sometimes unpredictable because their mood fluctuates between depression and mania”, “When someone has a mental illness, their brain is impaired in a way that affects their behavior and emotions”, and “One of the main causes of mental illness is a lack of control and discipline.” The responses were recategorized as “correct” (=1) or “incorrect” (=0) and then summed to reflect the number of accurately answered items (range = 0 to 8 items answered correctly). Higher scores represented greater mental health knowledge.
Negative attitudes toward mental illness and working with students with mental health problems were assessed with an 11-item Likert scale, which ranged from 1 (“strongly disagree”) to 5 (“strongly agree”). Six items were adapted from the personal stigma subscale from the Depression Stigma Scale (Griffiths et al., 2004) and were slightly re-worded to focus on the target population (students) and mental health issues more broadly. Example items included statements such as “Mental health is a sign of personal weakness” and “Students who have mental health problems are unpredictable.” The other five items focused on teachers’ personal attitudes toward mental health services and the perceived role of helping professionals, such as “Mental health services should only be used if nothing else works” and “Asking about suicide should only be done by trained professionals.” A total negative attitudes score was created by taking the average across the observed items (ranging from 1 to 5, α = 0.75), with higher scores representing more negative attitudes toward mental illness and greater reluctance toward working with youth experiencing mental health challenges.
Intentions to intervene relate to teachers’ willingness to intervene in help-seeking behavior and were operationalized through a 10-item Likert scale that ranged from 1 (“not very likely) to 3 (“very likely”). Adapted from Jorm et al. (2005, 2010), teachers were initially presented with a scenario depicting a youth experiencing mental health difficulties and were then asked to indicate the likelihood that they would engage in various help-seeking behaviors (e.g., encouraging the use of professional help services, finding resources, calling a suicide prevention hotline, etc.) The average of the 10 items was used (range 1–5, α = 0.80). Higher scores indicated greater intentions to intervene in helpful behaviors.
Satisfaction with the training was included in the posttest evaluation to examine the utility, engagement, and expectations through 6 items (α = 0.73) in a Likert scale format (1 = “strongly disagree” to 5 = “strongly agree”). Teachers responded to questions evaluating whether the YMHFA training aligned with their expectations and the extent to which its content could be applied to their professional responsibilities. For example, teachers were asked if the training was culturally sensitive, if they were comfortable, felt that it was engaging, and met learning expectations. The average of the six items was used to represent training satisfaction, which ranged from 1 to 5. Higher scores represented greater satisfaction with the training.
2.5. Analytic Procedure
The analyses followed the three research questions. To answer the first research question (i.e., compare pretest/baseline scores across teachers who did and did not report prior mental health training), independent sample t-tests were first conducted. Four separate independent sample t-tests were performed to examine differences in confidence, knowledge, negative attitudes, and intentions to intervene prior to delivery of the training. Cohen’s d was also calculated to identify the strength/magnitude of the mean differences (MD) between the prior mental health training groups. Next, for constructs that demonstrated statistically significant mean differences in pretest scores across mental health training groups, ordinary least square (OLS) regression models were estimated to understand if prior mental health training predicted teachers’ reported confidence, knowledge, negative attitudes, and help-seeking intentions at baseline, after accounting for demographic factors and work-related characteristics.
To answer the second research question (i.e., compare changes over time in average scores of the mental health literacy constructs across groups of teachers on whether they reported prior mental health training), a repeated measures analysis of variance (RM-ANOVA) was conducted for each training outcome. This analytical approach requires dependent variables to be measured at a minimum of two time points, with the independent variable conceptualized as a latent factor representing “time”. Each time point functions as a distinct level or grouping within this independent variable. In the current study, four outcome variables (i.e., confidence, knowledge, negative attitudes, and intentions to intervene) were assessed across two time points (pretest and posttest). We first considered the main within-subjects effects as an initial assessment of whether meaningful change from pretest to posttest occurred among the full sample (i.e., regardless of previous training experience). Then, we examined between-subjects effects, which estimated the interaction between “time” and prior mental health training. For within- and between-subjects effects, meaningful changes over time were determined by the F-statistic (p < 0.05) and partial eta2 (i.e., effect size, ηp2). Sphericity was evaluated using Mauchly’s test. When the assumption was violated (p < 0.05), Greenhouse–Geisser corrections were applied to adjust the degrees of freedom. We also calculated post-hoc estimates using the Bonferroni method for pairwise comparisons to identify mean differences (MD) from pretest to posttest across training groups. To answer the third research question (i.e., examine whether satisfaction with the YMHFA training differed across teachers’ prior training history), an independent samples t-test was conducted to examine differences in satisfaction with the training at posttest (after delivery of the training) across teachers who did and did not report prior mental health training.
