
Genetic Predisposition to Primary Lactose Intolerance Does Not Influence Dairy Intake and Health-Related Quality of Life in Romanian Children: A Hospital-Based Cross-Sectional Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Analyzed Variables
2.3. Molecular Analysis
2.4. Statistical Analysis
2.5. Ethics
3. Results
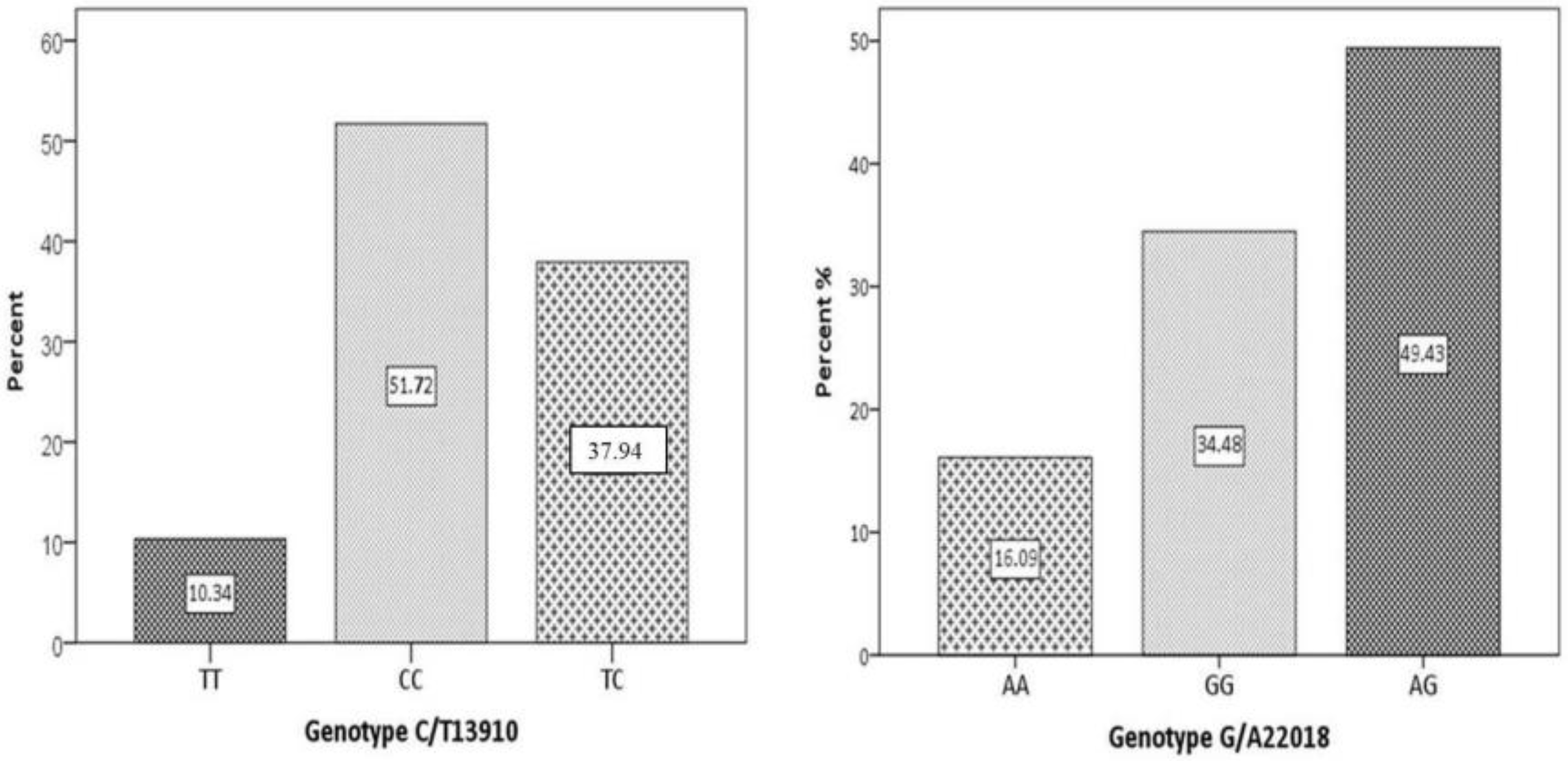
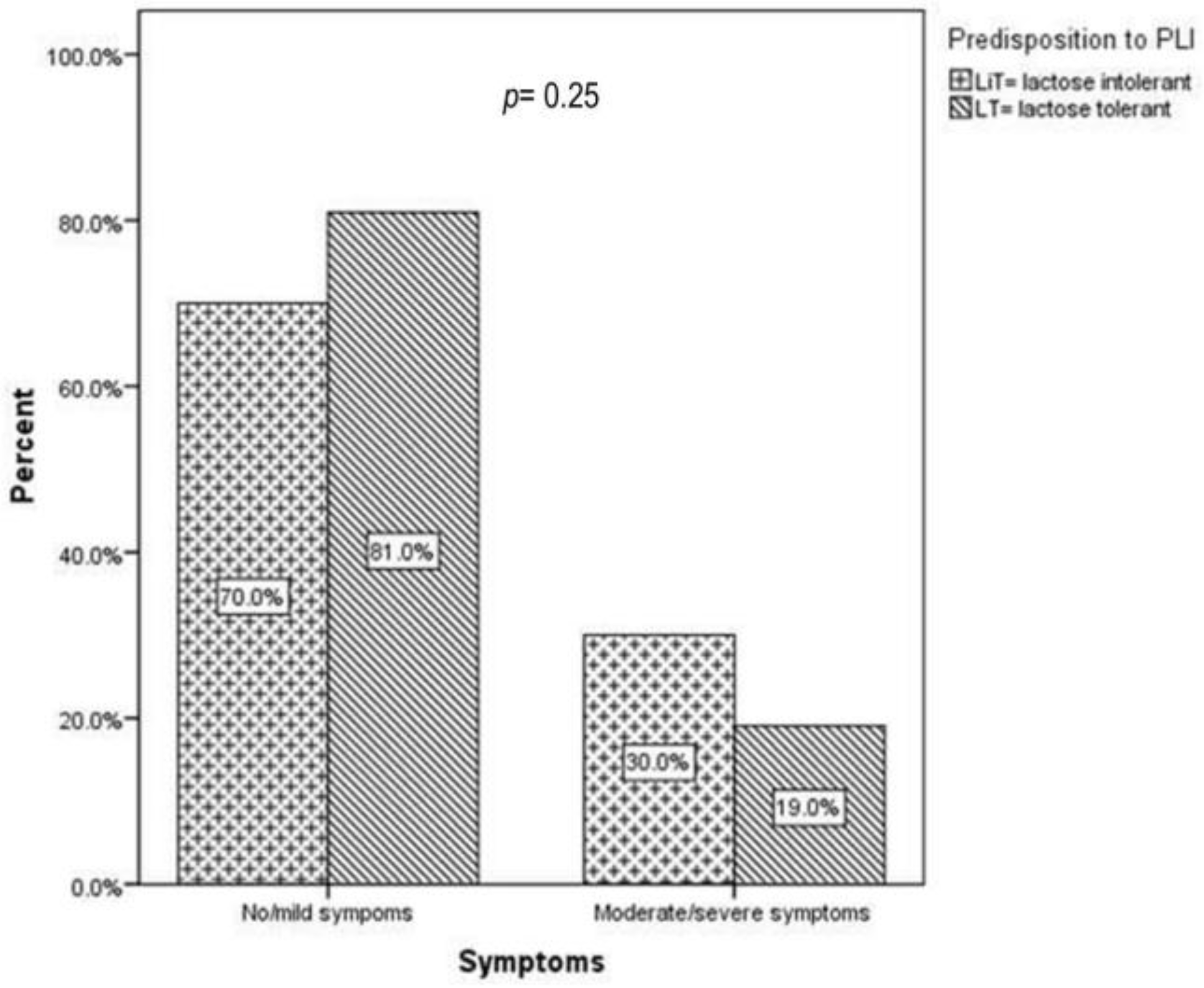
3.1. Genetic Predisposition to PLI and PLI-Related Symptoms
3.2. Genetic Predisposition to PLI and Dairy Intake
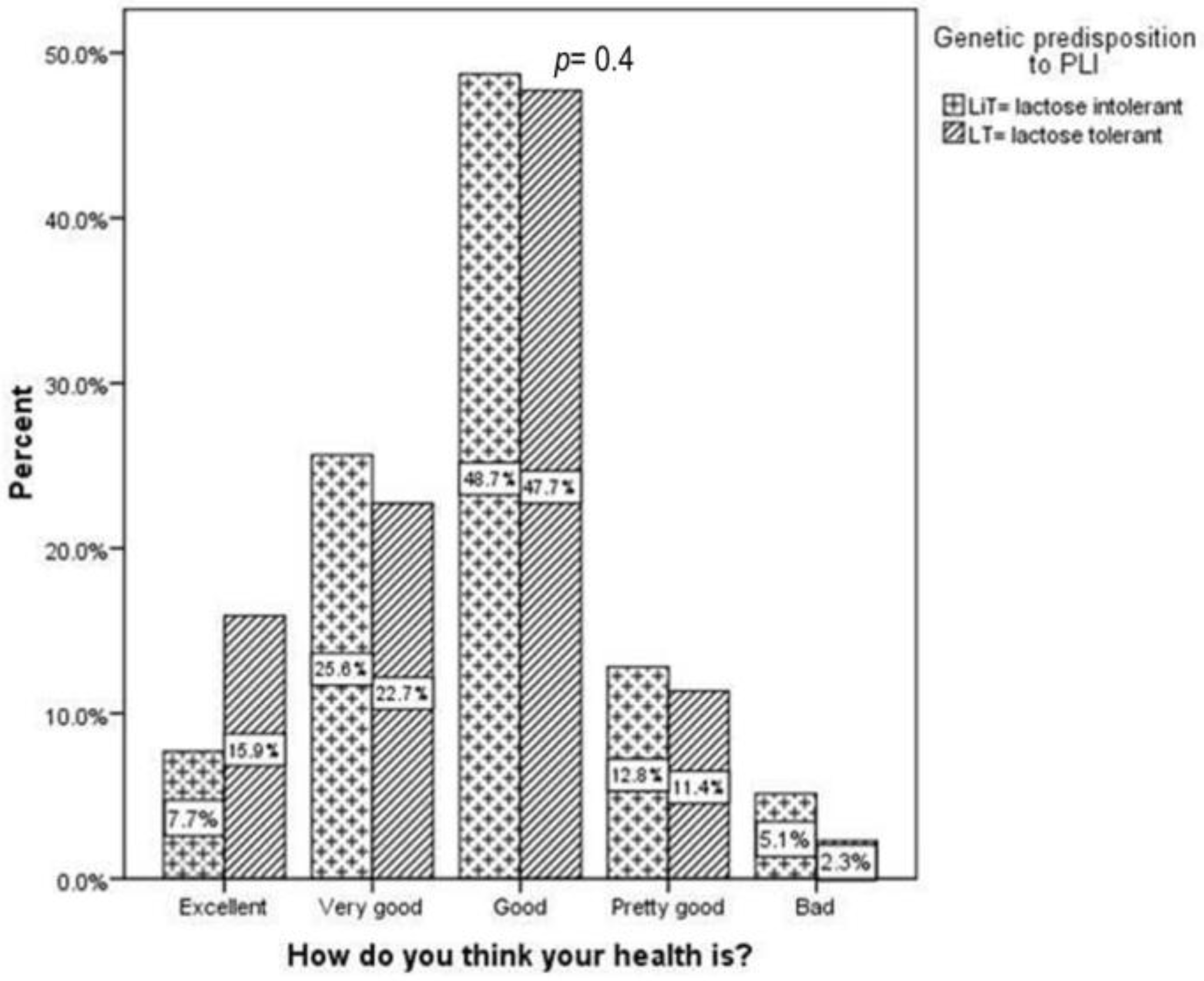
3.3. Genetic Predisposition to PLI and HRQoL
4. Discussion
4.1. Genetic Predisposition to PLI and PLI-Related Symptoms
4.2. Genetic Predisposition to PLI and Dairy Intake
4.3. Genetic Predisposition to PLI and HRQoL
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



References
- Heyman, M.B.; Committee on Nutrition. Lactose Intolerance in Infants, Children, and Adolescents. Pediatrics 2006, 118, 1279–1286. [Google Scholar] [CrossRef] [Green Version]
- Mattar, R.; de Campos Mazo, D.F.; Carrilho, F.J. Lactose intolerance: Diagnosis, genetic, and clinical factors. Clin. Exp. Gastroenterol. 2012, 5, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Zecca, L.; Mesonero, J.E.; Stutz, A.; Poirée, J.C.; Giudicelli, J.; Cursio, R.; Gloor, S.M.; Semenza, G. Intestinal lactase-phlorizin hydrolase (LPH): The two catalytic sites; the role of the pancreas in pro-LPH maturation. FEBS Lett. 1998, 435, 225–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Järvelä, I.; Torniainen, S.; Kolho, K.L. Molecular genetics of human lactase deficiencies. Ann. Med. 2009, 41, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Lomer, M.C.E.; Parkes, G.C.; Sanderson, J.D. Review article: Lactose intolerance in clinical practice–myths and realities. Aliment. Pharmacol. Ther. 2008, 27, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Broekaert, I.J.; Borrelli, O.; Dolinsek, J.; Martin-de-Carpi, J.; Mas, E.; Miele, E.; Pienar, C.; Ribes-Koninckx, C.; Thomassen, R.; Thomson, M.; et al. An ESPGHAN Position Paper on the Use of Breath Testing in Paediatric Gastroenterology. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 123. [Google Scholar] [CrossRef]
