
Emotional Regulation Interventions on Developmental Course for Preterm Children: A Systematic Review of Randomized Control Trials


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
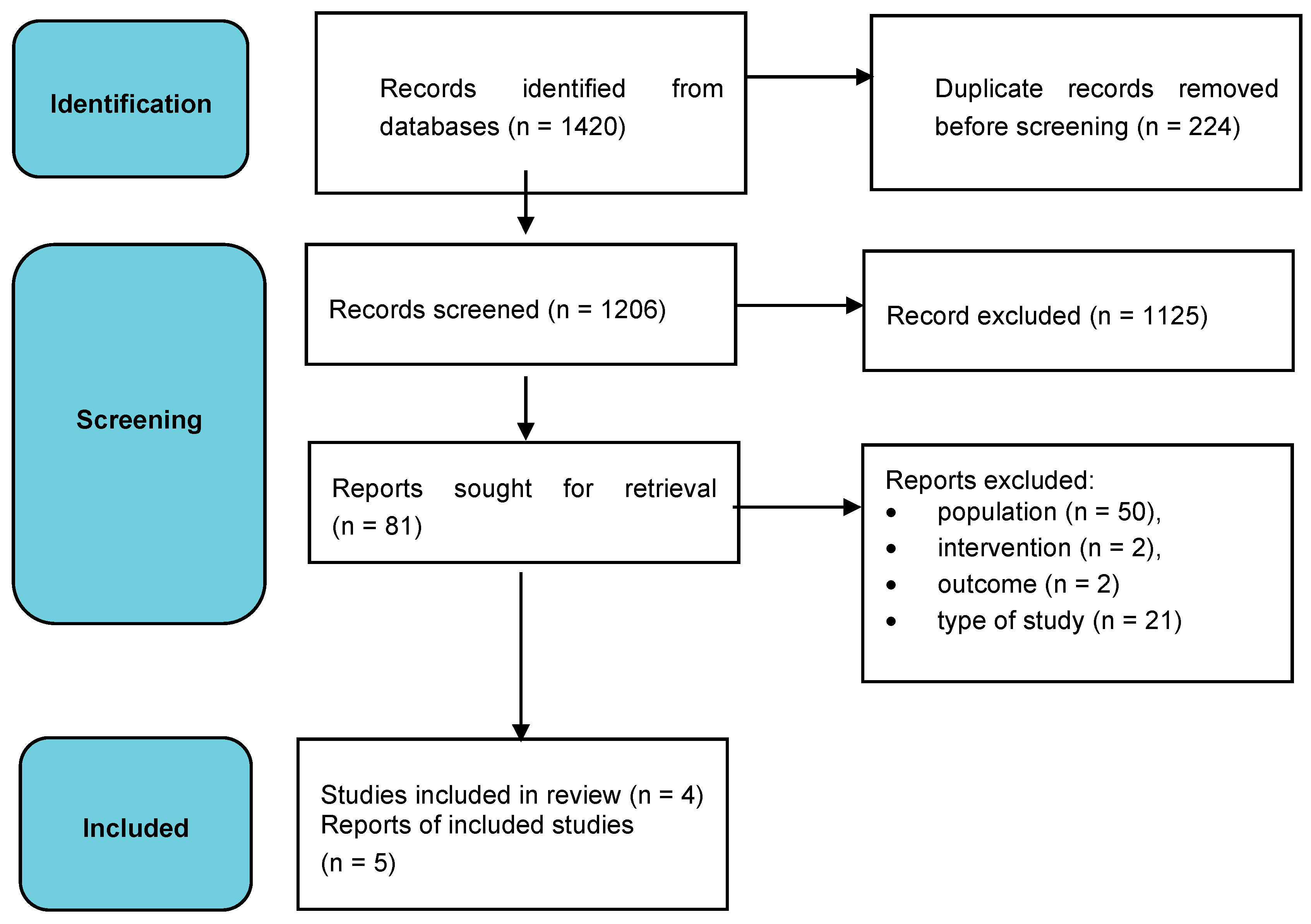
2.2. Study Selection and Data Collection Process
2.3. Risk of Bias
3. Results
3.1. Group Physiotherapy Intervention
3.2. Computerized Intervention in Executive Functions
3.3. Parent Training
3.4. Mindfulness Intervention
3.5. Methodological Quality and Risk of Bias
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Saigal, S.; Doyle, L. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef]
- Voigt, B.; Pietz, J.; Pauen, S.; Kliegel, M.; Reuner, G. Cognitive development in very vs. moderately to late preterm and full-term children: Can effortful control account for group differences in toddlerhood? Early Hum. Dev. 2012, 88, 307–313. [Google Scholar] [CrossRef]
- WHO. Preterm Birth Fact Sheet. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 7 September 2022).
