
Caries-Free Prevalence among Schoolchildren in Malaysia—Time-Series Analysis of Trends and Projections from 1996 to 2030

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants, Data Source and Description
2.2. Data Analysis
3. Results
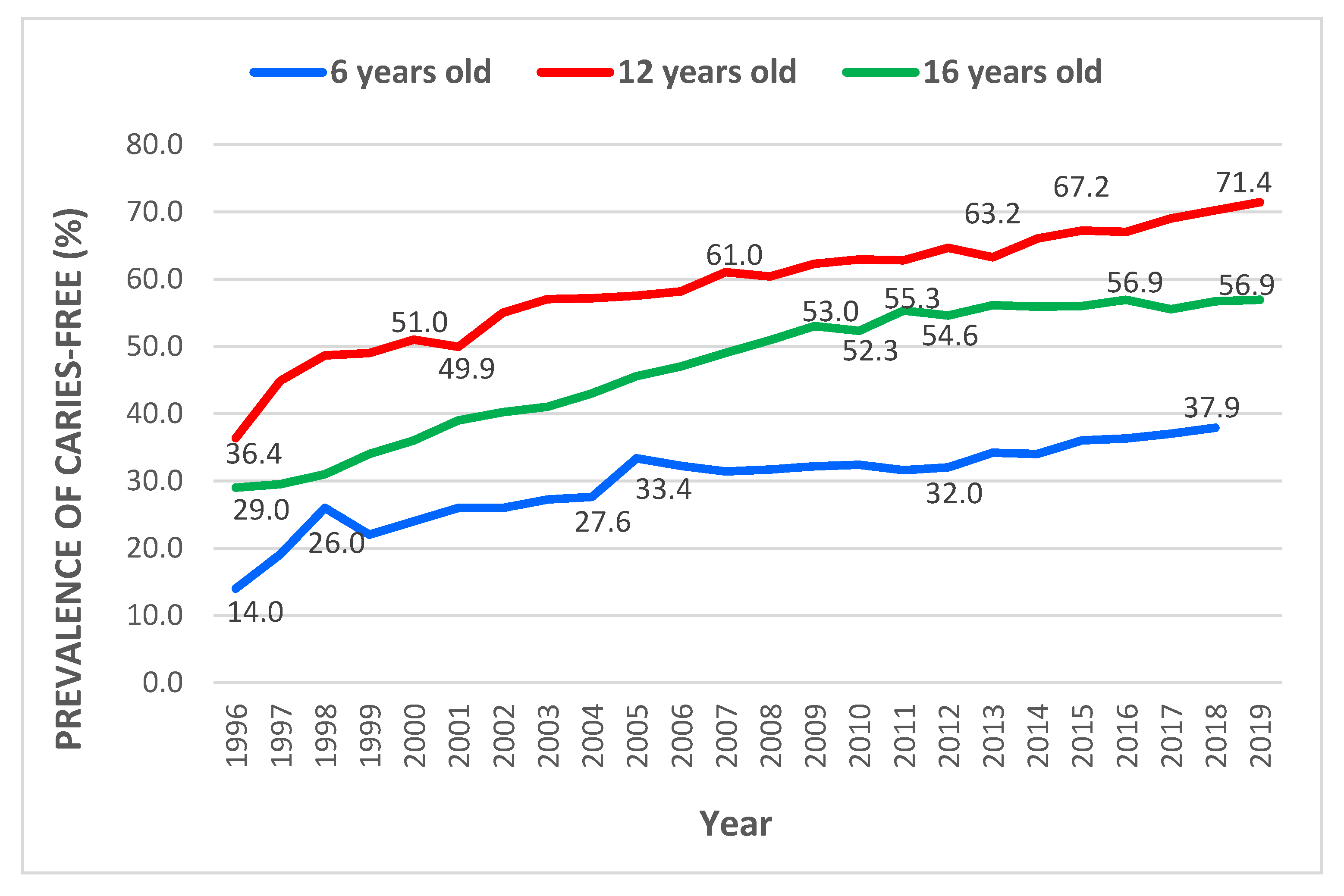
3.1. Trends of Caries-Free Prevalence among 6-, 12- and 16-Year-Old Schoolchildren in Malaysia from 1996 to 2019
3.2. Selection of the Best Time Series Model for Projecting Caries-Free Prevalence for Each Age Group
3.3. Projection of Caries-Free Prevalence in 6-, 12- and 16-Year-Old Schoolchildren until 2030
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kassebaum, N.J.; Smith, A.G.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.; Marcenes, W.; Collaborators, G.O.H. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the global burden of diseases, injuries, and risk factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Qiu, W.; Zhou, Y.; Li, Z.; Huang, T.; Xiao, Y.; Cheng, L.; Peng, X.; Zhang, L.; Ren, B. Application of antibiotics/antimicrobial agents on dental caries. BioMed Res. Int. 2020, 2020, 5658212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quock, R.L. Dental caries: A current understanding and implications. J. Nat. Sci. 2015, 1, 27. [Google Scholar]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Stephens, M.B.; Wiedemer, J.P.; Kushner, G.M. Dental problems in primary care. Am. Fam. Physician 2018, 98, 654–660. [Google Scholar]
- Crall, J.J.; Vujicic, M. Children’s Oral Health: Progress, Policy Development, And Priorities For Continued Improvement: Study examines improvements in American children’s oral health and oral health care that stem from major federal and state initiatives, and persistent disparities. Health Aff. 2020, 39, 1762–1769. [Google Scholar]
- Bönecker, M.; Abanto, J.; Tello, G.; Oliveira, L.B. Impact of dental caries on preschool children’s quality of life: An update. Braz. Oral Res. 2012, 26, 103–107. [Google Scholar] [CrossRef] [Green Version]
- WHO. Sugar and Dental Caries; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Kundu, H.; Patthi, B.; Singla, A.; Jankiram, C.; Jain, S.; Singh, K. Dental caries scenario among 5, 12 and 15-year-old children in India-A retrospective analysis. J. Clin. Diagn. Res. JCDR 2015, 9, ZE01. [Google Scholar] [CrossRef]
- UNICEF. The State of the World’s Children 2019: Children, Food and Nutrition: Growing Well in a Changing World; UNICEF: Pyrmont, Australia, 2019. [Google Scholar]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef]