- Robles, L.; Priefer, R. Lactose Intolerance: What Your Breath Can Tell You. Diagnostics 2020, 10, 412. [Google Scholar] [CrossRef] [PubMed]
- Catanzaro, R.; Sciuto, M.; Marotta, F. Lactose intolerance: An update on its pathogenesis, diagnosis, and treatment. Nutr. Res. 2021, 89, 23–34. [Google Scholar] [CrossRef]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M.; et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. Am. J. Gastroenterol. 2017, 112, 775–784. [Google Scholar] [CrossRef] [Green Version]
- Almazar, A.E.; Chang, J.Y.; Larson, J.J.; Atkinson, E.J.; Locke, G.R.; Talley, N.J.; Saito, Y.A. Comparison of Lactase Variant MCM6– 13910 C>T Testing and Self-Report of Dairy Sensitivity in Patients with Irritable Bowel Syndrome. J. Clin. Gastroenterol. 2019, 53, e227. [Google Scholar] [CrossRef]
- Kerber, M.; Oberkanins, C.; Kriegshäuser, G.; Kollerits, B.; Dossenbach-Glaninger, A.; Fuchs, D.; Ledochowski, M. Hydrogen breath testing versus LCT genotyping for the diagnosis of lactose intolerance: A matter of age? Clin. Chim. Acta 2007, 383, 91–96. [Google Scholar] [CrossRef]
- Pohl, D.; Savarino, E.; Hersberger, M.; Behlis, Z.; Stutz, B.; Goetze, O.; Eckardstein, A.v.; Fried, M.; Tutuian, R. Excellent agreement between genetic and hydrogen breath tests for lactase deficiency and the role of extended symptom assessment. Br. J. Nutr. 2010, 104, 900–907. [Google Scholar] [CrossRef]
- Alliende, F.; Vial, C.; Espinoza, K.; Schnettle, D.; Romero, V.; Miquel, I.; Arancibia, M.E.; Rios, G.; Rodriguez, L.; Quesada, S. Accuracy of a Genetic Test for the Diagnosis of Hypolactasia in Chilean Children: Comparison with the Breath Test. J. Pediatr. Gastroenterol. Nutr. 2016, 63, e10. [Google Scholar] [CrossRef]
- Tomczonek-Moruś, J.; Wojtasik, A.; Zeman, K.; Smolarz, B.; Bąk-Romaniszyn, L. 13910C>T and 22018G>A LCT gene polymorphisms in diagnosing hypolactasia in children. United Eur. Gastroenterol. J. 2019, 7, 210–216. [Google Scholar] [CrossRef] [Green Version]
- Couce, M.L.; Sánchez-Pintos, P.; González-Vioque, E.; Leis, R. Clinical Utility of LCT Genotyping in Children with Suspected Functional Gastrointestinal Disorder. Nutrients 2020, 12, 3017. [Google Scholar] [CrossRef] [PubMed]
