
Efficacy and Safety of Elexacaftor-Tezacaftor-Ivacaftor in the Treatment of Cystic Fibrosis: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
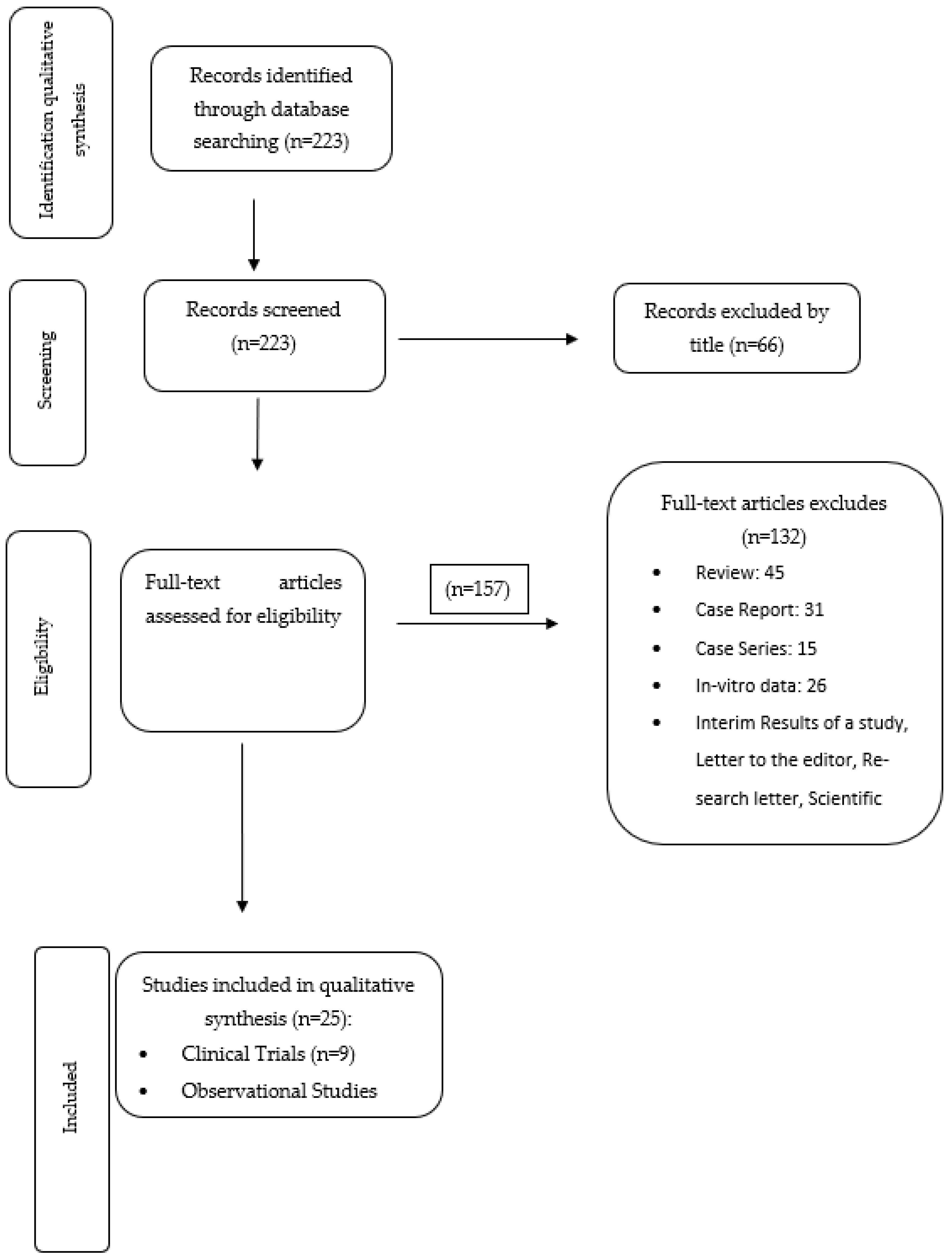
2.1. Literature Search, Eligibility Criteria and Study Selection
2.2. Study Selection
3. Results
3.1. Data from Case-Control Studies
3.1.1. Efficacy of Elexacaftor-Tezacaftor-Ivacaftor
3.1.2. Safety of Elexacaftor-Tezacaftor-Ivacaftor
3.2. Data Based on Observational Studies
3.2.1. Efficacy of Elexacaftor-Tezacaftor-Ivacaftor
- i.
- Cardiometabolic parameters
- ii.