- Glass, H.C.; Costarino, A.T.; Stayer, S.A.; Brett, C.M.; Cladis, F.; Davis, P.J. Outcomes for Extremely Premature Infants. Anesth. Analg. 2015, 120, 1337–1351. [Google Scholar] [CrossRef]
- Hintz, S.R.; Vohr, B.R.; Bann, C.M.; Taylor, H.G.; Das, A.; Gustafson, K.E.; Yolton, K.; Watson, V.E.; Lowe, J.; DeAnda, M.E.; et al. Preterm Neuroimaging and School-Age Cognitive Outcomes. Pediatrics 2018, 142, e20174058. [Google Scholar] [CrossRef] [PubMed]
- Luu, T.M.; Rehman Mian, M.O.; Nuyt, A.M. Long-Term Impact of Preterm Birth. Clin. Perinatol. 2017, 44, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, L.; Burnett, A.C.; Anderson, P.J. Cognitive and academic outcomes of children born extremely preterm. Semin. Perinatol. 2021, 45, 151480. [Google Scholar] [CrossRef] [PubMed]
- Cassiano, R.G.M.; Gaspardo, C.M.; Linhares, M.B.M. Prematurity, neonatal health status, and later child behavioral/emotional problems: A systematic review. Infant Ment. Health J. 2016, 37, 274–288. [Google Scholar] [CrossRef]
- Peralta-Carcelen, M.; Schwartz, J.; Carcelen, A.C. Behavioral and Socioemotional Development in Preterm Children. Clin. Perinatol. 2018, 45, 529–546. [Google Scholar] [CrossRef]
- Peralta-Carcelen, M.; Carlo, W.A.; Pappas, A. Behavioral problems and socioemotional competence at 18 to 22 months of extremely premature children. Pediatrics 2017, 139, e20161043. [Google Scholar] [CrossRef]
- Denham, S.A.; Blair, K.A.; DeMulder, E.; Levitas, J.; Sawyer, K.; Auerbach-Major, S.; Queenan, P. Preschool Emotional Competence: Pathway to Social Competence? Child Dev. 2003, 74, 238–256. [Google Scholar] [CrossRef]
- Clark, C.A.C.; Woodward, L.J.; Horwood, L.J.; Moor, S. Development of Emotional and Behavioral Regulation in Children Born Extremely Preterm and Very Preterm: Biological and Social Influences. Child Dev. 2008, 79, 1444–1462. [Google Scholar] [CrossRef]
- Cole, P.M.; Michel, M.K.; Teti, L.O. The development of emotion regulation and dysregulation: A clinical perspective. Monogr. Sociaty Res. Child Dev. 1994, 59, 73–100. [Google Scholar] [CrossRef]
- Als, H.; Duffy, F.H.; McAnulty, G.B.; Rivkin, M.J.; Vajapeyam, S.; Mulkern, R.V.; Warfield, S.K.; Huppi, P.S.; Butler, S.C.; Conneman, N.; et al. Early Experience Alters Brain Function and Structure. Pediatrics 2004, 113, 846–857. [Google Scholar] [CrossRef]
- Ionio, C.; Lista, G.; Veggiotti, P.; Colombo, C.; Ciuffo, G.; Daniele, I.; Landoni, M.; Scelsa, B.; Alfei, E.; Bova, S. Cognitive, Behavioral and Socioemotional Development in a Cohort of Preterm Infants at School Age: A Cross-Sectional Study. Pediatr. Rep. 2022, 14, 115–126. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.E.; Hofheimer, J.A.; O’Shea, M.; Kilbride, H.; Carter, B.S.; Check, J.; Helderman, J.; Neal, C.R.; Pastyrnak, S.; Smith, L.M.; et al. Analysis of Neonatal Neurobehavior and Developmental Outcomes Among Preterm Infants. JAMA 2022, 5, e2222249. [Google Scholar] [CrossRef] [PubMed]
- Kvanta, H.; Bolk, J.; Strindberg, M.; Jiménez-Espinoza, C.; Broström, L.; Padilla, N.; Ådén, U. Exploring the distribution of grey and white matter brain volumes in extremely preterm children, using magnetic resonance imaging at term age and at 10 years of age. PLoS ONE 2021, 16, e0259717. [Google Scholar] [CrossRef]