- Rasinperä, H.; Savilahti, E.; Enattah, N.S.; Kuokkanen, M.; Tötterman, N.; Lindahl, H.; Järvelä, I.; Kolho, K.-L. A genetic test which can be used to diagnose adult-type hypolactasia in children. Gut 2004, 53, 1571–1576. [Google Scholar] [CrossRef] [Green Version]
- Stefano, M.D.; Terulla, V.; Tana, P.; Mazzocchi, S.; Romero, E.; Corazza, G.R. Genetic test for lactase non-persistence and hydrogen breath test: Is genotype better than phenotype to diagnose lactose malabsorption? Dig. Liver Dis. 2009, 41, 474–479. [Google Scholar] [CrossRef]
- Hodges, J.K.; Cao, S.; Cladis, D.P.; Weaver, C.M. Lactose Intolerance and Bone Health: The Challenge of Ensuring Adequate Calcium Intake. Nutrients. 2019, 11, 718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, K.; Hill, R.J. The role of food intolerance in functional gastrointestinal disorders in children. Aust. Fam. Phys. 2014, 43, 686–689. [Google Scholar]
- Misselwitz, B.; Butter, M.; Verbeke, K.; Fox, M.R. Update on lactose malabsorption and intolerance: Pathogenesis, diagnosis and clinical management. Gut 2019, 68, 2080–2091. [Google Scholar] [CrossRef] [Green Version]
- Alharbi, O.; El-Sohemy, A. Lactose Intolerance (LCT-13910C>T) Genotype Is Associated with Plasma 25-Hydroxyvitamin D Concentrations in Caucasians: A Mendelian Randomization Study. J. Nutr. 2017, 147, 1063–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, E.L.; Huang, L.; Bouzid, Y.Y.; Kirschke, C.P.; Durbin-Johnson, B.; Baldiviez, L.M.; Bonnel, E.L.; Keim, N.L.; Korf, I.; Stephensen, C.B.; et al. Association of Lactase Persistence Genotypes (rs4988235) and Ethnicity with Dairy Intake in a Healthy U.S. Population. Nutrients 2019, 11, 1860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popadowska, A.; Kempinska-Podhorodecka, A. Relation of the C/T-13910 LCT Polymorphism with Body Composition Measures and Their Modulation by Dairy Products in a Caucasian Men. Am. J. Men’s Health 2021, 15, 15579883211007272. [Google Scholar] [CrossRef]
- Jansson-Knodell, C.L.; White, M.; Lockett, C.; Xu, H.; Shin, A. Associations of Food Intolerance with Irritable Bowel Syndrome, Psychological Symptoms, and Quality of Life. Clin. Gastroenterol. Hepatol. 2022, 20, 2121–2131.e3. [Google Scholar] [CrossRef]