3. Results
3.1. Research Question 1: Differences in Baseline Scores Across Prior Training Groups
The first research question addressed whether teachers with and without prior mental health training differed across dimensions of mental health literacy. Table 2 reports the results of four independent samples t-tests, one test each for confidence, mental health knowledge, negative attitudes, and help-seeking intentions. Results indicate that confidence and mental health knowledge showed statistically significant differences across prior training groups (p < 0.05). On average, participants who reported prior mental health training reported higher scores in confidence to engage in help-seeking behavior and knowledge to identify mental health conditions. No statistically significant differences in negative attitudes or help-seeking intentions were found across training groups.
Table 2.
Independent samples t-test of baseline scores and prior training experiences.
The three separate OLS regression models for confidence, mental health knowledge, and intentions to intervene are reported in Table 3. OLS regression results predicting baseline scores for negative attitudes are not reported because no bivariate differences across training groups were observed in the prior analyses (Allison, 1999). However, although intentions to intervene did not attain the standard p < 0.05 threshold, we report the OLS results for this domain because the two-tailed p-value was exactly at the threshold cutoff (i.e., p = 0.05), the one-tailed t-test met the p < 0.05 threshold (p = 0.03), and Cohen’s d was over 0.20. These bivariate results demonstrate small to modest mean differences in help-seeking intentions across prior training groups.
Table 3.
Ordinary least squares regression predicting baseline (pretest) score for each domain.
Prior mental health training was a statistically significant predictor of baseline scores across all three models. After controlling for relevant individual and work-related characteristics, teachers’ who reported prior mental health training were higher at baseline on confidence (b = 0.74, SE = 0.10, p < 0.001), mental health knowledge (b = 0.73, SE = 0.22, p < 0.01), and intentions to intervene (b = 0.10, SE = 0.05, p < 0.05). The only other covariate to show a meaningful pattern across all three domains was a teacher’s sex. Females were more likely to have higher pretest scores for mental health knowledge (b = 0.91, SE = 0.29, p < 0.01) and intentions to intervene (b = 0.18, SE = 0.07, p < 0.01) compared to their male counterparts.
3.2. Research Question 2: Differences in YMHFA Effectiveness Across Prior Training Groups
The second research question examined whether changes in the four training outcomes differed between teachers with and without mental health training. To answer the second research question, four separate RM-ANOVAs were performed. Each model included individual (e.g., White, female) and work-related (graduate degree, years worked with students, frequency of interactions about students’ mental health) characteristics as covariates, and prior mental health training was the between-subjects contrast.
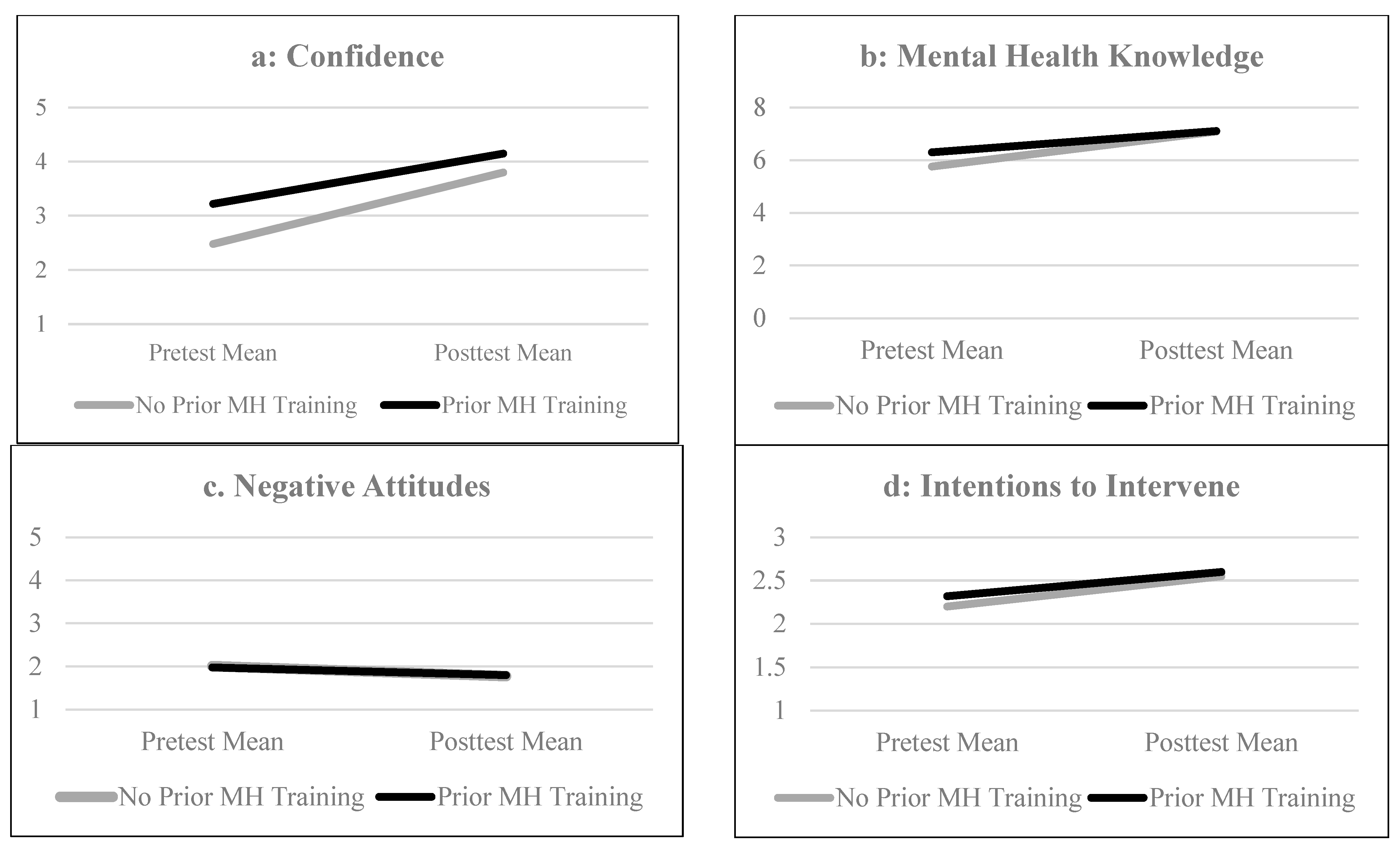
