
Do We Need Palliative Care in Pediatric Nephrology? Patients’ and Caregivers’ Disease Experience

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Methods
3. Results
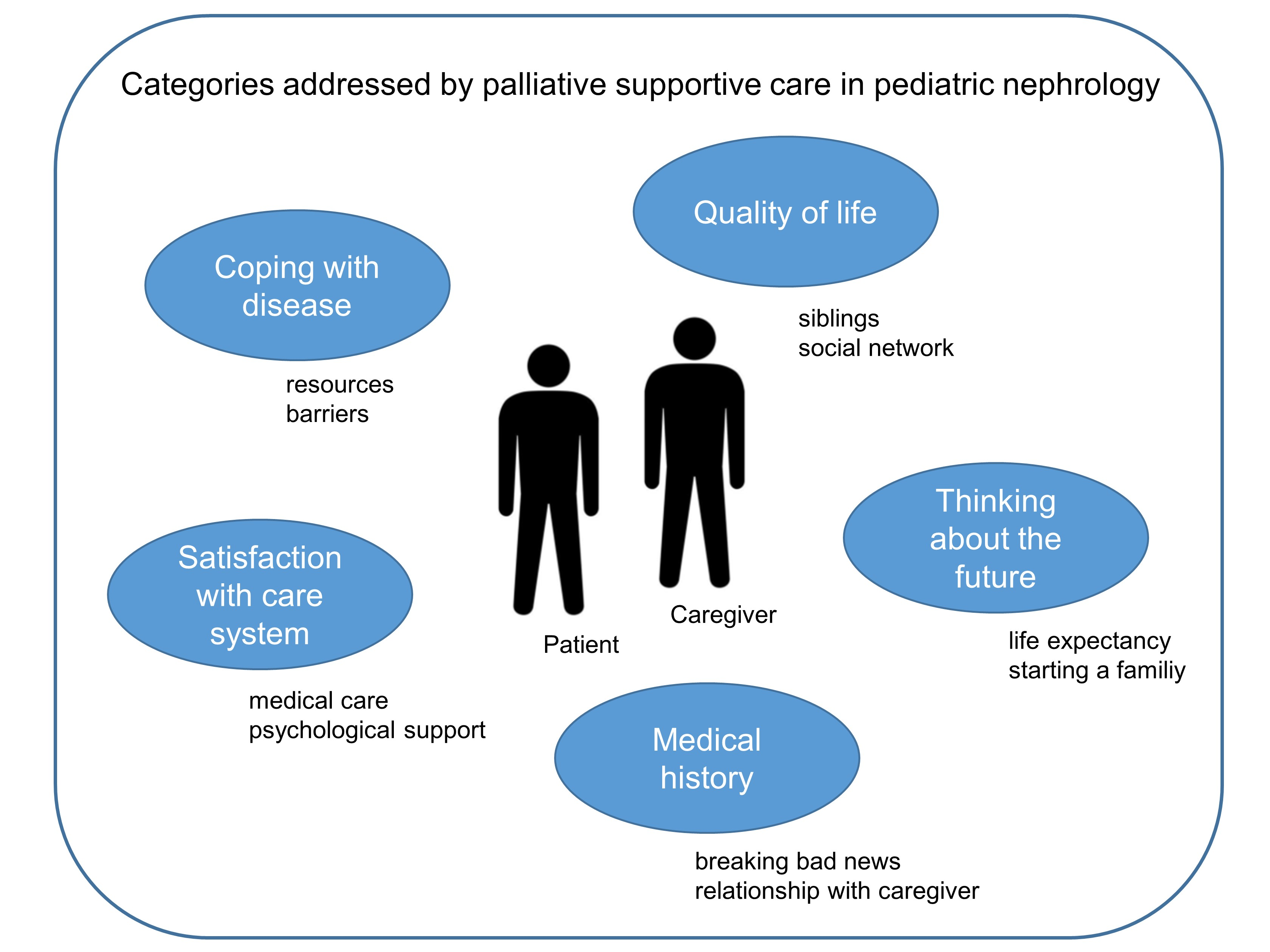
3.1. Main Categories
3.2. Caregivers’ View—Medical History (Breaking the Bad News)
“I just cried. I couldn’t take it at all that they told me, yes she has nephroblastoma [kidney tumor]. As if it wasn’t enough that she had a tumor, they said that not only one kidney, but the other one didn’t work neither, because the tumor was already on the other artery. And later it turned out that it was a de novo mutation, not inherited from the family. But to see this, this disease in your own child, yes, it’s hard.”(Female caregiver, 31 years, child transplanted)
“But, I have to say that the conversation was difficult. She told us the diagnosis, we asked how bad is it, and she immediately said: “Well, he is probably a transplant patient, a dialysis patient, you have to assume.” If you have never dealt with this before, of course, it is for you, as a parent, you think, you are scared to death.”(Female caregiver, 35 years, child on dialysis)
3.3. Patients’ View—Medical History (Family Support in Coping with Disease)
“Well, I grew up with four brothers and my parents, so to speak, six of them, and my dad was always the disease manager. He created the most blatant Excel tables with medications and always knew when we had to re-order medication. He did the dialysis until I was able to do it myself, so to speak. He also went on a school trip with me, […] and always came in the evening and took care of everything. He was a very close reference person for me. My mother was also always there, but took over less of the hospital things.”(Woman, 22 years, transplanted)
“So my mother studied biology and she knows the most about it and was able to fight for me the most when it came to things that happened in the hospital. And she usually went with me to the doctor, because her job makes her more flexible than my father, for example. He can’t just say, by the way, I’m not here for a few hours.”(Woman, 22 years, CKD stage 4)
3.4. Caregivers’ View—Quality of Life
“Our son had to take a back seat in many areas. When we were in hospital a lot, for example, and everything revolved around X (his sister). And of course that was awful for Y (our son), because he was also going through puberty. And then there are sometimes these sentences in retrospect: “You weren’t there.” But then we were always compensating either way. Either, we were in hospital, couldn’t work and had to compensate balance things at home. And that was quite difficult sometimes.”(Male caregiver, 53 years, child transplanted)
“But we are also lucky that, if necessary/ that we had our friends’ backs, that we were always able to solve it somehow.”(Male caregiver, 53 years, child transplanted)
3.5. Patients’ View—Quality of Life
“Well, what I am thinking is: there are always diseases worse than mine. So I am lucky. (…) I’m going to school and I’m doing eleventh grade and I would like to study pharmacy. (...) But, ‘cause of dialysis, I do not have that much time, so, hope I can do it. (...) Last school year, I only slept for about four or three hours per night because I missed so much and had to catch up on the material.”(Woman, 18 years, on dialysis)