- Pitts, N.; Mayne, C. A Global Consensus for Achieving a Dental Cavity-Free Future. 2021. Available online: https://kclpure.kcl.ac.uk/portal/en/publications/a-global-consensus-for-achieving-a-dental-cavityfree-future(c3b4777e-f615-4a5e-934d-e47a11843183).html (accessed on 2 December 2022).
- Nohss, O.H.D.; Ministry of Health Malaysia. National Oral Health Survey of School Children. In Volume II: Oral Health Status of 12-Year-Old School Children; University of Adelaide Press: Adelaide, Australia, 2017; Volume II. [Google Scholar]
- NOHPS, O.H.D.; Ministry of Health Malaysia. National Oral Health Survey of Preschool Children 2015 (NOHPS 2015). In Oral Health Status and Caries Treatment Needs of 5-Year-Old Children; Ministry of Health: Putrajaya, Malaysia, 2015; Volume 1, pp. 3–58. [Google Scholar]
- Rozier, R.G.; White, B.A.; Slade, G.D. Trends in oral diseases in the US population. J. Dent. Educ. 2017, 81, eS97–eS109. [Google Scholar] [CrossRef]
- Ahmar, A.S.; Boj, E. The date predicted 200.000 cases of Covid-19 in Spain. J. Appl. Sci. Eng. Technol. Educ. 2020, 2, 188–193. [Google Scholar] [CrossRef]
- Xi, J.-Y.; Lin, X.; Hao, Y.-T. Measurement and projection of the burden of disease attributable to population aging in 188 countries, 1990–2050: A population-based study. J. Glob. Health 2022, 12, 04093. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.; Abllah, Z.; Radhi, N.A.M.; Musa, S.; Halim, M.F.A.A. Time-series forecasting analysis on the major treatment need among patients referred for periodontal and conservative treatments in IIUM Dental Outpatient Clinic. J. Int. Oral Health 2021, 13, 485. [Google Scholar]
- Zhang, X.; Zhang, L.; Zhang, Y.; Liao, Z.; Song, J. Predicting trend of early childhood caries in mainland China: A combined meta-analytic and mathematical modelling approach based on epidemiological surveys. Sci. Rep. 2017, 7, 6507. [Google Scholar]
- Jordan, R.A.; Krois, J.; Schiffner, U.; Micheelis, W.; Schwendicke, F. Trends in caries experience in the permanent dentition in Germany 1997–2014, and projection to 2030: Morbidity shifts in an aging society. Sci. Rep. 2019, 9, 5534. [Google Scholar] [CrossRef]
- Nagarajan, R.; Panny, A.; Ryan, M.; Murphy, S.; Vujicic, M.; Nycz, G. Forecasting Preventive Dental Quality Measures. medRxiv 2021. [Google Scholar] [CrossRef]