The within-subjects main effect was statistically significant for confidence (F [1] = 17.05, p < 0.001, ηp2 = 0.06), mental health knowledge (F [1] = 10.02, p < 0.002, ηp2 = 0.04), and intentions to intervene (F [1] = 12.19, p < 0.001, ηp2 = 0.04) but did not attain statistical significance for negative attitudes (F [1] = 2.10, p = 0.15, ηp2 = 0.01). These results suggest that completion of the YMHFA program had a meaningful and positive effect on teachers’ levels of confidence, knowledge, and intentions to intervene. Among the full sample, the average confidence score increased by 52%, mental health knowledge increased by 20%, and intentions to intervene increased by 15%. Figure 1 displays changes in the pretest and posttest means for each training outcome separated by prior training group.
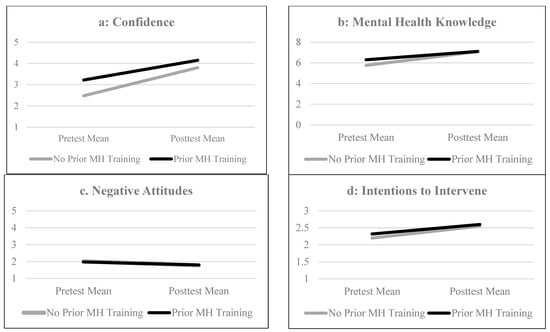
Figure 1.
Between-subjects effects of prior mental health training across time points. Note: Covariates include female, White race, graduate degree, years worked with students, and frequency of interactions about student mental health. Confidence: n = 303, mental health knowledge: n = 294; negative attitudes: n = 306; intentions to intervene: n = 297.
The between-subjects effect for prior training was statistically significant for confidence (F [1] = 54.66, p < 0.001, ηp2 = 0.16) and mental health knowledge (F [1] = 7.99, p < 0.01, ηp2 = 0.03). Figure 1a shows positive trend lines, which reflect improvement in confidence from pretest to posttest, for both training groups. The group with no prior training showed a higher mean difference (MD) from pretest to posttest, suggesting that teachers with no prior training experienced a greater rate of improvement in confidence after YMHFA (no prior training MD = 1.32, SE = 0.06, p < 0.001; prior training MD = 0.96, SE = 0.09, p < 0.001). However, compared to teachers with prior mental health training, the group with no prior training remained lower on confidence after completion of the YMHFA program (MD across training groups at pretest = 0.72, SE = 0.10, p < 0.001; MD across training groups at posttest = 0.36, SE = 0.08, p < 0.001).
Figure 1b displays trends for mental health knowledge across training groups. Compared to the group with prior mental health training, the group with no training had a lower average score on the pretest survey, however these differences diminished after completion of the YMHFA training program (MD across training groups at pretest = 0.77, SE = 0.24, p < 0.01; MD across training groups at posttest = 0.05, SE = 0.12, p = 0.68). Figure 1c plots the pretest and posttest means for negative attitudes. No meaningful changes in negative attitudes were observed from pretest to posttest (F [1] = 2.10, p = 0.15, ηp2 = 0.01) and this was consistent across training groups (between-subjects effect: F [1] = 0.57, p = 0.45, ηp2 = 0.00). Figure 1d plots the pretest and posttest means for intentions to intervene. Although intentions to intervene showed statistically significant improvements after the training among the full sample, prior training history did not interact with time in a meaningful way (F [1] = 3.35, p = 0.07, ηp2 = 0.01).