- Glycemic status
3.2.2. Safety of Elexacaftor-Tezacaftor-Ivacaftor
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| 5-HT2c | 5-hydroxytryptamine2c |
| AE | Adverse Event |
| AG | Average Glucose |
| ALD | Advanced Lung Disease |
| ALP | Alkaline Phosphatase |
| ALT | Alanine Transaminase |
| AUC | Area Under the Curve |
| BMI | Body Mass Index |
| CF | Cystic Fibrosis |
| CFAbd-Score | Cystic Fibrosis Abdomen Score |
| CFQ-R RD | Cystic Fibrosis Questionnaire-Revised respiratory domain |
| CFRD | Cystic Fibrosis-related diabetes |
| CFTR | Cystic Fibrosis Transmembrane Conductance Regulator |
| CGM | Continuous Glucose Monitoring |
| CI | Confidence Interval |
| DA | Disorders of Appetite |
| DBM | Disorders of Bowel Movement |
| DBP | Diastolic Blood Pressure |
| DC | Derivative Control |
| DILI | Drug-induced liver injury |
| DIOS | Distal Intestinal Obstruction Syndrome |
| ELX/TEZ/IVA | Elexacaftor/Tezacaftor/Ivacaftor |
| ETI | Elexacaftor/Tezacaftor/Ivacaftor |
| FDA | Food and Drug Administration |
| FEV1 | Forced Expiratory Volume in the 1st second |
| FVC | Forced Vital Capacity |
| GERD | Gastro-esophageal Reflux Disease |
| HbA1c | Hemoglobin A1c |
| HC | Healthy Controls |
| HDL | High-Density Lipoprotein |
| ICP | Intracranial Pressure |
| IGT | Impaired Glucose Tolerance |
| INDET | Intermediate Glucose Tolerance |
| IQR | Interquartile range |
| IVA | Ivacaftor |
| LCI | Lung Clearance Index |
| LCI2.5 | Lung Clearance Index (lung volume turnover required to reach 2.5% of starting N2 concentration) |
| LDL | Low-Density Lipoprotein |
| LUM | Lumacaftor |
| MF | Minimal Function |
| mM | Millimolar (—mmol/lt) |
| NGT | Normal Glucose Tolerance |
| NIV | non-invasive Ventilation |
| OGTT | Oral Glucose Tolerance Test |
| PC | Proportional Control |
| PEx | pulmonary exacerbations |
| ppFEF25–75 | percent predicted forced mid-expiratory flow rate |
| ppFEV1 | percent predicted Forced Expiratory Volume in the first second |
| ppFVC | percent predicted Forced Vital Capacity |
| ppLCI | percent predicted Lung Clearance Index |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
| PwCF | People with Cystic Fibrosis |
| QoL | Quality of Life |
| RR | Rate Ratio |
| RV/TLC | Residual Volume/Total Lung Capacity |
| SBP | Systolic Blood Pressure |
| SC test | Sweat Chloride test |
| SCC | Sweat Chloride Concentration |
| TBIL | Total Bilirubin |
| VA | Alveolar Volume |
References
- Cystic Fibrosis Foundation Patient Registry. Annual Data Report 2021. Available online: https://www.cff.org/sites/default/files/2021-11/Patient-Registry-Annual-Data-Report.pdf (accessed on 6 January 2023).