- Montagna, A.; Nosarti, C. Socio-Emotional Development Following Very Preterm Birth: Pathways to Psychopathology. Front. Psychol. 2016, 7, 80. [Google Scholar] [CrossRef]
- Neubauer, A.; Menegaux, A.; Wendt, J.; Li, H.B.; Schmitz-Koep, B.; Ruzok, T.; Thalhammer, M.; Schinz, D.; Bartmann, P.; Wolke, D.; et al. Aberrant claustrum structure in preterm-born neonates: An MRI study. Neuroimage Clin. 2022, 8, 103286. [Google Scholar] [CrossRef]
- Ganella, E.P.; Burnett, A.; Cheong, J.; Thompson, D.; Roberts, G.; Wood, S. Abnormalities in orbitofrontal cortex gyrification and mental health outcomes in adolescents born extremely preterm and/or at an extremely low birth weight. Hum. Brain Mapp. 2014, 36, 1138–1150. [Google Scholar] [CrossRef]
- Mossad, S.I.; Muscat, C.; Pang, E.W.; Taylor, M. Emerging atypical connectivity networks for processing angry and fearful faces in very preterm born children. Hum. Brain Mapp. 2020, 41, 3794–3806. [Google Scholar] [CrossRef]
- Pavlova, M.A.; Galli, J.; Zanetti, F.; Pagani, F.; Micheletti, S.; Rossi, A.; Fazzi, E.M. Social cognition in individuals born preterm. Sci. Rep. 2021, 11, 14448. [Google Scholar] [CrossRef] [PubMed]
- Peterson, B.S. Regional Brain Volume Abnormalities and Long-term Cognitive Outcome in Preterm Infants. JAMA 2000, 284, 1939. [Google Scholar] [CrossRef]
- Schmitz-Koep, B.; Zimmermann, J.; Menegaux, A.; Nuttall, R.; Bäuml, J.G.; Schneider, S.C.; Sorg, C. Within amygdala: Basolateral parts are selectively impaired in premature-born adults. NeuroImage Clin. 2021, 31, 102780. [Google Scholar] [CrossRef]
- Sato, J.; Safar, K.; Vandewouw, M.M.; Bando, N.; O’Connor, D.L.; Unger, S.L.; Taylor, M.J. Altered functional connectivity during face processing in children born with very low birth weight. Soc. Cogn. Affect. Neurosci. 2021, 16, 1182–1190. [Google Scholar] [CrossRef] [PubMed]
- Nosarti, C.; Giouroukou, E.; Healy, E.; Rifkin, L.; Walshe, M.; Reichenberg, A.; Murray, R.M. Grey and white matter distribution in very preterm adolescents mediates neurodevelopmental outcome. Brain 2007, 131, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Gousias, I.S.; Edwards, A.D.; Rutherford, M.A.; Counsell, S.J.; Hajnal, J.V.; Rueckert, D.; Hammers, A. Magnetic resonance imaging of the newborn brain: Manual segmentation of labelled atlases in term-born and preterm infants. NeuroImage 2012, 62, 1499–1509. [Google Scholar] [CrossRef]
- Aanes, S.; Bjuland, K.J.; Skranes, J.; Løhaugen, G.C.C. Memory function and hippocampal volumes in preterm born very-low-birth-weight (VLBW) young adults. NeuroImage 2015, 105, 76–83. [Google Scholar] [CrossRef]
- Omizzolo, C.; Scratch, S.E.; Stargatt, R.; Kidokoro, H.; Thompson, D.K.; Lee, K.J.; Anderson, P.J. Neonatal brain abnormalities and memory and learning outcomes at 7 years in children born very preterm. Memory 2013, 22, 605–615. [Google Scholar] [CrossRef]