3.3. Research Question 3: Satisfaction with YMHFA Across Past Training Experiences
The third research question assessed whether satisfaction with the YMHFA training differed between teachers with and without prior mental health training. Preliminary bivariate analysis, using an independent samples t-test, showed no meaningful differences in training satisfaction across participants who did (M = 4.40, SD = 0.59) and did not (M = 4.45, SD = 0.64) report prior mental health training (t [297] = −0.72, p = 0.47). Therefore, we do not report OLS regression results as no statistically significant bivariate differences in satisfaction were observed across the independent variable (i.e., prior training history). These results suggest that YMHFA satisfaction scores were high among this sample of teachers, regardless of their previous training experiences.
4. Discussion
Using data from a pretest/posttest evaluation of the Youth Mental Health First Aid (YMHFA) training in one school district in a southeastern state in the United States, the purpose of the current study was to examine the role of prior mental health training in shaping how teachers respond to the YMHFA program. Specifically, the study investigated differences in teachers’ confidence, mental health knowledge, negative attitudes, help-seeking intentions, and satisfaction with the training across those with and without prior mental health training. One key takeaway from this study’s findings is that, after completion of the YMHFA training program, participants showed meaningful improvement in three of the four constructs (confidence, mental health knowledge, and intentions to intervene) and reported positive training experiences. These findings are consistent with prior YMHFA research involving educators (e.g., Childs et al., 2020; Jorm et al., 2010) and highlight some of the short-term benefits of adopting the YMHFA curriculum as a professional development tool for improving different dimensions of teachers’ mental health literacy.
Our first research question explored whether baseline scores on the four constructs of interest differed across teachers’ previous mental health training experiences. Teachers who reported prior mental health training scored substantially higher on confidence and mental health knowledge and somewhat higher on intentions to intervene, even after controlling for important individual (e.g., race/ethnicity, sex) and work-related (e.g., graduate degree earned, frequency of student interactions) factors. There are two important points to make about these findings. First, these differences provide broad support for the delivery of mental health prevention training programs to teachers. Both confidence and knowledge are indicators of teachers’ beliefs about their capabilities and competence (i.e., teacher self-efficacy, see Zee & Koomen, 2016). A large body of research highlights the importance of teachers’ self-efficacy and the strong and positive link to teaching quality, classroom management, and student engagement (Klassen & Tze, 2014; Lauermann & ten Hagen, 2021; Zee & Koomen, 2020). Applying this research to mental health prevention training, it is likely that teachers’ confidence and knowledge about youth mental health is linked to the frequency and quality of teachers’ mental health support in the classroom. Higher teacher confidence and help-seeking intentions, brought about by mental health prevention training, are likely to increase the chances that teachers will take action to identify or prevent future mental health challenges among their students.
Second, these differences show that, even when participants are from the same profession (i.e., teachers), all YMHFA participants are not the same at baseline (e.g., before the training). Notably, these differences appear to be associated with at least one identifiable, work-related characteristic, which is prior mental health prevention training experiences. Future YMHFA studies should replicate these findings and investigate in greater depth any possible ceiling effects due to teachers’ prior mental health training experiences and/or their baseline scores. It is important to examine more closely how and under what circumstances these possible ceiling effects could lead to misleading interpretations of YMHFA effectiveness among teachers and other helping professionals.
The second research question focused on differences in YMHFA outcomes based on whether participants had previous mental health training. Differences in the average rate of improvement in confidence and mental health knowledge were found across prior training groups. Both groups experienced significant increases in confidence after completion of the YMHFA training. This finding reinforces prior research that has shown increases in confidence and self-efficacy after completing the YMHFA program (e.g., Jorm et al., 2010; Ross et al., 2023). However, confidence was notably higher at both pretest and posttest among participants with previous mental health training. The consistently higher levels of confidence, combined with the significant increase in confidence after YMHFA training (among those with prior mental health training experiences), suggests that YMHFA may serve as an effective “confidence booster” for those who have already had prior mental health prevention training.
Group differences in mental health knowledge showed a different pattern. The group with no prior mental health training scored lower on mental health knowledge on the pretest survey. However, after YMHFA, this group caught up to the group with prior mental health training (i.e., no group differences in mental health knowledge at posttest). Although not statistically significant, a similar pattern of “catch up” was observed for help-seeking intentions. Teachers with no prior training scored marginally lower on intentions to intervene at pretest, but no significant group differences were present at posttest. Thus, the YMHFA training seems to be slightly more effective at enhancing teachers’ mental health knowledge and help-seeking intentions when they have never received prior mental health training.