- Bell, S.C.; Mall, M.A. The future of cystic fibrosis care: A global perspective. Lancet Respir. Med. 2020, 8, 65–124. [Google Scholar] [CrossRef] [PubMed]
- Elborn, J.S. Cystic fibrosis. Lancet 2016, 388, 2519–2531. [Google Scholar] [CrossRef] [PubMed]
- Bardin, E.; Pastor, A. Modulators of CFTR. Updates on clinical development and future directions. Eur. J. Med. Chem. 2021, 213, 113195. [Google Scholar] [CrossRef] [PubMed]
- De Boeck, K.; Amaral, M.D. Progress in therapies for cystic fibrosis. Lancet Respir. Med. 2016, 4, 662–674. [Google Scholar] [CrossRef]
- Middleton, P.G.; Taylor-Cousar, J.L. Development of elexacaftor-tezacaftor-ivacaftor: Highly effective CFTR modulation for the majority of people with cystic fibrosis. Expert Rev. Respir. Med. 2021, 15, 723–735. [Google Scholar] [CrossRef]
- Goetz, D.M.; Savant, A.P. Review of CFTR modulators 2020. Pediatr. Pulmonol. 2021, 56, 3595–3606. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Keating, D.; Gautham, M. VX-445-Tezacaftor-Ivacaftor in Patients with Cystic Fibrosis and One or Two Phe508del Alleles. N. Engl. J. Med. 2018, 379, 1612–1620. [Google Scholar] [CrossRef]
- Middleton, P.G.; Mall, M.A. Elexacaftor-Tezacaftor-Ivacaftor for Cystic Fibrosis with a Single Phe508del Allele. N. Engl. J. Med. 2019, 381, 1809–1819. [Google Scholar] [CrossRef] [PubMed]
- Heijerman, H.G.M.; McKone, E.F. Efficacy and safety of elexacaftor/tezacaftor/ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: A double-blind, randomised, phase 3 trial. Lancet 2019, 394, 1940–1948. [Google Scholar] [CrossRef]
- Sutharsan, S.; McKone, E.F. Efficacy and safety of elaxacaftor plus tezacaftor plus ivacaftor versus tezacaftor plus ivacaftor in people with cystic fibrosis homozygous for F508del-CFTR: A 24-week, multicenter, randomised, double-blind, active-controlled, phase 3b trial. Lancet Respir. Med. 2022, 10, 267–277. [Google Scholar] [CrossRef]
- Migliorisi, G.; Collura, M. Elexacaftor-Tezacaftor-Ivacaftor as a Final Frontier in the Treatment of Cystic Fibrosis: Definition of the Clinical and Microbiological Implications in a Case-Control Study. Pharmaceuticals 2022, 15, 606. [Google Scholar] [CrossRef]
- Barry, P.J.; Mall, M.A. Triple Therapy for Cystic Fibrosis Phe508del-Gating and Residual Function Genotypes. N. Engl. J. Med. 2021, 385, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Mall, M.A.; Brugha, R. Efficacy and Safety of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 Through 11 Years of Age with Cystic Fibrosis Heterozygous for F508del and a Minimal Function Mutation: A Phase 3B, Randomized, Placebo-Controlled Study. Am. J. Respir. Crit. Care Med. 2022, 206, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Mainz, J.G.; Zagoya, C. Elexacaftor-Tezacaftor-Ivacaftor Treatment in Cystic Fibrosis-Early results Obtained with the CF-Specific CFAbd-Score. Front. Pharmacol. 2022, 13, 877118. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.C.; Harris, L.M. The Rapid Reduction of Infection-Related Visits and Antibiotic Use Among People with Cystic Fibrosis After Starting Elexacaftor-Tezacaftor-Ivacaftor. Clin. Infect. Dis. 2022, 75, 1115–1122. [Google Scholar] [CrossRef]
- DiMango, E.; Spielman, D.B. Effect of highly effective modulator therapy on quality of life in adults with cystic fibrosis. Int. Forum Allergy Rhinol. 2021, 11, 75–78. [Google Scholar] [CrossRef]
- Nichols, D.P.; Paynter, A.C. Clinical Effectiveness of Elexacaftor/Tezacaftor/Ivacaftor in People with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2022, 205, 529–539. [Google Scholar] [CrossRef]
- Graeber, S.Y.; Vitzthum, C. Effects of Elexacaftor/Tezacaftor/Ivacaftor Therapy on CFTR Function in Patients with Cystic Fibrosis and One or Two F508del Alleles. Am. J. Respir. Crit. Care Med. 2022, 205, 540–549. [Google Scholar] [CrossRef]