- Yerushalmy-Feler, A.; Soback, H.; Lubetzky, R.; Ben-Tov, A.; Dali-Levy, M.; Galai, T.; Cohen, S. One-third of children with lactose intolerance managed to achieve a regular diet at the three-year follow-up point. Acta Paediatr. 2018, 107, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.d.J.; Leite, I.D.S.; Rodrigues, J.W.; Almeida, S.P.d.; Nóbrega, B.P.; Sampaio, J.D.R. Analysis of lactose intolerance in students with suggestive symptoms of irritable bowel syndrome. Arq. Gastroenterol. 2019, 56, 304–311. [Google Scholar] [CrossRef] [Green Version]
- Erminia, R.; Ilaria, B.; Tiziana, M.; Silvia, P.; Antonio, N.; Pierpaolo, D.A.; Loris, B. HRQoL questionnaire evaluation in lactose intolerant patients with adverse reactions to foods. Intern. Emerg. Med. 2013, 8, 493–496. [Google Scholar] [CrossRef]
- Zheng, X.; Chu, H.; Cong, Y.; Deng, Y.; Long, Y.; Zhu, Y.; Pohl, D.; Fried, M.; Dai, N.; Fox, M. Self-reported lactose intolerance in clinic patients with functional gastrointestinal symptoms: Prevalence, risk factors, and impact on food choices. Neurogastroenterol. Motil. 2015, 27, 1138–1146. [Google Scholar] [CrossRef]
- Campbell, A.K.; Matthews, S.B.; Vassel, N.; Cox, C.D.; Naseem, R.; Chaichi, J.; Holland, I.B.; Green, J.; Wann, K.T. Bacterial metabolic ‘toxins’: A new mechanism for lactose and food intolerance, and irritable bowel syndrome. Toxicology 2010, 278, 268–276. [Google Scholar] [CrossRef]
- Tomba, C.; Baldassarri, A.; Coletta, M.; Cesana, B.M.; Basilisco, G. Is the subjective perception of lactose intolerance influenced by the psychological profile? Aliment. Pharmacol. Ther. 2012, 36, 660–669. [Google Scholar] [CrossRef]
- Strinnholm, Å.; Hedman, L.; Winberg, A.; Jansson, S.A.; Lindh, V.; Rönmark, E. Health Related Quality of Life among schoolchildren aged 12–13 years in relation to food hypersensitivity phenotypes: A population-based study. Clin. Transl. Allergy 2017, 7, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerbault, P. The Onset of Lactase Persistence in Europe. Hum. Hered. 2014, 76, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, S.; Body, J.J.; Bruyère, O.; Bergmann, P.; Brandi, M.L.; Cooper, C.; Devogelaer, J.