- Rogers, C.E.; Anderson, P.J.; Thompson, D.K.; Kidokoro, H.; Wallendorf, M.; Treyvaud, K.; Inder, T.E. Regional Cerebral Development at Term Relates to School-Age Social–Emotional Development in Very Preterm Children. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 181–191. [Google Scholar] [CrossRef]
- Nosarti, C.; Froudist-Walsh, S. Alterations in development of hippocampal and cortical memory mechanisms following very preterm birth. Dev. Med. Child. Neurol. 2016, 4, 35–45. [Google Scholar] [CrossRef]
- Williamson, K.E.; Jakobson, L.S. Social attribution skills of children born preterm at very low birth weight. Dev. Psychopathol. 2014, 26 Pt 1, 889–900. [Google Scholar] [CrossRef]
- Healy, E.; Reichenberg, A.; Nam, K.W.; Allin, M.P.; Walshe, M.; Rifkin, L.; Murray, S.R.M.; Nosarti, C. Preterm Birth and Adolescent Social Functioning–Alterations in Emotion-Processing Brain Areas. J. Pediatr. 2013, 163, 1596–1604. [Google Scholar] [CrossRef] [PubMed]
- Mossad, S.I.; Vandewouw, M.M.; Smith, M.L.; Taylor, M.J. The preterm social brain: Altered functional networks for Theory of Mind in very preterm children. Brain Commun. 2021, 3, fcaa237. [Google Scholar] [CrossRef]
- Arpi, E.; Ferrari, F. Preterm birth and behaviour problems in infants and preschool-age children: A review of the recent literature. Dev. Med. Child Neurol. 2013, 55, 788–796. [Google Scholar] [CrossRef]
- Cheong, J.L.; Doyle, L.W.; Burnett, A.C.; Lee, K.J.; Walsh, J.M.; Potter, C.R.; Spittle, A.J. Association Between Moderate and Late Preterm Birth and Neurodevelopment and Social-Emotional Development at Age 2 Years. JAMA Pediatr. 2017, 171, e164805. [Google Scholar] [CrossRef]
- Johnson, S.; Marlow, N. Preterm Birth and Childhood Psychiatric Disorders. Pediatr. Res. 2011, 69 Pt 2, 11R–18R. [Google Scholar] [CrossRef]
- Spittle, A.J.; Treyvaud, K.; Doyle, L.W.; Roberts, G.; Lee, K.J.; Inder, T.E.; Anderson, P.J. Early Emergence of Behavior and Social-Emotional Problems in Very Preterm Infants. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 909–918. [Google Scholar] [CrossRef]
- Fitzallen, G.C.; Sagar, Y.K.; Taylor, H.G.; Bora, S. Anxiety and Depressive Disorders in Children Born Preterm: A Meta-Analysis. J. Dev. Behav. Pediatr. 2021, 42, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Mathewson, K.J.; Chow, C.H.T.; Dobson, K.G.; Pope, E.I.; Schmidt, L.A.; Van Lieshout, R.J. Mental health of extremely low birth weight survivors: A systematic review and meta-analysis. Psychol. Bull. 2017, 143, 347–383. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.G. Neurodevelopmental origins of social competence in very preterm children. Semin. Fetal Neonatal Med. 2020, 25, 101108. [Google Scholar] [CrossRef]
- Potijk, M.R.; de Winter, A.F.; Bos, A.F.; Kerstjens, J.M.; Reijneveld, S.A. Co-occurrence of developmental and behavioural problems in moderate to late preterm-born children. Arch. Dis. Child. 2015, 101, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R. The Development of Regulatory Functions from Birth to 5 Years: Insights from Premature Infants. Child Dev. 2009, 80, 544–561. [Google Scholar] [CrossRef] [PubMed]