- Tiwari, R.; Bhayat, A.; Chikte, U. Forecasting for the need of dentists and specialists in South Africa until 2030. PLoS ONE 2021, 16, e0251238. [Google Scholar] [CrossRef]
- Glick, M.; Williams, D.M. FDI vision 2030: Delivering optimal oral health for all. Int. Dent. J. 2021, 71, 3. [Google Scholar] [CrossRef]
- Hyndman, R.J.; George, A. Forecasting: Principles and Practice, 2nd ed.; OTexts: Melbourne, Australia, 2018. [Google Scholar]
- Hyndman, R.J.; Kostenko, A.V. Minimum sample size requirements for seasonal forecasting models. Foresight 2007, 6, 12–15. [Google Scholar]
- Al-Qazzaz, R.A.; Yousif, S.A. High performance time series models using auto autoregressive integrated moving average. Indones. J. Electr. Eng. Comput. Sci. 2022, 27, 422–430. [Google Scholar] [CrossRef]
- Booranawong, T.; Booranawong, A. Simple and double exponential smoothing methods with designed input data for forecasting a seasonal time series: In an application for lime prices in Thailand. Suranaree J. Sci. Technol. 2017, 24, 301–310. [Google Scholar]
- Lazim, M. Introductory Business Forecasting. A Practical Approach, 3rd ed.; Routledge: Abingdon, UK, 2013. [Google Scholar]
- Abdulgader, Q.M. Time series forecasting using ARIMA methodology with application on census data in Iraq. Sci. J. Univ. Zakho 2016, 4, 258–268. [Google Scholar] [CrossRef]
- Chatfield, M.J.; Borman, P.J. Acceptance criteria for method equivalency assessments. Anal. Chem. 2009, 81, 9841–9848. [Google Scholar] [PubMed]
- Kolassa, S. Why the “best” point forecast depends on the error or accuracy measure. Int. J. Forecast. 2020, 36, 208–211. [Google Scholar] [CrossRef]
- Lewis, C. International and Business Forecasting Methods; Butterworths: London, UK, 1982; p. 144. [Google Scholar]
- Kazeminia, M.; Abdi, A.; Shohaimi, S.; Jalali, R.; Vaisi-Raygani, A.; Salari, N.; Mohammadi, M. Dental caries in primary and permanent teeth in children’s worldwide, 1995 to 2019: A systematic review and meta-analysis. Head Face Med. 2020, 16, 1–21. [Google Scholar]
- Goldberg, M. Deciduous tooth and dental caries. Ann. Pediatr. Child Health 2017, 5, 1120. [Google Scholar]
- Mendes, F.M.; Braga, M.M. Caries detection in primary teeth is less challenging than in permanent teeth. Dent. Hypotheses 2013, 4, 17–20. [Google Scholar] [CrossRef]
- Health, M.O. Annual Report 2020. 2020. Oral Health Division, Ministry of Health Malaysia: Putrajaya, 2020. Available online: https://ohd.moh.gov.my/images/pdf/annual_rpt/annual_%20rpt20.pdf (accessed on 3 December 2022).