-P.; Gielen, E.; Goemaere, S.; Kaufman, J.-M.; et al. Effects of Dairy Products Consumption on Health: Benefits and Beliefs—A Commentary from the Belgian Bone Club and the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases. Calcif. Tissue Int. 2016, 98, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Di Stefano, M.; Brondino, N.; Bonaso, V.; Miceli, E.; Lapia, F.; Grandi, G.; Pagani, E.; Corazza, G.R.; Di Sabatino, A. The Perception of Lactose-Related Symptoms of Patients with Lactose Malabsorption. Int. J. Environ. Res. Public Health 2022, 19, 10234. [Google Scholar] [CrossRef]
- Pienar, C.; Pop, L.; Lăzărescu, M.; Costăchescu, R.; Șeclăman, E. Anthropometric and metabolic profile of children with gene polymorphisms for primary lactose intolerance. Exp. Ther. Med. 2021, 22, 1333. [Google Scholar] [CrossRef]
- Mattar, R.; do Socorro Monteiro, M.; Matie Kinoshita da Silva, J.; Jose Carrilho, F. LCT-22018G>A single nucleotide polymorphism is a better predictor of adult-type hypolactasia/lactase persistence in Japanese-Brazilians than LCT-13910C>T. Clinics 2010, 65, 1399–1400. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Sun, H.; Zhang, X.; Wang, J.; Sun, D.; Chen, F.; Bai, J.; Fu, S. The -22018A allele matches the lactase persistence phenotype in northern Chinese populations. Scand. J. Gastroenterol. 2010, 45, 168–174. [Google Scholar] [CrossRef]
- Suchy, F.J.; Brannon, P.M.; Carpenter, T.O.; Fernandez, J.R.; Gilsanz, V.; Gould, J.B.; Hall, K.; Hui, S.L.; Lupton, J.; Mennella, J.; et al. National Institutes of Health Consensus Development Conference: Lactose Intolerance and Health. Ann. Intern. Med. 2010, 152, 792–796. [Google Scholar] [CrossRef] [Green Version]
- Szilagyi, A.; Ishayek, N. Lactose Intolerance, Dairy Avoidance, and Treatment Options. Nutrients 2018, 10, 1994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koppen, I.J.N.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Benninga, M.A. The pediatric Rome IV criteria: What’s new? Expert Rev. Gastroenterol. Hepatol. 2017, 11, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Nicklas, T.A.; Qu, H.; Hughes, S.O.; Wagner, S.E.; Foushee, H.R.; Shewchuk, R.M. Prevalence of self-reported lactose intolerance in a multiethnic sample of adults. Nutr. Today 2009, 44, 222–227. [Google Scholar] [CrossRef]