- Vinall, J.; Miller, S.P.; Synnes, A.R.; Grunau, R.E. Parent behaviors moderate the relationship between neonatal pain and internalizing behaviors at 18 months corrected age in children born very prematurely. Pain 2013, 154, 1831–1839. [Google Scholar] [CrossRef]
- Zmyj, N.; Witt, S.; Weitkämper, A.; Neumann, H.; Lücke, T. Social Cognition in Children Born Preterm: A Perspective on Future Research Directions. Front. Psychol. 2017, 8, 455. [Google Scholar] [CrossRef] [PubMed]
- Tofani, M.; Mustari, M.; Tiozzo, E.; Dall’Oglio, I.; Morelli, D.; Gawronsky, O.; Salata, M.; Cantonetti, L.; Castelli, E.; Di Lallo, D.; et al. The development of the International Classification of Functioning, Disability and Health for Child and Youth (ICF-CY) Core Sets: A systematic review. Disabil. Rehabil. 2022, 1–10. [Google Scholar] [CrossRef]
- Cheol Chang, M. Pediatric Physical Medicine and Rehabilitation. Children 2022, 9, 954. [Google Scholar] [CrossRef]
- Hsu, N.; Monasterio, E.; Rolin, O. Telehealth in Pediatric Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2021, 32, 307–317. [Google Scholar] [CrossRef]
- Ekhtiari, H.; Rezapour, T.; Aupperle, R.L.; Paulus, M.P. Neuroscience-informed psychoeducation for addiction medicine: A neurocognitive perspective. Prog Brain Res. 2017, 235, 239–264. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Galeoto, G.; Berardi, A.; De Santis, R.; Di Valentini, L.; Beccasio, R.; Marquez, M.A.; Tofani, M. Validation and cross-cultural adaptation of the Van Lieshout test in an Italian population with cervical spinal cord injury: A psychometric study. Spinal Cord Ser. Cases 2018, 4, 49. [Google Scholar] [CrossRef]
- Fabbri, B.; Berardi, A.; Tofani, M.; Panuccio, F.; Ruotolo, I.; Sellitto, G.; Galeoto, G. A systematic review of the psychometric properties of the Jebsen–Taylor Hand Function Test (JTHFT). Hand Surg. Rehabil. 2021, 40, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Berardi, A.; Panuccio, F.; Pilli, L.; Tofani, M.; Valente, D.; Galeoto, G. Evaluation instruments for executive functions in children and adolescents: A systematic review. Expert Rev. Pharm. Outcomes Res. 2021, 21, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Tofani, M.; Blasetti, G.; Lucibello, L.; Berardi, A.; Galeoto, G.; Sabbadini, M.; Santecchia, L.; Castelli, E. An Italian Validation of ABILHAND-Kids for Children with Cerebral Palsy. Percept. Mot. Ski. 2021, 128, 2605–2620. [Google Scholar] [CrossRef] [PubMed]
- Tofani, M.; Scarcella, L.; Galeoto, G.; Giovannone, F.; Sogos, C. Behavioral gender differences across Pre-School Children with Autism Spectrum Disorders: A cross-sectional study. J. Autism Dev. Disord. 2022, 1–6. [Google Scholar] [CrossRef]
- Ioncoli, M.; Berardi, A.; Tofani, M.; Panuccio, F.; Servadio, A.; Valente, D.; Galeoto, G. Crosscultural validation of the community integration questionnaire–revised in an Italian population. Occup. Ther. Int. 2020, 2020, 8916541. [Google Scholar] [CrossRef]
- Brown, L.; Burns, Y.R.; Watter, P.; Gray, P.H.; Gibbons, K.S. Behaviour of 4- to 5-year-old nondisabled ELBW children: Outcomes following group-based physiotherapy intervention. Child Care Health Dev. 2017, 44, 227–233. [Google Scholar] [CrossRef]