- Bohari, N.F.M.; Kruger, E.; John, J.; Tennant, M. Analysis of dental services distribution in Malaysia: A geographic information systems–based approach. Int. Dent. J. 2019, 69, 223–229. [Google Scholar] [CrossRef]
- Karim, F.A.; Yusof, Z.Y.M.; Nor, N.A.M. Water Fluoridation And Oral Health In Malaysia: A Review Of Literature. J. Health Transl. Med. 2020, 23, 76–91. [Google Scholar]
- Mahfouz, M.; Abu Esaid, A. Dental caries prevalence among 12–15 year old Palestinian children. Int. Sch. Res. Not. 2014, 2014, 785404. [Google Scholar] [CrossRef]
- Murray, J.; Vernazza, C.; Holmes, R. Forty years of national surveys: An overview of children’s dental health from 1973–2013. Br. Dent. J. 2015, 219, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Ab Mumin, N.; Yusof, Z.Y.M.; Marhazlinda, J.; Obaidellah, U. Exploring the opinions of secondary school students on the strengths and weaknesses of the school dental service in Selangor, Malaysia: A qualitative study. BMC Oral Health 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zemaitiene, M.; Grigalauskiene, R.; Andruskeviciene, V.; Matulaitiene, Z.K.; Zubiene, J.; Narbutaite, J.; Slabsinskiene, E. Dental caries risk indicators in early childhood and their association with caries polarization in adolescence: A cross-sectional study. BMC Oral Health 2017, 17, 1–6. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Error Measures | Error Values | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 6 Years Old | 12 Years Old | 16 Years Old | |||||||
| DES | ETS (A,Ad,N) | ARIMA (0,1,0) | DES | ETS (A,Ad,N) | ARIMA (0,1,0) | DES | ETS (A,A,N) | ARIMA (0,1,0) | |
| MSE | 5.73 | 4.00 | 6.82 | 4.70 | 3.41 | 5.55 | 1.29 | 1.30 | 1.65 |
| RMSE | 2.39 | 2.00 | 2.61 | 2.17 | 1.85 | 2.36 | 1.14 | 1.14 | 1.28 |
| MAPE | 8.29 | 6.37 | 7.48 | 3.25 | 2.39 | 3.24 | 2.29 | 2.30 | 2.45 |
| MAD | 2.10 | 1.46 | 1.98 | 1.62 | 1.16 | 1.75 | 0.93 | 0.93 | 0.82 |
| ME | 0.95 | 0.29 | 0.001 | 0.68 | 0.35 | 0.002 | 0.39 | 1.53 | 0.004 |
| Error Measures | Error Values | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 6 Years Old | 12 Years Old | 16 Years Old | |||||||
| DES | ETS (A,Ad,N) | ARIMA (0,1,0) | DES | ETS (A,Ad,N) | ARIMA (0,1,0) | DES | ETS (A,A,N) | ARIMA (0,1,0) | |
| MSE | 14.92 | 4.25 | 2.64 | 1.69 | 4.95 | 6.17 | 3.41 | 2.77 | 19.68 |
| RMSE | 3.86 | 2.06 | 1.62 | 1.30 | 2.22 | 2.48 | 1.85 | 1.66 | 4.43 |
| MAPE | 9.78 | 4.92 | 4.18 | 1.75 | 2.89 | 3.35 | 3.11 | 2.78 | 7.06 |
| MAD | 3.59 | 1.82 | 1.52 | 1.22 | 2.02 | 2.33 | 1.57 | 1.75 | 3.32 |