“And then I made it to the job interview and then they somehow still didn’t want me. Once, because I still did not have a driver’s license and second because of my kidney disease. (...) Yes, I thought that was a bit mean somehow.“(Man, 21 years, CKD stage 4)
“(...) that it was difficult and uncomfortable for me to talk about it [catheter] when someone asked. During sports lessons and when changing or so (...) Then I told it to the people individually, but I didn’t really tell it in a big way, only to the closer people, so to speak.”(Boy, 16 years, transplanted)
“Beauty is, I think I am the most beautiful girl in the world, but, [patient and interviewer laugh] yes, my hand, where I was punctured, has really many scars and I don’t like that so much, yes. Still, I am not ashamed of it at all. Yes, and if someone asks me what it is, then I simply tell them what it is [fistula].”(Woman, 18 years, on dialyses)
“I think, I lost my–at the time–best friend also a little bit because of the disease. I think you also go through a bit of a personality change. However, I am actually quite happy about it, because, I think, it has changed a lot for the better in terms of personal development.”(Woman, 22 years, CKD stage 4)
“Yes, I have changed since dialysis. I actually became stronger and my personality, too, a lot has changed.”(Woman, 18 years, on dialyses)
“So far, I do not really have any problems with the disease. (...) I hardly notice the disease at all. Nothing hurts me or anything like this. I only notice that I am ill, because I have to go to the doctor all the time and because I have to take the medicines. It is just the knowledge that maybe in 10 or 20 years I may have to go on dialysis when my kidneys won’t work at all anymore. Otherwise, well, I actually live a very normal life.”(Man, 19 years, CKD stage 3)
3.6. Caregivers’ View—Thinking about the Future (Life Expectancy)
“[I worry about] dialysis or organ transplantation, whether it will all work out as one is hoping, so that it will be good for him [son] afterwards. And of course, this whole prognosis for him now in terms of life expectancy and so on [I’m also worried about that]. So, I just hope, I strongly hope for the research, that it will somehow progress further and further.”(Female caregiver, 37 years, child CKD stage 4)
“We used to have a relatively easy life. We did not have certain worries. Now we do occasionally have very big worries, especially when we do not know what is going to happen next. [...] And when you realize that your daughter’s life expectancy, for example, is considerably reduced and her quality of life is also limited, then you really worry.”(Male caregiver, 53 years, child transplanted)
3.7. Patients’ View—Thinking about the Future (Starting a Family)
“Otherwise, I would like to have children of my own, but I am also afraid that my kidney will deteriorate as a result. That the values will deteriorate. And I don’t think I could cope with that, because you never know whether another transplant will be possible, whether there will be an offer, whether it will be just as good.”(Woman, 22 years, transplanted)
“About family. I don’t know. I think patients try to suppress it a bit.”(Woman, 22 years, CKD stage 4)
3.8. Caregivers’ View—Satisfaction with Care System (Medical Care)
“I sometimes find it difficult when you are on the ward and always have a different contact person. Sometimes it’s an assistant doctor, sometimes it’s a senior doctor, sometimes it’s Dr. X”(Female caregiver, 35 years, CKD Stage 5).