- Van Houdt, C.A.; van Wassenaer-Leemhuis, A.G.; Oosterlaan, J.; Königs, M.; Koopman-Esseboom, C.; Laarman, A.R.C.; Aarnoudse-Moens, C.S.H. Executive function training in very preterm children: A randomized controlled trial. Eur. Child Adolesc. Psychiatry 2020, 10, 2100. [Google Scholar] [CrossRef]
- Rodríguez, G.M.; Bagner, D.M.; Graziano, P.A. Parent Training for Children Born Premature: A Pilot Study Examining the Moderating Role of Emotion Regulation. Child Psychiatry Hum. Dev. 2013, 45, 143–152. [Google Scholar] [CrossRef]
- Bagner, D.M.; Sheinkopf, S.J.; Vohr, B.R.; Lester, B.M. Parenting Intervention for Externalizing Behavior Problems in Children Born Premature: An Initial Examination. J. Dev. Behav. Pediatr. 2010, 31, 209–216. [Google Scholar] [CrossRef]
- Siffredi, V.; Liverani, M.C.; Hüppi, P.S.; Freitas, L.G.A.; Gimbert, F. The effect of a mindfulness-based intervention on executive, behavioural and socio-emotional competencies in very preterm young adolescents. Sci. Rep. 2021, 11, 19876. [Google Scholar] [CrossRef] [PubMed]
- Berger, V.; Alperson, S. A General Framework for the Evaluation of Clinical Trial Quality. Rev. Recent Clin. Trials 2009, 4, 79–88. [Google Scholar] [CrossRef]
- Berardi, A.; Tofani, M.; Colalelli, F.; Valente, D.; Sellitto, G.; Ruotolo, I.; Galeoto, G. The psychometric properties of the Italian version of the PEDro Scale. Gazz. Med. Ital.-Arch. Sci. Med. 2022, 181, 357–365. [Google Scholar] [CrossRef]
- Della Longa, L.; Nosarti, C.; Farroni, T. Emotion Recognition in Preterm and Full-Term School-Age Children. Int. J. Environ. Res. Public Health 2022, 19, 6507. [Google Scholar] [CrossRef]
- Zhang, X.; Kurtz, M.; Lee, S.-Y.; Liu, H. Early Intervention for Preterm Infants and Their Mothers. J. Perinat. Neonatal Nurs. 2014, 35, E69–E82. [Google Scholar] [CrossRef]
- Sala, G.; Aksayli, N.D.; Tatlidil, K.S.; Tatsumi, T.; Gondo, Y.; Gobet, F. Near and Far Transfer in Cognitive Training: A Second-Order Meta-Analysis. Psychology 2019, 5, 18. [Google Scholar] [CrossRef]
- Giangiacomo, E.; Visaggi, M.C.; Aceti, F.; Giacchetti, N.; Martucci, M.; Giovannone, F.; Valente, D.; Galeoto, G.; Tofani, M.; Sogos, C. Early Neuro-Psychomotor Therapy Intervention for Theory of Mind and Emotion Recognition in Neurodevelopmental Disorders: A Pilot Study. Children 2022, 9, 1142. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, G.; Galeoto, G.; Sogos, C.; Berardi, A.; Tofani, M. The efficacy of executive function interventions in children with autism spectrum disorder: A systematic review and meta-analysis. Expert Rev. Neurother. 2022, 22, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Poehlmann, J.; Schwichtenberg, A.J.M.; Shlafer, R.J.; Hahn, E.; Bianchi, J.-P.; Warner, R. Emerging self-regulation in toddlers born preterm or low birth weight: Differential susceptibility to parenting. Dev. Psychopathol. 2011, 23, 177–193. [Google Scholar] [CrossRef]
- Barlow, J.; Bergman, H.; Kornør, H.; Wei, Y.; Bennett, C. Group-based parent training programmes for improving emotional and behavioural adjustment in young children. Cochrane Database Syst. Rev. 2016, CD003680. [Google Scholar] [CrossRef]