- Gremse, D.A.; Greer, A.S.; Vacik, J.; Dipalma, J.A. Abdominal Pain Associated with Lactose Ingestion in Children with Lactose Intolerance. Clin. Pediatr. 2003, 42, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Ugidos-Rodríguez, S.; Matallana-González, M.C.; Sánchez-Mata, M.C. Lactose malabsorption and intolerance: A review. Food Funct. 2018, 9, 4056–4068. [Google Scholar] [CrossRef]
- Casellas, F.; Aparici, A.; Pérez, M.J.; Rodríguez, P. Perception of lactose intolerance impairs health-related quality of life. Eur. J. Clin. Nutr. 2016, 70, 1068–1072. [Google Scholar] [CrossRef] [PubMed]
- Obermayer-Pietsch, B.M.; Bonelli, C.M.; Walter, D.E.; Kuhn, R.J.; Fahrleitner-Pammer, A.; Berghold, A.; Goessler, W.; Stepan, V.; Dobnig, H.; Leb, G.; et al. Genetic Predisposition for Adult Lactose Intolerance and Relation to Diet, Bone Density, and Bone Fractures. J. Bone Miner. Res. 2004, 19, 42–47. [Google Scholar] [CrossRef]
- Schiffner, R.; Kostev, K.; Gothe, H. Do patients with lactose intolerance exhibit more frequent comorbidities than patients without lactose intolerance? An analysis of routine data from German medical practices. Ann. Gastroenterol. 2016, 29, 174–179. [Google Scholar] [CrossRef] [Green Version]
- Kull, M.; Kallikorm, R.; Lember, M. Impact of molecularly defined hypolactasia, self-perceived milk intolerance and milk consumption on bone mineral density in a population sample in Northern Europe. Scand. J. Gastroenterol. 2009, 44, 415–421. [Google Scholar] [CrossRef]
- Qiao, R.; Huang, C.; Du, H.; Zeng, G.; Li, L.; Ye, S. Milk consumption and lactose intolerance in adults. Biomed. Environ. Sci. 2011, 24, 512–517. [Google Scholar]
- Boukria, O.; El Hadrami, E.M.; Boudalia, S.; Safarov, J.; Leriche, F.; Aït-Kaddour, A. The Effect of Mixing Milk of Different Species on Chemical, Physicochemical, and Sensory Features of Cheeses: A Review. Foods 2020, 9, 1309. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lactose Tolerant n = 45 | Lactose Intolerant n = 42 | p 1 | ||
|---|---|---|---|---|
| Age (years) 2 | 11.09 ± 3.59 | 10.17 ± 3.4 | 0.221 | |
| Gender 3 | Girls | 21/45 | 24/42 | 0.744 |