3.9. Patients’ View—Satisfaction with Care System (Psychological Support)
“Probably it would have been good then too/ from today’s point of view I think it would have been good if you had somehow received psychological care (...) that you could somehow talk about how you feel (...) and come to terms with it, and also discuss it when people make comments.”(Woman, 22 years, CKD stage 4)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Topic 1 History of illness How long has your child been ill? When did you find out about it? Who told you about your child’s diagnosis? What was it like for you? What do you know about the disease? |
| Topic 2 Dealing with the disease Please describe a typical day/week... What is difficult in your situation? e.g., during the time of inpatient/ dialysis treatment, at home, at school, among friends, etc. What are you annoyed by? What do you manage well? Who do you turn to in case of difficulties? Do you know other children/adolescents who also suffer from kidney disease? How do the others deal with the disease? |
| Topic 3 Quality of life Would you tell me something about your child before he/she became ill? If necessary, ask about family, hobbies, everyday life, etc. What has changed since the illness? What is important to you now? What have you learned for yourself? |
| Topic 4 Ideas about the future Have you ever thought about your future or the future of your child? If necessary, inquiries about career, family, wishes |
| Topic 5 Satisfaction with the care Was there anything in the course of treatment so far where you thought: “That went really well now, that was particularly good”? Was there a situation where you would have liked support? Tell me more about these situations.... |
| Topic 6 Conclusion Are there still things that have not been addressed yet that are important to you? |
Appendix B
| Topic 1 History of illness Tell us about... Since when have you been ill? When did you find out about it? Who told you about it? What was it like for you? What do you know about your illness? Who in your family has been closest to you since the beginning of your illness? How is she/he coping with the disease? |
| Topic 2 Dealing with the disease Please describe a typical day/week... What is difficult in your situation? e.g., during the time of inpatient/ dialysis treatment, at home, at school, among friends, etc. What are you annoyed by? What works well for you? Who do you turn to in case of difficulties? Do you know children/adolescents who also suffer from kidney disease? Where from? Dialysis, summer camps, etc. How do the others deal with the disease? |
| Topic 3 Quality of life Would you tell me something about yourself before you became ill? If necessary, ask about family, hobbies, everyday life, etc. What has changed since the illness? What is important to you now? What have you learned for yourself? |
| Topic 4 Ideas about the future Have you ever thought about your future? If necessary, inquiries about job, family, wishes |
| Topic 5 Satisfaction with the care Was there anything in the course of treatment so far where you thought: “That went really well now, that was particularly good”? Was there a situation where you would have liked support? Tell me more about these situations.... |
| Topic 6 Conclusion Are there still things that have not been addressed yet that are important to you? |
References
- Splinter, A.; Tjaden, L.A.; Haverman, L.; Adams, B.; Collard, L.; Cransberg, K.; van Dyck, M.; Van Hoeck, K.J.; Hoppe, B.; Koster-Kamphuis, L.; et al. Children on dialysis as well as renal transplanted children report severely impaired health-related quality of life. Qual Life Res. 2018, 27, 1445–1454. [Google Scholar] [CrossRef]