No meaningful differences in negative attitudes were observed from the pretest to the posttest survey. However, the teachers in this sample did not report negative attitudes about youth mental health at pretest or posttest, and this finding was consistent across prior training experiences. This finding represents a notable example of the potential ceiling effect discussed previously. Since the teachers in this sample held positive attitudes as baseline, there was not much room for attitudes to improve after completion of the training. Importantly, this observation should not be interpreted as an issue of training effectiveness, but as a consequence of participants having little opportunity for the training curriculum to improve attitude scores because they were already high at baseline (i.e., ceiling effects).
Our final research question considered whether satisfaction with the YMHFA program differed across prior training groups. Results indicated that no differences in training satisfaction were observed across training groups. Like other YMHFA studies (e.g., police: Soderstrom et al., 2024; teachers: Ross et al., 2023), satisfaction with the YMHFA training was high among the full sample of teachers. Robust findings within the training transfer literature indicate that trainees who report higher training engagement, alignment with the training content and their job responsibilities, and overall positive training experiences are more likely to transfer the learned skills into their work and overall job responsibilities (Blume et al., 2019; Hutchins, 2009; Yamnill & McLean, 2001). Thus, widespread satisfaction among participants with diverse prior training experiences and work role characteristics seems to be another key benefit of YMHFA.
4.1. Limitations and Future Research
There are some limitations to our study that should be acknowledged. First, the sample consisted of teachers at five schools from one school district. As a result, the generalizability of findings to other school districts is unknown. Second, measures to assess training fidelity were not collected. However, it is important to note that instructors who delivered the training were certified by the NCWB. Third, this study did not include a follow-up period, which prevents assessments of the longevity of observed training impacts. Fourth, the individual characteristics (e.g., sex, race/ethnicity) of participants measured in the current study were limited due to the length of the survey and the low prevalence of participants who selected most of the “other” race/ethnicity categories. Therefore, another limitation is the lack of variables representing participants’ social identities, such as cultural heritage, self-reported gender, or socioeconomic status. Finally, our measure of prior mental health training experiences was limited to a dichotomous indicator, without the ability to account for important training characteristics such as the recency of prior training, name/curriculum of training, or training content or topics covered.
Despite these limitations, findings from this study can help set the stage for future research on the benefits of YMHFA within education settings. The delivery of YMHFA, as a professional development tool for teachers, whether mandated by local or state policy or delivered through school-based intervention programs, is readily occurring in school systems across the United States (e.g., Florida Department of Education, n.d.; Texas Education Agency, n.d.; Washington Office of Superintendent of Public Instruction, n.d.) and beyond (e.g., Jorm et al., 2010; Kidger et al., 2016). Such widespread implementation of this training program provides the opportunity for researchers to engage in the next phase of research on YMHFA, one that involves longitudinal evaluations of mental health literacy and helping behaviors. Qualitative studies (e.g., focus groups, observational) that assess changes in teachers’ mental health responses in the classroom and what factors lead to the possible decay in the application of YMHFA skills are important. For example, a qualitative assessment of when, how often, and under what circumstances teachers apply the ALGEE framework when encountering youth with potential mental health challenges would be a substantial extension and enhancement to current research.
Quantitative studies should strive to include additional time points beyond pretest and posttest survey designs. The number of studies that include (1) samples of teachers and (2) one or more follow-up periods is low, and their results are mixed (e.g., Haggerty et al., 2019; Jorm et al., 2010). Additional evaluations of YMHFA that include repeated measures designs will help clarify how well teachers maintain positive training outcomes observed in this study and other pretest and posttest designs. Collecting additional data about prior professional development experiences may enhance this line of inquiry by examining how previous mental health prevention training experiences impact YMHFA program effectiveness, including baseline scores on dimensions of mental health literacy and changes over time. Finally, future studies should consider expanding the individual and work-related characteristics used to explore differences in YMHFA training outcomes. Considering factors such as teachers’ job satisfaction, perceptions of organizational support, social identities (e.g., cultural heritage, self-reported gender), and self-assessment of one’s own mental health could offer a more comprehensive understanding of the variations in YMHFA outcomes among teachers.
4.2. Conclusions
Findings from this study provide additional support for the use of YMHFA as a professional development tool aimed at improving dimensions of mental health literacy among teachers. By extending the prior literature on YMHFA outcomes to focus specifically on teachers and the role of prior mental health training, this study contributes to a growing body of research supporting the utility of YMHFA in educational settings. YMHFA training can serve as an effective professional development tool when the objective is to improve teachers’ confidence, knowledge, and help-seeking intentions. Regardless of prior mental health training, teachers in our sample reported higher levels of confidence, mental health knowledge, and help-seeking intentions after participating in YMHFA. Teachers also reported high training satisfaction.