- Graeber, S.Y.; Renz, D.M. Effects of Elexacaftor/Tezacaftor/Ivacaftor Therapy on Lung Clearance Index and Magnetic Resonance Imaging in Patients with Cystic Fibrosis and One or Two F508del Alleles. Am. J. Respir. Crit. Care Med. 2022, 206, 311–320. [Google Scholar] [CrossRef]
- Zemanick, E.T.; Taylor-Cousar, J.L. A phase 3 Open-Label Study of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 through 11 Years of Age with Cystic Fibrosis and at Least One F508del Allele. Am. J. Respir. Crit. Care Med. 2021, 203, 1522–1532. [Google Scholar] [CrossRef] [PubMed]
- Petersen, M.C.; Begnel, L. Effect of elexacftor-tezacaftor-ivacaftor on body weight and metabolic parameters in adults with cystic fibrosis. J. Cyst. Fibros. 2022, 21, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Korten, I.; Kieninger, E. Short-Term Effects of Elexacaftor/Tezacaftor/Ivacaftor Combination on Glucose Tolerance in Young People with Custic Fibrosis—An observational Pilot Study. Front. Pediatr. 2022, 10, 852551. [Google Scholar] [CrossRef] [PubMed]
- Scully, K.J.; Marchetti, P. The effect of elexacftor/tezacaftor/ivacaftor (ETI) on glycemia in adults with cystic fibrosis. J. Cyst. Fibros. 2022, 21, 258–263. [Google Scholar] [CrossRef]
- Piona, C.; Mozzillo, E. Impact of CFTR Modulators on Beta-Cell Function in Children and Young Adults with Cystic Fibrosis. J. Clin. Med. 2022, 11, 4149. [Google Scholar] [CrossRef] [PubMed]
- Stylemans, D.; Darquenne, C. Peripheral lung effect of elexacaftor/tezacaftor/ivacaftor in adult cystic fibrosis. J. Cyst. Fibros. 2022, 21, 160–163. [Google Scholar] [CrossRef]
- Bermingham, B.; Rueschhoff, A. Short-term effect of elexacaftor-tezacaftor-ivacaftor on lung function and transplant planning in cystic fibrosis patients with advanced lung disease. J. Cyst. Fibros. 2021, 20, 768–771. [Google Scholar] [CrossRef]
- Martin, C.; Burnet, E. Patient perspectives following initiation of elexacaftor-tezacaftor-ivacaftor in people with cystic fibrosis and advanced lung disease. Respir. Med. Res. 2021, 80, 100829. [Google Scholar] [CrossRef]
- Burgel, P.R.; Durieu, I. Rapid Improvement after Starting Elexacaftor-Tezacaftor-Ivacaftor in Patients with Cystic Fibrosis and Advanced Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 204, 64–73. [Google Scholar] [CrossRef]
- Carnovale, V.; Iacotucci, P. Effectiveness and safety of elexacaftor/tezacaftor/ivacaftor in patients with cystic fibrosis and advanced lung disease with Phe508del/minimal function genotype. Respir. Med. 2021, 189, 106646. [Google Scholar] [CrossRef]
- Salvatore, D.; Cimino, G. Elexacaftor/tezacaftor/ivacaftor in children aged 6-11 years with cystic fibrosis, at least one F508DEL allele, and advanced lung disease: A 24-week observational study. Pediatr. Pulmonol. 2022, 57, 2253–2256. [Google Scholar] [CrossRef] [PubMed]
- Carnovale, V.; Iacotucci, P. Elexacaftor/Tezacaftor/Ivacaftor in Patients with Cystic Fibrosis Homozygous for the F508del Mutation and Advanced Lung Disease: A 48-Week Observational Study. J. Clin. Med. 2022, 11, 1021. [Google Scholar] [CrossRef] [PubMed]
- Walter, E.; Bass, J. The Effect of Elexacaftor/Tezacaftor/Ivacaftor on Hospitalisations and Intravenous Antibiotic Use. Perm. J. 2022, 26, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Keogh, R.H.; Cosgriff, R. Projecting the impact of triple CFTR modulator therapy on intravenous antibiotic requirements in cystic fibrosis using patient registry data combined with treatments effects from randomized trials. Thorax 2022, 77, 873–881. [Google Scholar] [CrossRef]
- Merjaneh, L.; Hasan, S. The role of modulators in cystic fibrosis related diabetes. J. Clin. Transl. Endocrinol. 2022, 27, 100286. [Google Scholar] [CrossRef]
- Dagenais, R.V.E.; Su, V.C.H. Real-World Safety of CFTR Modulators in the Treatment of Cystic Fibrosis: A Systematic Review. J. Clin. Med. 2020, 10, 23. [Google Scholar] [CrossRef]