- Moreira, J.M.; Bouissou Morais Soares, C.M.; Teixeira, A.L.; Simões e Silva, A.C.; Kummer, A.M. Anxiety, depression, resilience and quality of life in children and adolescents with pre-dialysis chronic kidney disease. Pediatr. Nephrol. 2015, 30, 2153–2162. [Google Scholar] [CrossRef]
- El Shafei, A.M.; Soliman Hegazy, I.; Fadel, F.I.; Nagy, E.M. Assessment of Quality of Life among Children with End-Stage Renal Disease: A Cross-Sectional Study. J. Environ. Public Health 2018, 2018, 8565498. [Google Scholar] [CrossRef]
- Steering Committee of the EAPC Task Force. IMPaCCT: Standards for paediatric palliative care in Europe. Eur. J. Palliat. Care 2007, 14, 109–114. [Google Scholar]
- Mack, J.W.; Wolfe, J. Early integration of pediatric palliative care: For some children, palliative care starts at diagnosis. Curr. Opin. Pediatr. 2006, 18, 10–14. [Google Scholar] [CrossRef]
- Neuburg, L. Early Initiation of Pediatric Palliative Care. J. Pediatr. Health Care 2021, 35, 114–119. [Google Scholar] [CrossRef]
- Lanini, I.; Samoni, S.; Husain-Syed, F.; Fabbri, S.; Canzani, F.; Messeri, A.; Mediati, R.D.; Ricci, Z.; Romagnoli, S.; Villa, G. Palliative Care for Patients with Kidney Disease. J. Clin. Med. 2022, 11, 3923. [Google Scholar] [CrossRef]
- Fowler, A.; Freiberger, D.; Moonan, M. Palliative and end-of-life care in pediatric solid organ transplantation. Pediatr. Transplant 2015, 19, 11–17. [Google Scholar] [CrossRef]
- House, T.R.; Wightman, A. Adding Life to Their Years: The Current State of Pediatric Palliative Care in CKD. Kidney360 2021, 2, 1063–1071. [Google Scholar] [CrossRef]
- Thumfart, J.; Reindl, T.; Rheinlaender, C.; Müller, D. Supportive palliative care should be integrated into routine care for paediatric patients with life-limiting kidney disease. Acta Paediatr. 2018, 107, 403–407. [Google Scholar] [CrossRef]
- Mitsnefes, M.M. Cardiovascular disease in children with chronic kidney disease. J. Am. Soc. Nephrol. 2012, 23, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Thumfart, J.; Bethe, D.; Wagner, S.; Pommer, W.; Rheinländer, C.; Müller, D. A survey demonstrates limited palliative care structures in paediatric nephrology from the perspective of a multidisciplinary healthcare team. Acta Paediatr. 2019, 108, 1350–1356. [Google Scholar] [CrossRef]
- Cornelia Helfferich. Die Qualität qualitativer Daten: Manual für die Durchführung qualitativer Interviews, 3rd ed.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2009. [Google Scholar]
- Philipp Mayring. Qualitative Inhaltsanalyse—Grundlagen und Techniken, 11th ed.; Beltz Pädagogik: Weinheim, Germany, 2010. [Google Scholar]
- Wightman, A.; Zimmerman, C.T.; Neul, S.; Lepere, K.; Cedars, K.; Opel, D. Caregiver Experience in Pediatric Dialysis. Pediatrics 2019, 143, e20182102. [Google Scholar] [CrossRef]
- Levy Erez, D.; Meyers, M.R.; Raman, S.; Thomas, M.; Furth, S.; Forrest, C.B.; Denburg, M. When Dialysis “Becomes Life”: Pediatric Caregivers’ Lived Experiences Obtained From Patient-Reported Outcomes Measures. Front. Pediatr. 2022, 10. Available online: https://www.frontiersin.org/article/10.3389/fped.2022.864134 (accessed on 20 June 2022). [CrossRef]
- Tong, A.; Lowe, A.; Sainsbury, P.; Craig, J.C. Parental perspectives on caring for a child with chronic kidney disease: An in-depth interview study. Child Care Health Dev. 2010, 36, 549–557. [Google Scholar] [CrossRef]
- Rana, P.; Mishra, D. Quality of life of unaffected siblings of children with chronic neurological disorders. Indian J. Pediatr. 2015, 82, 545–548. [Google Scholar] [CrossRef]
- Velasco, J.; Ferraris, J.R.; Eymann, A.; Ghezzi, L.F.R.; Coccia, P.A.; Ferraris, V. Health-related quality of life among siblings of kidney transplant recipients. Pediatr. Transplant 2020, 24, e13734. [Google Scholar] [CrossRef]