| ME | 3.59 | 4.66 | 1.52 | 1.22 | 2.01 | 2.33 | 1.56 | 1.75 | 3.98 |
| Error Measures | Error Values | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 6 Years Old | 12 YEARS Old | 16 Years Old | |||||||
| DES | ETS (A,Ad,N) | ARIMA (0,1,0) | DES | ETS (A,Ad,N) | ARIMA (0,1,0) | DES | ETS (A,A,N) | ARIMA (0,1,0) | |
| MSE | 2.03 | 1.783 | 0.74 | 0.36 | 2.712 | 0.65 | 0.92 | 1.00 | 2.25 |
| RMSE | 1.42 | 1.33 | 0.86 | 0.60 | 1.64 | 0.80 | 0.96 | 1.00 | 1.50 |
| MAPE | 2.56 | 2.97 | 2.12 | 0.68 | 2.315 | 1.04 | 1.51 | 1.53 | 2.08 |
| MAD | 0.91 | 1.10 | 0.75 | 0.47 | 1.55 | 0.71 | 0.85 | 0.86 | 1.17 |
| ME | 0.73 | 1.10 | 0.40 | 0.47 | 1.61 | 0.61 | 0.21 | 0.27 | 1.17 |
| Forecasted Years Ahead | Caries-Free Prevalence (95%CI) | ||
|---|---|---|---|
| 6 Years Old | 12 Years Old | 16 Years Old | |
| 2019 | 38.99 (34.03, 43.95) | - | - |
| 2020 | 40.07 (33.06, 47.09) | 72.60 (68.38, 76.82) | 56.36 (53.98, 58.74) |
| 2021 | 41.16 (32.57, 49.75) | 73.91 (69.36, 78.45) | 56.41 (53.69, 59.13) |
| 2022 | 42.25 (32.33, 52.16) | 75.21 (70.01, 80.42) | 56.46 (53.10, 59.83) |
| 2023 | 43.33 (32.24, 54.42) | 76.52 (70.32, 82.72) | 56.51 (52.24, 60.79) |
| 2024 | 44.42 (32.27, 56.57) | 77.82 (70.32, 85.32) | 56.57 (51.17, 61.96) |
| 2025 | 45.50 (32.38, 58,63) | 79.13 (70.08, 88.18) | 56.62 (49.94, 63.31) |
| 2026 | 46.59 (32.56, 60.62) | 80.43 (69.62, 91.24) | 56.67 (48.54, 64.80) |
| 2027 | 47.68 (32.80, 62.55) | 81.74 (68.99, 94.48) | 56.72 (47.03, 66.41) |
| 2028 | 48.76 (33.08, 64.45) | 83.04 (68.20, 97.88) | 56.77 (45.41, 68.13) |
| 2029 | 49.85 (33.40, 66.30) | 84.35 (67.28, 101.42) | 56.82 (43.68, 69.96) |
| 2030 | 50.94 (33.76, 68.12) | 85.65 (66.22, 105.08) | 56.87 (41.86, 71.88) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najihah, L.; Husin, W.Z.W.; Jalal, T.M.T.; Marhazlinda, J. Caries-Free Prevalence among Schoolchildren in Malaysia—Time-Series Analysis of Trends and Projections from 1996 to 2030. Children 2023, 10, 264. https://doi.org/10.3390/children10020264
Najihah L, Husin WZW, Jalal TMT, Marhazlinda J. Caries-Free Prevalence among Schoolchildren in Malaysia—Time-Series Analysis of Trends and Projections from 1996 to 2030. Children. 2023; 10(2):264. https://doi.org/10.3390/children10020264
Chicago/Turabian StyleNajihah, Lokman, Wan Zakiyatussariroh Wan Husin, Tengku Mardhiah Tengku Jalal, and Jamaludin Marhazlinda. 2023. "Caries-Free Prevalence among Schoolchildren in Malaysia—Time-Series Analysis of Trends and Projections from 1996 to 2030" Children 10, no. 2: 264. https://doi.org/10.3390/children10020264