
Mobile Dressing Trolleys Improve Satisfaction and Logistics on Pediatric Surgery Wards

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Observational Periods
2.1.1. First Time Period: No Dressing Trolley, Group 1
2.1.2. Second Time Period: Application of the Dressing Trolley, Group 2
2.2. The Dressing Trolley and Logistics

2.3. Outcome Parameters and Data Acquisition
2.4. Statistical Analysis
3. Results
3.1. Outcome Parameters
3.2. Surgeon Performing the Dressing Changes
3.3. Subjective Evaluation of the Dressing Trolley
4. Discussion
4.1. Satisfaction with the Procedures
4.2. The Effect of Stress on the Surgical Outcome and the Influence of Patient Satisfaction
4.3. Increasing Patient, Parent and Medical Staff Satisfaction
4.4. Dressing Types and Sizes
4.5. Dressing Change Preparation Time
4.6. Duration of the Dressing Change
4.7. Subjective Evaluation of the Dressing Trolley by a Questionnaire
4.8. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xiang, H.; Shen, J.; Wheeler, K.K.; Patterson, J.; Lever, K.; Armstrong, M.; Shi, J.; Thakkar, R.K.; Groner, J.I.; Noffsinger, D.; et al. Efficacy of Smartphone Active and Passive Virtual Reality Distraction vs. Standard Care on Burn Pain among Pediatric Patients: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2112082. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, C.K.; Lasoff, E.; Eide, Y.; Freeman, R.; McEttrick, M.; Dar, R.; Helgerson, R.; Remensynder, J.; Kalin, N. Learned helplessness and the pediatric burn patient: Dressing change behavior and serum cortisol and beta-endorphin. Adv. Pediatr. 1991, 38, 335–363. [Google Scholar] [CrossRef] [PubMed]
- Graves, C.L.; Longley, E.K.; Erickson, E.H.; Debusk, R.W. Where, oh where has our dressing cart gone? Mod. Hosp. 1953, 80, 60–61. [Google Scholar] [PubMed]
- Yazdi, M.G.; Naderizadeh, M.; Afzalipour, R.; Abedi, H.; Radmehr, M.; Yazdi, R.G.; Pashaghi, S.S. Designing and Developing Automatic Trolley for Washing and Dressing the Wounds. J. Biomed. Phys. Eng. 2017, 7, 409–414. [Google Scholar]
- Bailey, B.; Daoust, R.; Doyon-Trottier, E.; Dauphin-Pierre, S.; Gravel, J. Validation and properties of the verbal numeric scale in children with acute pain. Pain 2010, 149, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Shields, B.J.; Palermo, T.M.; Powers, J.D.; Grewe, S.D.; Smith, G.A. Predictors of a child’s ability to use a visual analogue scale. Child Care Health Dev. 2003, 29, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Shields, B.J.; Cohen, D.M.; Harbeck-Weber, C.; Powers, J.D.; Smith, G.A. Pediatric pain measurement using a visual analogue scale: A comparison of two teaching methods. Clin. Pediatr. 2003, 42, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. 11), S240–S252. [Google Scholar]
- Voutilainen, A.; Pitkäaho, T.; Kvist, T.; Vehviläinen-Julkunen, K. How to ask about patient satisfaction? The visual analogue scale is less vulnerable to confounding factors and ceiling effect than a symmetric Likert scale. J. Adv. Nurs. 2016, 72, 946–957. [Google Scholar] [CrossRef] [PubMed]
- Kiecolt-Glaser, J.K.; Glaser, R. Psychological stress and wound healing: Kiecolt-Glaser et al. (1995). Adv. Mind. Body Med. 2001, 17, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, E.; Petrie, K.J.; Alley, P.G.; Booth, R.J. Psychological stress impairs early wound repair following surgery. Psychosom. Med. 2003, 65, 865–869. [Google Scholar] [CrossRef] [PubMed]
- McGuire, L.; Heffner, K.; Glaser, R.; Needleman, B.; Malarkey, W.; Dickinson, S.; Lemeshow, S.; Cook, C.; Muscarella, P.; Melvin, W.S.; et al. Pain and wound healing in surgical patients. Ann. Behav. Med. 2006, 31, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, F. Work and the Nature of Man; World Pub. Co.: Cleveland, OH, USA, 1966. [Google Scholar]
- Buchhester, S. Patientenzufriedenheit als Kriterium der Dienstleistungsqualität im Krankenhaus; Diplom.de: Hamburg, Germany, 2000; Available online: https://nbn-resolving.org/urn:nbn:de:101:1-201506172732 (accessed on 7 September 2022).