- Gramegna, A.; De Petro, C. Onset of systemic arterial hypertension after initiation of elexacftor/tezacaftor/ivacaftor in adults with cystic fibrosis: A case series. J. Cyst. Fibros. 2022, 21, 885–887. [Google Scholar] [CrossRef]
- Lieberman, J.; Rodbard, S. Low blood pressure in young adults with cystic fibrosis: An effect on chronic salt loss in sweat? Ann. Intern. Med. 1975, 82, 806–808. [Google Scholar] [CrossRef]
- Griese, M.; Costa, S. Safety and Efficacy of Elexacaftor/Tezacftor/Ivacaftor for 24 weeks or Longer in People with Cystic Fibrosis and One or More F508del Alleles: Interim Results of an Open-Label Phase 3 Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 203, 381–385. [Google Scholar] [CrossRef]
- Safirstein, J.; Grant, J.J. Biliary disease and cholocystectomy after initiation of elexacftor/ivacaftor/tezacaftor in adults with cystic fibrosis. J. Cyst. Fibros. 2021, 20, 506–510. [Google Scholar] [CrossRef]
- Assis, D.N.; Freedman, S.D. Gastointestinal disorders in cystic fibrosis. Clin. Chest. Med. 2016, 37, 109–118. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, K.M.; O’Carroll, O.M. The efficacy of Elexacaftor/Tezacaftor/Ivacaftor in patients with cystic fibrosis and advanced lung disease. Eur. Respir. J. 2021, 57, 2003079. [Google Scholar] [CrossRef] [PubMed]
- Rotolo, S.M.; Duehlmeyer, S. Testicular pain following initiation of elexacaftor/tezacaftor/ivacaftor in males with cystic fibrosis. J. Cyst. Fibros. 2020, 19, e39–e41. [Google Scholar] [CrossRef]
- Miller, M.J.; Foroozan, R. Papilledema and hypervitaminosis A after elexacaftor/tezacaftor/ivacaftor for cystic fibrosis. Can. J. Ophtalmol. 2022, 57, e6–e10. [Google Scholar] [CrossRef]
- Heo, S.; Young, D.C. Mental status changes during elexacaftor/tezacaftor/ivacaftor therapy. J. Cyst. Fibros. 2022, 21, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Tindel, W.; Su, A. Trikafta and Psychopathology in Cystic Fibrosis: A case Report. Psychosomatics 2020, 61, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Stylemans, D.; François, S. A case of self-limited drug induced liver injury under treatment with elexacaftor/tezacaftor/ivacaftor: When it is worth taking the risk. J. Cyst. Fibros. 2021, 20, 712–714. [Google Scholar] [CrossRef]
- Terlizzi, V.; Colangelo, C. Effectiveness of Elexacaftor/Tezacaftor/Ivacaftor in Three Subjects with the Cystic Fibrosis Genotype Phe508del/Unknown and Advanced Lung Disease. Genes 2021, 2, 1178. [Google Scholar] [CrossRef]
- Terlizzi, V.; Castaldo, G. Genotype–phenotype correlation and functional studies in patients with cystic fibrosis bearing CFTR complex alleles. J. Med. Genet. 2017, 54, 224–235. [Google Scholar] [CrossRef]
- Terlizzi, V.; Amato, F. Ex vivo model predicted in vivo efficacy of CFTR modulator therapy in a child with rare genotype. Mol. Genet. Genom. Med. 2021, 9, e1656. [Google Scholar] [CrossRef]
- Liu, Z.; Anderson, J.D. Human Nasal Epithelial Organoids for Therapeutic Development in Cystic Fibrosis. Genes 2020, 11, 603. [Google Scholar] [CrossRef] [PubMed]
- Berkers, G.; van Mourik, P. Rectal Organoids Enable Personalized Treatment of Cystic Fibrosis. Cell Rep. 2019, 26, 1701–1708.e3. [Google Scholar] [CrossRef] [PubMed]
- Gramegna, A.; Contarini, M. From Ivacaftor to Triple Combination: A Systematic Review of Efficacy and Safety of CFTR Modulators in People with Cystic Fibrosis. Int. J. Mol. Sci. 2020, 21, 5882. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Trial | Study Population | Intervention Analyzed | Primary Outcome |
|---|---|---|---|
|
Keating et al. (2018) Randomized, placebo–controlled, double-blind, phase 2 trial [9] | Phe508del heterozygous with a MF (n = 95) and Ph508del homozygous (n = 28), after a 4 week TEZ/IVA run in, aged ≥18 years | - Phe508del/MF (n = 21): VX-445 200 mg × 1 + TEZ 100 mg × 1 + IVA 150 mg × 2 daily - Phe508del/Phe508del (n = 21): VX-445 200 mg × 1 + TEZ 100 mg × 1 + IVA 150 mg × 2 daily | - Safety at 4 weeks: 92% of patients received VX-445 + TEZ + IVA had AE: 53% mild events, 43% moderate and 4% serious, 100% of patients received placebo had AE - FEV1 % (at 4 weeks): Phe508del/MF Increase in FEV1%: 13.8 points (95% CI 10.9–16.6) Phe508del/Phe508del Increase in FEV1: 11.0 points (95% CI 7.9–14.0) |