- Spittle, A.; Treyvaud, K. The role of early developmental intervention to influence neurobehavioral outcomes of children born preterm. Semin. Perinatol. 2016, 40, 542–548. [Google Scholar] [CrossRef]
- Spittle, A.; Orton, J.; Anderson, P.J.; Boyd, R.; Doyle, L.W. Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants. Cochrane Database Syst. Rev. 2015, 2015, CD005495. [Google Scholar] [CrossRef] [PubMed]
- Ames, C.S.; Richardson, J.; Payne, S.; Smith, P.; Leigh, E. Mindfulness-based cognitive therapy for depression in adolescents. Child Adolesc. Ment. Health 2014, 19, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Cotton, S.; Luberto, C.M.; Sears, R.W.; Strawn, J.R.; Stahl, L.; Wasson, R.S.; Delbello, M.P. Mindfulness-based cognitive therapy for youth with anxiety disorders at risk for bipolar disorder: A pilot trial. Early Interv. Psychiatry 2015, 10, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Díaz-González, M.C.; Pérez Dueñas, C.; Sánchez-Raya, A.; Moriana Elvira, J.A.; Sánchez Vázquez, V. Mindfulness-based stress reduction in adolescents with mental disorders: A randomised clinical trial. Psicothema 2018, 30, 165–170. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-Based Interventions in Context: Past, Present, and Future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Schuman-Olivier, Z.; Trombka, M.; Lovas, D.A.; Brewer, J.A.; Vago, D.R.; Gawande, R.; Dunne, J.P.; Lazar, S.W.; Loucks, E.B.; Fulwiler, C. Mindfulness and Behavior Change. Harv. Rev. Psychiatry 2020, 28, 371–394. [Google Scholar] [CrossRef]
- Crane, R.S.; Brewer, J.; Feldman, C.; Kabat-Zinn, J.; Santorelli, S.; Williams, J.M.; Kuyken, W. What defines mindfulness-based programs? The warp and the weft. Psychol. Med. 2017, 47, 990–999. [Google Scholar] [CrossRef]
- Baraldi, E.; Allodi, M.W.; Löwing, K.; Smedler, A.-C.; Westrup, B.; Ådén, U. Stockholm preterm interaction-based intervention (SPIBI)—Study protocol for an RCT of a 12-month parallel-group post-discharge program for extremely preterm infants and their parents. BMC Pediatr. 2020, 20, 49. [Google Scholar] [CrossRef]
- Valencia, F.; Urbiola, E.; Romero-González, M.; Navas, I.; Elías, M.; Garriz, A.; Ramírez, A.; Villalta, L. Protocol for a randomized pilot study (FIRST STEPS): Implementation of the Incredible Years-ASLD® program in Spanish children with autism and preterm children with communication and/or socialization difficulties. Trials 2021, 22, 291. [Google Scholar] [CrossRef]


{kind=link}
| Study | Sample | Intervention Group | Control Group | Duration and Follow-up | Outcome Measures | Results | Jadad | PEDro |
|---|---|---|---|---|---|---|---|---|
| Brown et al. (2017) [57] | 50 4-year-old children ELBW IG:24; CG: 26 | Group-based physiotherapy intervention | Standard care: best practice advice | 6 group-based physiotherapy weekly sessions and home program F: 12 months | Child Behavior Checklist (CBCL); Movement Assessment Battery for Children Second Edition, Beery Visual-Motor Integration Test 5th Edition and Peabody Picture Vocabulary Test 4th Edition | IG and CG improved on CBCL total problems score at baseline and 1-year follow-up, p = 0.004. There were no significant differences between groups for CBCL internalizing, externalizing or total problems scores | 2 | 6 |