- Ausserhofer, D.; Zander, B.; Busse, R.; Schubert, M.; De Geest, S.; Rafferty, A.M.; Ball, J.; Scott, A.; Kinnunen, J.; Heinen, M.; et al. Prevalence, patterns and predictors of nursing care left undone in European hospitals: Results from the multicountry cross-sectional RN4CAST study. BMJ Qual. Saf. 2014, 23, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, K.; Kuhlmey, A.; Greß, S.; Klauber, J.; Schwinger, A. (Eds.) Pflege-Report 2020: Neuausrichtung von Versorgung und Finanzierung; Springer Nature: New York, NY, USA, 2020. [Google Scholar] [CrossRef]
- Golombek, J.; Fleßa, S. Einflussfaktoren auf die Verweildauer im Beruf und die Standortwahl des Arbeitsplatzes bei Gesundheits- und Krankenpflegern. HBScience 2011, 2, 3–10. [Google Scholar] [CrossRef]
- Porst, R. Fragebogen: Ein Arbeitsbuch; Springer: Berlin/Heidelberg, Germany, 2013; Available online: https://scholar.google.com/scholar_lookup?&title=Fragebogen&publication_year=2014&author=Porst%2CRolf (accessed on 20 September 2022).
- Porst, R. Frageformulierung. In Handbuch Methoden der Empirischen Sozialforschung; Baur, N., Blasius, J., Eds.; Springer Fachmedien: Wiesbaden, Germany, 2019; pp. 829–842. [Google Scholar]
- Benson, K.; Hartz, A.J. A comparison of observational studies and randomized, controlled trials. N. Engl. J. Med. 2000, 342, 1878–1886. [Google Scholar] [CrossRef] [PubMed]
- Dingman, R.O.; Natvig, P.; Winkler, J.M. A new dressing cart for plastic surgery. Plast. Reconstr. Surg. 1957, 19, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Myers, R.S. How to keep dressing cart from carrying contamination. Mod. Hosp. 1959, 93, 136. [Google Scholar] [PubMed]
- Taylor, G.W.; Shooter, R.A.; Allen, S.M. Ward dressing technique for use with central supply. Br. Med. J. 1962, 2, 1746–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Drawer No. | Contents of the Drawer |
|---|---|
| 1 | Thread removal materials, syringes of different sizes, sutures and utensils for wound irrigation |
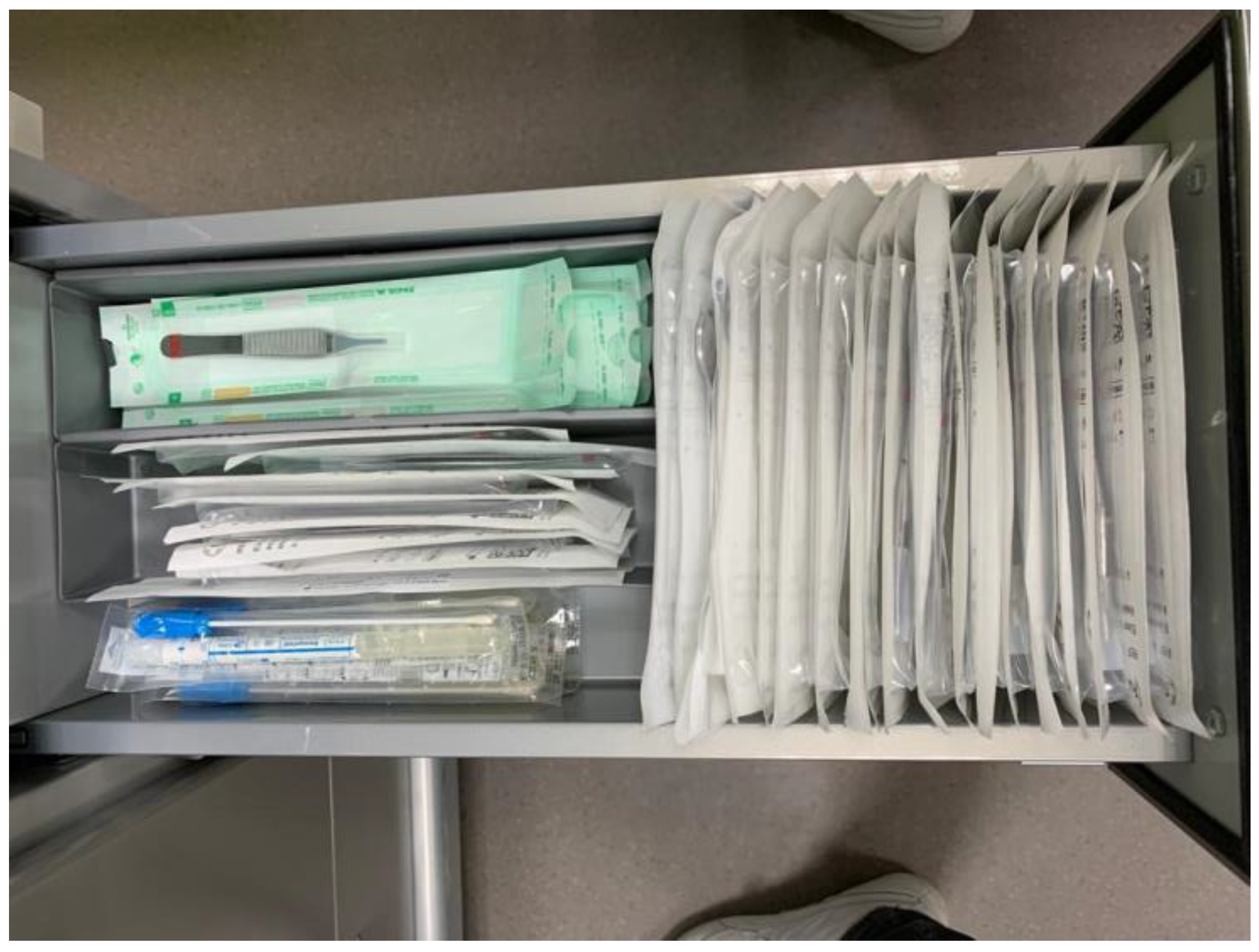
| 2 | Sterile scissors, tweezers and clamps (Figure 2) |
| 3 | Sterile gloves and sterile drapes in different sizes |
| 4 | Rewards for brave children and Moltex underlays |