| Boys | 24/45 | 18/42 | ||
| Weight (kg) 2 | 42.92 ± 16.94 | 39.07 ± 17.41 | 0.372 | |
| Height (cm) 2 | 144.37 ± 18.38 | 148.67 ± 18.06 | 0.273 | |
| BMI (kg/mp) 2 | 19 ± 5.08 | 17.99 ± 4.65 | 0.440 | |
| Homozygosy for Genotype 13910 (n = 15) | Homozygosy for Both Genotype 13910 and 22018 (n = 30) | Heterozygosy/Absence of Polymorphisms (n = 42) | p 1 | ||
|---|---|---|---|---|---|
| Gender 2 | Girls | 7 | 21 | 17 | 0.045 |
| Boys | 8 | 9 | 25 | ||
| Age (years) 3 | 9.71 ± 3.14 | 11.2 ± 3.52 | 10.62 ± 3.64 | 0.406 | |
| Weight (kg) 3 | 39.89 ± 17.79 | 43.73 ± 17.54 | 38.24 ± 15.57 | 0.355 | |
| Height (m) 3 | 142 ± 18.69 | 148 ± 19.03 | 145.13 ± 18.59 | 0.549 | |
| BMI (kg/m2) 3 | 18.86 ± 5.38 | 19.19 ± 4.67 | 17.87 ± 4.67 | 0.362 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pienar, C.; Pop, L.; Lăzărescu, M.; Costăchescu, R.; Mogoi, M.; Mare, R.; Șeclăman, E. Genetic Predisposition to Primary Lactose Intolerance Does Not Influence Dairy Intake and Health-Related Quality of Life in Romanian Children: A Hospital-Based Cross-Sectional Study. Children 2023, 10, 1075. https://doi.org/10.3390/children10061075
Pienar C, Pop L, Lăzărescu M, Costăchescu R, Mogoi M, Mare R, Șeclăman E. Genetic Predisposition to Primary Lactose Intolerance Does Not Influence Dairy Intake and Health-Related Quality of Life in Romanian Children: A Hospital-Based Cross-Sectional Study. Children. 2023; 10(6):1075. https://doi.org/10.3390/children10061075
Chicago/Turabian StylePienar, Corina, Liviu Pop, Marilena Lăzărescu, Radmila Costăchescu, Mirela Mogoi, Ruxandra Mare, and Edward Șeclăman. 2023. "Genetic Predisposition to Primary Lactose Intolerance Does Not Influence Dairy Intake and Health-Related Quality of Life in Romanian Children: A Hospital-Based Cross-Sectional Study" Children 10, no. 6: 1075. https://doi.org/10.3390/children10061075
APA StylePienar, C., Pop, L., Lăzărescu, M., Costăchescu, R., Mogoi, M., Mare, R., & Șeclăman, E. (2023). Genetic Predisposition to Primary Lactose Intolerance Does Not Influence Dairy Intake and Health-Related Quality of Life in Romanian Children: A Hospital-Based Cross-Sectional Study. Children, 10(6), 1075. https://doi.org/10.3390/children10061075