Our findings lay the groundwork for future studies to investigate how prior mental health training experiences impact training retention and decay across key YMHFA constructs and time points. In the current study, prior mental health training did matter. Teachers with prior training scored higher at baseline and experienced a smaller magnitude of change from pretest to posttest. These findings raise important questions about the scalability of YMHFA. Specifically, the results highlight the need to determine whether large-scale, universal implementation is necessary, or whether a tiered implementation that prioritizes professionals with no prior training would be more efficient (see Elligson et al., 2021). These questions are not only for future research inquiries, but also for school administrators and other stakeholders to consider when identifying training priorities and resources and developing training plans. Teachers’ time is already spread thin, as they balance multiple responsibilities such as lesson planning, administrative tasks, classroom management, and increasingly, providing emotional support to students. This means that professional development opportunities must be enjoyable, applicable to their work role, and provide observable, long-term benefits. Research must continue to investigate whether the YMHFA program can successfully meet all three of these characteristics to solidify its role as an effective professional development tool for enhancing teachers’ ability to support their students’ mental health.
Author Contributions
Conceptualization, K.K.C., J.H.P. and K.G.; Methodology, K.K.C. and J.H.P.; Formal analysis, K.K.C.; Data curation, K.K.C.; Writing—original draft, K.K.C., J.H.P. and K.G.; Writing—review & editing, J.H.P. and K.G.; Project administration, K.K.C. and K.G.; Funding acquisition, K.K.C. and K.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by National Institute of Justice, grant number 2014-CK-BX-0014.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. University of Central Florida Review Board #1, IRB00001138 11 March 2015.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets presented in this article are not readily available due to confidentiality protections.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Aakre, J. M., Lucksted, A., & Browning-McNee, L. A. (2016). Evaluation of youth mental health first aid USA: A program to assist young people in psychological distress. Psychological Services, 13(2), 121. [Google Scholar] [CrossRef] [PubMed]
- Adelman, H. S., & Taylor, L. (Eds.). (2009). Mental health in schools: Engaging learners, preventing problems, and improving schools. Corwin Press. [Google Scholar]
- Adelman, H. S., & Taylor, L. (2012). Mental health in schools: Moving in new directions. Contemporary School Psychology, 16(1), 9–18. [Google Scholar] [CrossRef]
- Allison, P. D. (1999). Multiple regression: A primer. Pine Forge Press. [Google Scholar]
- Atkins, M. S., Hoagwood, K. E., Kutash, K., & Seidman, E. (2010). Toward the integration of education and mental health in schools. Administration and Policy in Mental Health and Mental Health Services Research, 37, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Blume, B. D., Ford, J. K., Surface, E. A., & Olenick, J. (2019). A dynamic model of training transfer. Human Resource Management Review, 29(2), 270–283. [Google Scholar] [CrossRef]
- Bommersbach, T. J., McKean, A. J., Olfson, M., & Rhee, T. G. (2023). National trends in mental health–related emergency department visits among youth, 2011–2020. JAMA, 329(17), 1469–1477. [Google Scholar] [CrossRef] [PubMed]
- Brady, C. M., & Childs, K. K. (2023). Implementation and evaluation of a juvenile mental health training for law enforcement in a medium-sized jurisdiction. Behavioral Sciences & the Law, 41(1), 1–18. [Google Scholar]
- Burnette, C., Ramchand, R., & Ayer, L. (2015). Gatekeeper training for suicide prevention: Theoretical model and review of the empirical literature. Rand Health Quarterly, 5(1), 16. [Google Scholar] [PubMed]
- Childs, K. K., Bryson, S. L., Peck, J. H., Gryglewicz, K., & Potter, R. H. (2019). Brevard public schools school safety and climate study: Final summary overview. Available online: https://www.ojp.gov/library/publications/brevard-public-schools-school-safety-and-climate-study-final-summary-overview (accessed on 15 July 2025).
- Childs, K. K., Gryglewicz, K., & Elligson, R. (2020). An assessment of the utility of the Youth Mental Health First Aid Training: Effectiveness, satisfaction, and universality. Community Mental Health Journal, 56(8), 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Davidson, M. L. (2016). A criminal justice system-wide response to mental illness: Evaluating the effectiveness of the Memphis Crisis Intervention Team training curriculum among law enforcement and correctional officers. Criminal Justice Policy Review, 27(1), 46–75. [Google Scholar] [CrossRef]
- Elligson, R. L., Jr., Childs, K. K., & Gryglewicz, K. (2021). Youth mental health first aid: Examining the influence of pre-existing attitudes and knowledge on training effectiveness. The Journal of Primary Prevention, 42(6), 549–565. [Google Scholar] [CrossRef] [PubMed]
- Florida Department of Education. (n.d.) Florida AWARE program model. Available online: https://www.fldoe.org/core/fileparse.php/18612/urlt/Florida-AWARE-Program-Model.pdf (accessed on 15 July 2025).