|
Middleton et al. (2019) Randomized, placebo–controlled, double-blind, phase 3 trial [10] | Phe508del heterozygous with a MF, aged ≥12 years, FEV1 40–90%, stable disease during the 4 week screening period before the beginning of the triple combination or the placebo (n = 403) | ELX 200 mg × 1 + TEZ 100 mg × 1 + IVA 150 mg × 2 daily (n = 200) | Increase in FEV1%: 13.8 points at 4 weeks (95% CI 12.4–15.4) |
|
Heijerman et al. (2019) Multi-centre, randomized, active-controlled, double-blind, phase 3 trial [11] | Phe508del homozygous, aged ≥12 years, FEV1 40–90% with stable disease, as judged by the investigators (n = 113) | ELX 200 mg × 1 + TEZ 100 mg × 1 + IVA 150 mg × 2 daily (n = 55) | Increase in FEV1% by 10 points (95% CI 7.4–12.6) at week 4 |
|
Barry et al. (2021) Phase 3, double-blind, randomized, active-controlled trial [14] | Phe508del/Gating mutation or Phe508del/ Residual mutation, aged ≥12 years (n = 258) | ELX 200 mg × 1 + TEZ 150 mg × 1 + IVA 150 mg × 2 daily (n = 132) | Change from baseline in FEV1% at week 8: 3.7 points (95% CI 2.8–4.6), higher by 3.5 points (95% CI 2.2–4.7) relative to active control |
|
Sutharsan et al. (2022) Multicentre, double-blind, active-controlled, phase 3b trial [12] | Phe508del homozygous, aged ≥12 years, FEV1% 40–90, with stable disease (n = 175) | ELX 200 mg × 1 + TEZ 100 mg × 1 + IVA 150 mg × 2 daily (n = 87) | Absolute change in CFQ-R RD from baseline at week 24: 17.1 (95% CI 14.1–20.1) |
|
Mainz et al. (2022) Prospective study [16] | Phe508del homozygous or heterozygous, aged ≥18 years (UK cohort) or ≥12 years (German cohort) (n = 152) | ELX/TEZ/IVA combination (n = 107): 60 PwCF under a different CFTR modulator before 47 PwCF without previous treatment | Decrease in total CFAbd-Score at week 24 by 29% during treatment (p < 0.01) |
|
Miller et al. (2022) Case-crossover analysis [17] | PwCF who were treated by ELX/TEZ/IVA before 1/12/2019 (n = 778) | ELX/TEZ/IVA (n = 389) | - Change in days with a health care visit: −2.5 (95% CI −3.31, −1.7) - Change in inpatients visits: −0.16 (95% CI −2.2, −1) - Decrease in days with an infection-related visit: −0.62 (−0.93, −0.31) - Decrease in distinct antibiotics prescribe: −0.78 (−1.03, −0.54) |
|
Mall et al. (2022) Phase 3b, randomized, double blind, placebo-controlled study [15] | Phe508del heterozygous with a MF, aged 6–11 years (n = 121) | - Children < 30 kg: ELX 100 mg × 1 + TEZ 50 mg × 1 + IVA 75 mg × 2 daily - Children ≥ 30 kg: ELX 200 mg × 1 + TEZ 100 mg × 1 + IVA 150 mg × 2 daily (n = 60) | Decrease in LCI2.5 from baseline at week 24: 2.29 units (95% CI 1.97–2.6) and between groups difference −2.26 (95% CI −2.71 to −1.81) |
|
Migliorisi et al. (2022) Case-control study [13] | PwCF with at least one Phe508del mutation and severe pulmonary disease (ppFEV1 < 40%) (n = 26) | ELX/TEZ/IVA | - Increase 10–15 points in ppFEV1 in treated patients - Amelioration in radiological findings - Increase in BMI of treated patients - 77% of case group patients presented a decrease in sweat chloride concentration - Increase in CFQ-R score in 100% of in case group patients - P. aerigunosa was detected in sputum of treated patients vs S. aureus in samples of the control group - Reduction in pulmonary exacerbations (p < 0.05) after 1 year of ETI treatment in case group patients |
| Study | Study Population | Primary Outcomes |
|---|---|---|
|
DiMango et al. (2020) Prospective Cohort Study [18] | -Adults with CF with at least one copy of Phe508del mutation (n = 43) | - BMI improvement from 21.8 to 22.7 (p = 0.000002) - Increase in ppFEV1 from 65% to 76% (p = 0.0000005) - Improvement of all domains of CFQ-R |