| Van Houdt et al. (2019) [58] | 85 8–12-year-old children born very preterm IG: 29 CG: 26 (placebo training); 30 (waitlist) | EF training | Placebo training or waitlist | The EF and placebo training involved 6 weeks, for a total of 25 (30–45 min) sessions of the training program. F: 5 months | Child version of the Attention Network Test (Child-ANT), Strengths and Difficulties Questionnaire (SDQ) and Self-Perception Profile for Children (CBSK) | IG improved on all training tasks but not on attention, parent- or teacher-rated behavioral and emotional functioning, or self-perceived competence | 5 | 9 |
| Rodríguez et al. (2014) [59] | 28 children born preterm with externalizing behavior problems and their mothers IG: 14 CG: 14 | Parent training (PCIT) | Waitlist | One session a week for four months | Eyberg Child Behavior Inventory (ECBI) and videotaped 10 min parent–child interaction | PCIT increased global regulation (p < 0.05) | 2 | 4 |
| Bagner et al. (2010) [60] | 28 children born preterm with externalizing behavior problems and their mothers IG: 14 CG: 14 | Parent training (PCIT) | Waitlist | One session a week for four months F: 4 months | Eyberg Child Behavior Inventory (ECBI) and videotaped 10 min parent–child interaction | IG had fewer attention problems, aggressive behaviors, and externalizing and internalizing behavior problems | 3 | 8 |
| Siffredi et al. (2020) [61] | 56 very preterm young adolescents, IG: 29, CG: 27 | Mindfulness-based intervention (MBI) | Waitlist | 8-week MBI in a cross-over design. F: 1 month F2: 3 months | Behavior Rating Inventory of Executive Function—parent version (BRIEF), Strength and Difficulties Questionnaire—parent version (SDQ), KIDSCREEN-27, NEPSY-II | IG enhanced organizational capabilities in everyday life and decreased SDQ scores, but it was not maintained at follow-up except for the improvement of information processing | 2 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dell’Aversana, V.; Tofani, M.; Valente, D. Emotional Regulation Interventions on Developmental Course for Preterm Children: A Systematic Review of Randomized Control Trials. Children 2023, 10, 603. https://doi.org/10.3390/children10030603
Dell’Aversana V, Tofani M, Valente D. Emotional Regulation Interventions on Developmental Course for Preterm Children: A Systematic Review of Randomized Control Trials. Children. 2023; 10(3):603. https://doi.org/10.3390/children10030603
Chicago/Turabian StyleDell’Aversana, Vincenza, Marco Tofani, and Donatella Valente. 2023. "Emotional Regulation Interventions on Developmental Course for Preterm Children: A Systematic Review of Randomized Control Trials" Children 10, no. 3: 603. https://doi.org/10.3390/children10030603
APA StyleDell’Aversana, V., Tofani, M., & Valente, D. (2023). Emotional Regulation Interventions on Developmental Course for Preterm Children: A Systematic Review of Randomized Control Trials. Children, 10(3), 603. https://doi.org/10.3390/children10030603