- Geierstanger, S., Yu, J., Saphir, M., & Soleimanpour, S. (2024). Youth mental health first aid training: Impact on the ability to recognize and support youth needs. The Journal of Behavioral Health Services & Research, 51(4), 588–598. [Google Scholar] [CrossRef] [PubMed]
- Gili, M., Castellví, P., Vives, M., de la Torre-Luque, A., Almenara, J., Blasco, M. J., Cebrià, A. I., Gabilondo, A., Pérez-Ara, M. A., Miranda-Mendizábal, A., Lagares, C., Parés-Badell, O., Piqueras, J. A., Rodríguez-Jimínez, T., Rodríguez-Marin, J., Soto-Sanz, V., Alonso, J., & Roca, M. (2019). Mental disorders as risk factors for suicidal behavior in young people: A meta-analysis and systematic review of longitudinal studies. Journal of Affective Disorders, 245, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, K. M., Christensen, H., Jorm, A. F., Evans, K., & Grove, C. (2004). Effect of web-based depression literacy and cognitive behavioural therapy interventions on stigmatising attitudes to depression. The British Journal of Psychiatry, 185(4), 342–349. [Google Scholar] [CrossRef] [PubMed]
- Gryglewicz, K., Childs, K. K., & Soderstrom, M. F. (2018). An evaluation of youth mental health first aid training in school settings. School Mental Health, 10, 48–60. [Google Scholar] [CrossRef]
- Gryglewicz, K., Gleason, L., Chen, J., Steding, L., Monahan, M., Jordan-Arthur, B., Brown, R., Bozzay, M., Romero, G., Rakhshani, A., Sulbaran, A., Ruiz Chavez, D., Witmeier, M., & Karver, M. (2015). Florida youth suicide prevention project. Substance Abuse and Mental Health Service Administration. [Google Scholar]
- Hadlaczky, G., Hökby, S., Mkrtchian, A., Carli, V., & Wasserman, D. (2014). Mental Health First Aid is an effective public health intervention for improving knowledge, attitudes, and behavior: A meta-analysis. International Review of Psychiatry, 26(4), 467–475. [Google Scholar] [CrossRef] [PubMed]
- Haggerty, D., Carlson, J. S., McNall, M., Lee, K., & Williams, S. (2019). Exploring youth mental health first aider training outcomes by workforce affiliation: A survey of project AWARE participants. School Mental Health, 11, 345–356. [Google Scholar] [CrossRef]
- Hutchins, H. M. (2009). In the trainer’s voice: A study of training transfer practices. Performance Improvement Quarterly, 22(1), 69–93. [Google Scholar] [CrossRef]
- Isaac, M., Elias, B., Katz, L. Y., Belik, S. L., Deane, F. P., Enns, M. W., Sareen, J., & Swampy Cree Suicide Prevention Team. (2009). Gatekeeper training as a preventative intervention for suicide: A systematic review. The Canadian Journal of Psychiatry, 54(4), 260–268. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A. F. (2000). Mental health literacy: Public knowledge and beliefs about mental disorders. The British Journal of Psychiatry, 177(5), 396–401. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A. F., Kitchener, B. A., & Mugford, S. K. (2005). Experiences in applying skills learned in a Mental Health First Aid training course: A qualitative study of participants’ stories. BMC Psychiatry, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A. F., Kitchener, B. A., Sawyer, M. G., Scales, H., & Cvetkovski, S. (2010). Mental Health First Aid training for high school teachers: A cluster randomized trial. BMC Psychiatry, 10, 51. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C. M., Mithen, J. M., Fischer, J. A., Kitchener, B. A., Jorm, A. F., Lowe, A., & Scanlan, C. (2011). Youth Mental Health First Aid: A description of the program and an initial evaluation. International Journal of Mental Health Systems, 5(1), 4. [Google Scholar] [CrossRef] [PubMed]
- Kidger, J., Stone, T., Tilling, K., Brockman, R., Campbell, R., Ford, T., Hollingworth, W., King, M., Araya, R., & Gunnell, D. (2016). A pilot cluster randomised controlled trial of a support and training intervention to improve the mental health of secondary school teachers and students—The WISE (Wellbeing in Secondary Education) study. BMC Public Health, 16, 1060. [Google Scholar] [CrossRef] [PubMed]
- Kitchener, B. A., & Jorm, A. F. (2002). Mental Health First Aid training for the public: Evaluation of effects on knowledge, attitudes and helping behavior. BMC Psychiatry, 2, 10. [Google Scholar] [CrossRef] [PubMed]
- Kitchener, B. A., & Jorm, A. F. (2004). Mental Health First Aid training in a workplace setting: A randomized controlled trial. BMC Psychiatry, 4, 23. [Google Scholar] [CrossRef] [PubMed]
- Klassen, R. M., & Tze, V. M. (2014). Teachers’ self-efficacy, personality, and teaching effectiveness: A meta-analysis. Educational Research Review, 12, 59–76. [Google Scholar] [CrossRef]
- Kutcher, S., Bagnell, A., & Wei, Y. (2015). Mental health literacy in secondary schools: A Canadian approach. Child & Adolescent Psychiatric Clinics of North America, 24(2), 233–244. [Google Scholar]
- Kutcher, S., Wei, Y., & Coniglio, C. (2016). Mental health literacy: Past, present, and future. The Canadian Journal of Psychiatry, 61(3), 154–158. [Google Scholar] [CrossRef] [PubMed]
- Lauermann, F., & ten Hagen, I. (2021). Do teachers’ perceived teaching competence and self-efficacy affect students’ academic outcomes? A closer look at student-reported classroom processes and outcomes. Educational Psychologist, 56(4), 265–282. [Google Scholar] [CrossRef]
- Marsico, K. F., Wang, C., & Liu, J. L. (2022). Effectiveness of Youth Mental Health First Aid training for parents at school. Psychology in the Schools, 59(8), 1701–1716. [Google Scholar] [CrossRef]
- Mental Health First Aid. (n.d.) U.S. reach. Available online: https://www.mentalhealthfirstaid.org/us-reach/ (accessed on 7 April 2025).