|
Stylemans et al. (2021) Real-life follow-up study [27] | -PwCF aged ≥18 years -Genotype Ph508del/Phe508del or Phe508del/MF -Severe lung disease and ppFEV1 < 30% for Phe508del/Phe508del genotype and <40% for Phe508del/MF genotype (n = 14) | - Increase in ppFEV1 by 12% at week 4 (p < 0.001) - Decrease in ppLCI by 31% from baseline at week 4 (p < 0.002) - Decrease in acinar Ventilation heterogeneity by 411% predicted at week 4 (p < 0.001) - Improvements in RV/TLC ratio to 0.49 % from 0.58% at week 4 (p < 0.001) - Increase in ppFVC by 13 points at 1 month (p < 0.001) - Increase in VA to 4.14 lt from 3.64 lt at week 4 (p < 0.001) - Diminished exacerbation rate to 0.07/month from baseline at 3 months |
|
Bermingham et al. (2021) Retrospective cohort study [28] | PwCF aged >18 years with advanced lung disease (n = 50) | - Increase in ppFEV1 of 7.9 points (95% CI 5.85–10.2) - Increase in ppFVC of 10.5 points (95% CI 7.76–13.48) - Fewer patients needed lung transplant planning |
| Martin et al. (2021) [29] | PwCF aged ≥ 12 years with advanced lung disease (ppFEV1 < 40% and/or indication for lung transplantation) (n = 110) | - Reduction of respiratory symptoms (cough, pulmonary exacerbations) - Improvement of appetite and sleep - Increase in gastrointestinal symptoms - Less time needed for other kinds of treatments (ex. chest physiotherapy) - Diminished use of antibiotics and less admissions in hospitals - Suspension from lung transplantation list - Amelioration of body self-esteem, self-confidence and autonomy |
|
Burgel et al. (2021) Prospective Observational cohort study [30] | PwCF ≥12 years old, with at least one Phe508del mutation and advanced lung disease (ppFEV1 < 40 and/or under evaluation for transplantation (n = 245) | At 3 months: - Increase in ppFEV1 by 15.1 points (95% CI 13.8–16.4) - Increase in ppFEV1 by 16.2 (95% CI 14.5–17.9) for PwCF not treated with O2 or NIV - Increase in ppFEV1 by 13.6 points (95% CI 11.6–15.7) for those without O2 or NIV - Mean increase in BMI 4.2 kg (95% CI 4.1–4.9) - 50% reduction in O2 requirements (p < 0.001) - 30% decrease in NIV use (p < 0.001) - 50% decrease in enteral tube feeding (p < 0.001) - 2 out of 16 received a transplant
|
|
Zemanick et al. (2021) Phase 3, two-part, open-label, multicenter trial [22] | Children 6–11 years old with Phe508del/MF genotype or Phe508del homozygous (n = 66) | - 98.5% of children presented AE, 54.5% of which were mild and 42.4% moderate - PK: 30 kg is the weight limit for the administration of the full adult daily dose of ETI instead of the 50% of it - Through week 24:
|
|
Scully et al. (2021) Prospective single-center Observational study [25] | PwCF aged >18 years Phe508del heterozygous and with or without CFRD (n = 23) | - Decrease in AG (p < 0.018), SD (p < 0.001), % time Gly > 200 mg/dL (p < 0.006), peak sensor value (p < 0.45) - Increase in %time Gly 70–180 mg/dl (p < 0.04) |
|
Carnovale et al. (2021) Retrospective Cohort Study [31] | PwCF aged >12 years with Phe508del/MF genotype and advanced lung disease (n = 47) | Increase 10.69% (95% CI 8.05–13.33) in ppFEV1 at week 4 and 14.16 points (95% CI 11.43–16.89) at week 24 |
|
Nichols et al. (2021) PROMISE STUDY Prospective Observational Study [19] | PwCF ≥ 12 years old with at least one copy of Phe508del At baseline 238 were on no CFTR treatment, 34 were on IVA and 215 on a two-drug modulator use (LUM/IVA or TEZ/IVA) (n = 487) | At 6 months: - Average increase in ppFEV1 by 9.8 points (95% CI 8.8–10.8) - Average decrease in SCC by 41.7 mmol/lt (95% CI −43.8, −39.6) - Increase in CFQ-R RD score by a mean of 20.4 points - Mean increase in BMI of 1.2 kg/m2 in adults and 0.3 z-score in children |
|