- Agerskov, H.; Thiesson, H.C.; Pedersen, B.D. Siblings of children with chronic kidney disease: A qualitative study of everyday life experiences. J. Ren. Care 2021, 47, 242–249. [Google Scholar] [CrossRef]
- Agerskov, H.; Thiesson, H.C.; Pedersen, B.D. The significance of relationships and dynamics in families with a child with end-stage kidney disease: A qualitative study. J. Clin. Nurs. 2020, 29, 987–995. [Google Scholar] [CrossRef]
- Kerklaan, J.; Hannan, E.; Hanson, C.; Guha, C.; Cho, Y.; Christian, M.; Hamiwka, L.; Ryan, J.; Sinha, A.; Wong, G.; et al. Perspectives on life participation by young adults with chronic kidney disease: An interview study. BMJ Open 2020, 10, e037840. [Google Scholar] [CrossRef]
- Clavé, S.; Tsimaratos, M.; Boucekine, M.; Ranchin, B.; Salomon, R.; Dunand, O.; Garnier, A.; Lahoche, A.; Fila, M.; Roussey, G.; et al. Quality of life in adolescents with chronic kidney disease who initiate haemodialysis treatment. BMC Nephrol. 2019, 20, 163. [Google Scholar] [CrossRef]
- Kubiak, N.; Jordans, I.; Müller, D. Kapitel 20—Chronische Niereninsuffizienz—Psychologische und sozialmedizinische Betreuung von Kindern und Jugendlichen. In Therapie-Handbuch—Nephrologie; Benzing, T., Ahrens, M., Benz, M., Bergmann, L., Bokemeyer, D., Brinkkötter, P., Ellinger, J., Fischereder, M., Floege, J., Grundmann, F., et al., Eds.; Urban & Fischer: Munich, Germany, 2022; pp. 150–153. [Google Scholar] [CrossRef]
| Caregiver (n = 10) | Patient (n = 5) | ||
|---|---|---|---|
| Sex | Female/male | 6/4 | 3/2 |
| Age | Median age [range] in years | 50,5 [29–54] | 19 [16–22] |
| Age of patient at the time of diagnosis | At time of birth <6 months ≥6 months | 3 3 4 | 2 3 0 |
| Stage of CKD | Stage 3–4 Stage ESKD Dialysis Transplantation | 4 1 5 | 2 1 2 |
| Marital status | Single Married Divorced | 0 9 1 | 5 0 0 |
| Citizenship | German Not German | 6 4 | 4 1 |
| Religion | Christian Muslim None | 2 3 5 | 0 1 4 |
| Place of residence | Berlin City Rural | 6 4 | 3 2 |
| Degree of disability of the patient | <50% ≥50% None | 0 9 1 | 1 4 0 |
| Care level of the patient | None Care level 1–2 * Care level 3–4 ** | 4 3 3 | 4 1 0 |
| Graduation of interview partner | Secondary school Middle school High school | 1 3 6 | 0 0 5 |
| Professional status of interview partner | Housewife/-man Education Academic education Unemployed Attending school | 2 3 4 1 0 | 0 1 2 0 2 |
| Monthly net income of interview partner | <EUR 1.000 EUR 1.000–3000 >EUR 3.000 No income | 4 2 4 0 | 2 0 0 3 |
| Main Categories | Subcategories |
|---|---|
| Medical History | Request for further medical information about disease Breaking bad news Transmitting diagnosis Family support in coping with disease |
| Coping with disease | Resources Barriers |
| Quality of life | Siblings Social relationship, peer group Research Free time Cosmetic changes in the body School/Education/Academic career Discipline dealing with disease Vacation/Holidays |
| Thinking about the future | Life as couple/starting a family Life expectancy |
| Satisfaction with care system | Language barriers Medical care Transition Psychological support Psychosocial care/advice |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubiak, N.; Fehrenbach, C.; Prüfe, J.; Thumfart, J. Do We Need Palliative Care in Pediatric Nephrology? Patients’ and Caregivers’ Disease Experience. Children 2023, 10, 324. https://doi.org/10.3390/children10020324
Kubiak N, Fehrenbach C, Prüfe J, Thumfart J. Do We Need Palliative Care in Pediatric Nephrology? Patients’ and Caregivers’ Disease Experience. Children. 2023; 10(2):324. https://doi.org/10.3390/children10020324
Chicago/Turabian StyleKubiak, Nina, Chiara Fehrenbach, Jenny Prüfe, and Julia Thumfart. 2023. "Do We Need Palliative Care in Pediatric Nephrology? Patients’ and Caregivers’ Disease Experience" Children 10, no. 2: 324. https://doi.org/10.3390/children10020324