- Ng, S. H., Tan, N. J. H., Luo, Y., Goh, W. S., Ho, R., & Ho, C. S. H. (2021). A systematic review of youth and teen mental health first aid: Improving adolescent mental health. Journal of Adolescent Health, 69(2), 199–210. [Google Scholar] [CrossRef] [PubMed]
- Noltemeyer, A., Huang, H., Meehan, C., Jordan, E., Morio, K., Shaw, K., & Oberlin, K. (2020). Youth mental health first aid: Initial outcomes of a statewide rollout in Ohio. Journal of Applied School Psychology, 36(1), 1–19. [Google Scholar] [CrossRef]
- Piao, J., Huang, Y., Han, C., Li, Y., Xu, Y., Liu, Y., & He, X. (2022). Alarming changes in the global burden of mental disorders in children and adolescents from 1990 to 2019: A systematic analysis for the Global Burden of Disease study. European Child & Adolescent Psychiatry, 31(11), 1827–1845. [Google Scholar] [CrossRef] [PubMed]
- Rose, T., Leitch, J., Collins, K. S., Frey, J. J., & Osteen, P. J. (2019). Effectiveness of youth mental health first aid USA for social work students. Research on Social Work Practice, 29(3), 291–302. [Google Scholar] [CrossRef]
- Ross, A. S., Wang, C., & Liu, J. L. (2023). Youth mental health first aid training with diverse educators. Psychological Services, 20(4), 941–951. [Google Scholar] [CrossRef] [PubMed]
- Sagar, R., & Pattanayak, R. D. (2016). Suicidality and mood disorders: Gatekeepers’ training and mental health first aid. Journal of Mental Health and Human Behavior, 21(2), 85. [Google Scholar] [CrossRef]
- Sánchez, A. M., Latimer, J. D., Scarimbolo, K., von der Embse, N. P., Suldo, S. M., & Salvatore, C. R. (2021). Youth mental health first aid (Y-MHFA) trainings for educators: A systematic review. School Mental Health, 13(1), 1–12. [Google Scholar] [CrossRef]
- Soderstrom, M. F. P., Childs, K. K., & Gryglewicz, K. (2024). An evaluation of youth mental health first aid training with law enforcement officers. Psychological Services. advance online publication. [Google Scholar]
- Texas Education Agency. (n.d.). Educator preparation programs (EPP) resources. Available online: https://tea.texas.gov/about-tea/other-services/mental-health/educator-preparation-programs-epp-resources (accessed on 15 July 2025).
- Washington Office of Superintendent of Public Instruction. (n.d.) Project AWARE. Available online: https://ospi.k12.wa.us/student-success/health-safety/school-safety-center/mental-social-behavioral-health/project-aware (accessed on 15 July 2025).
- Yamnill, S., & McLean, G. N. (2001). Theories supporting transfer of training. Human Resource Development Quarterly, 12(2), 195–208. [Google Scholar] [CrossRef]
- Zee, M., & Koomen, H. (2020). Engaging children in the upper elementary grades: Unique contributions of teacher self-efficacy, autonomy support, and student-teacher relationships. Journal of Research in Childhood Education, 34(4), 477–495. [Google Scholar] [CrossRef]
- Zee, M., & Koomen, H. M. Y. (2016). Teacher self-efficacy and its effects on classroom processes, student academic adjustment, and teacher well-being: A synthesis of 40 years of research. Review of Educational Research, 86(4), 981–1015. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).