Petersen et al. (2021) Single-center, retrospective, observation study [23] | Adults with CF, Phe508del heterozygous (pregnant and lung transplant patients the previous year or since starting the treatment were excluded) (n = 134) | - Increase in annualized difference in BMI by 1.47 kg/m2/year (95% CI 1.08–1.87) - Increase in annualized difference in weight by 4.55 kg/year (95% CI 3.14–5.36) - Increase in SBP by 4.94 mmHg/year (95% CI 0.31–9.57) - Increase in DBP by 3.49 mmHg per year (95% CI 0.31–9.57) - Decrease in protein gap by 5.84 g/L/year (95% CI −4.67 to −7.04) - In PWCF without CFRD: Decrease in annualized rate of random blood Gly by 0.78 mM/year (95%CI −0.23 to −1.33) Decrease in annualized rate of HbA1c by 0.16%/year (95% CI −0.07 to −0.26) - In PwCF with CFRD: Increase in total cholesterol by 0.67 mM/year (95% CI 0.37–0.97) Increase in LDL by 0.47 mM/year (95% CI 0.25–0.69) Increase in HDL by 0.23 mM/year (95%CI 0.04–0.42) |
|
Salvatore et al. (2022) A 24-week Retrospective Observational Study [32] | Children aged 6–11 years with Phe508del/Phe508del or Phe508del/MF genotypes, and ppFEV1 < 40% (n = 9) | 22.4 points increase in ppFEV1 at week 24 (95% CI 15.22–29.52) |
|
Carnovale et al. (2022) A 48-week Retrospective Observational Study [33] | PwCF aged ≥ 6 years, Phe508del homozygous with LUM/IVA or TEZ/IVA treatment for at least 6 months and severe lung disease (n = 26) | - Increase in ppFEV1% from baseline by 12.06 points (95% CI 9.47–16.98) at week 4, by 13.22 points (95% CI 9.47–16.98) at week 12, by 15.32 points (95% CI 11.3–19.34) at week 24 and by 14.48 points (95% CI 10.64–18.32) at week 48 - Increase in ppFVC% from baseline by 13.08 points (95%CI 8.54–17.62) at week 4, by 14.59 points (95%CI 9.69–19.49) at week 8, by 18.89 points (95% CI 14.20–23.59) at week 24 and by 18.50 points (95% CI 13.64–23.35) at week 48 |
|
Graeber et al. (2022) Prospective Multicenter Observational Study [20] | PwCF ≥ 12 years old Phe508del homozygous or Phe508del/MF with no previous exposure to ELX/TEZ/IVA (n = 107) | Phe508del/MF:
|
|
Korten et al. (2022) Observation Pilot Study [24] | PwCF ≥ 12 years old with at least one copy of Phe508del mutation and with no CFRD (n = 16) | - OGTT improved after treatment (p < 0.02): 7 patients improved in OGTT 5 had a normal result 2 remained stable 1 changed from indeterminate glucose tolerance to impaired glucose tolerance - Improvement in plasma Gly levels at 60, 90 and 120 min (p < 0.03, p < 0.04, p < 0.03 respectively) - Lower insulin levels at 120 and 180 min (p < 0.01, p< 0.006 respectively) - Lower C-peptide levels at 120 and 180 min (p < 0.08 and p < 0.005 respectively) - HbA1c values were stable - Mean, minimum, maximum Gly levels and percentage of Gly level time appeared no difference after treatment |
| Piona et al. (2022) Prospective Observational Study [26] | PwCF ≥ 6 years old with at least one Phe508del mutation (n = 21) | 12–18 months after treatment with ELX/TEZ/IVA: - No difference in glucose tolerance, beta-cell function, insulin clearance and insulin sensitivity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapouni, N.; Moustaki, M.; Douros, K.; Loukou, I. Efficacy and Safety of Elexacaftor-Tezacaftor-Ivacaftor in the Treatment of Cystic Fibrosis: A Systematic Review. Children 2023, 10, 554. https://doi.org/10.3390/children10030554
Kapouni N, Moustaki M, Douros K, Loukou I. Efficacy and Safety of Elexacaftor-Tezacaftor-Ivacaftor in the Treatment of Cystic Fibrosis: A Systematic Review. Children. 2023; 10(3):554. https://doi.org/10.3390/children10030554
Chicago/Turabian StyleKapouni, Nikoletta, Maria Moustaki, Konstantinos Douros, and Ioanna Loukou. 2023. "Efficacy and Safety of Elexacaftor-Tezacaftor-Ivacaftor in the Treatment of Cystic Fibrosis: A Systematic Review" Children 10, no. 3: 554. https://doi.org/10.3390/children10030554
APA StyleKapouni, N., Moustaki, M., Douros, K., & Loukou, I. (2023). Efficacy and Safety of Elexacaftor-Tezacaftor-Ivacaftor in the Treatment of Cystic Fibrosis: A Systematic Review. Children, 10(3), 554. https://doi.org/10.3390/children10030554