| 5 | Suction compresses, small Mepithel (Mölnlycke, Germany), elastic bandages, cotton bandages, disposable gowns and face masks |
| 6 | Large Mepithel (Ethicon, Germany), elastic bandages, cotton wool bandages disposable gowns, mouthguards, gauze compresses, gauze bandages, Steristrips, Cavilon skin protection, and antiseptic skin disinfectants |
| 7 | Wound dressings of different sizes, taping strips and plaster remover |
| Question | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| How did you find the selection of bandage materials? | ||||||
| How did you find the number of bandages? | ||||||
| How did you find the manageability of the dressing trolley? | ||||||
| How did you find the cleanliness of the dressing trolley? | ||||||
| Did the dressing trolley facilitate your work? | ||||||
| What is the probability that you will use the dressing trolley in the future? |
| Group 1 No Trolley | Group 2 with Trolley | p-Value | |
|---|---|---|---|
| n | 51 | 49 | |
| Age (years) $ | 1.97 (0.21/9.65) | 2.64 (0.57/10.05) | 0.41 $$ |
| Sex | 0.68 && | ||
| Female * | 26 (51) | 27 (55.1) | |
| Male * | 25 (49) | 22 (44.9) | |
| The child’s mood (VAS, mm) $ | 81.5 (60.0/96.5) | 86.0 (70.75/95.125) | 0.57 $$ |
| Missing data | 4 | 3 | |
| Gender of the accompanying parent | 0.077 && | ||
| Female * | 28 (54.9) | 36 (73.5) | |
| Male * | 13 (25.5) | 10 (20.4) | |
| No accompanying parent present * | 10 (19.6) | 3 (6.1) | |
| Category of the surgical procedure | 0.2 && | ||
| 1. Single incision laparoscopic surgery (SILS) * | 2 (3.9) | 0 (0.0) | |
| 2. Multiport laparoscopy/robotics * | 1 (2.0) | 6 (12.2) | |
| 3. Umbilical minilaparotomy * | 5 (9.8) | 2 (4.1) | |
| 4. Median/transverse laparotomy * | 22 (43.1) | 19 (38.8) | |
| 5. Inguinal hernia, lymph node biopsy/abscess drainage, (sub)cutaneous tumor extirpation/biopsy, burns, anorectal malformation repair * | 14 (27.5) | 16 (32.7) | |
| 6. Vacuum-assisted closure (VAC) * | 7 (13.7) | 6 (12.2) | |
| Type of dressing applied according to the size of the wounds | 0.98 && | ||
| Small dressings with a size of up to 5 cm and a maximum of 3 dressings used * | 25 (49.0) | 25 (51.0) | |
| Large dressings of at least 12 cm (e.g., median laparotomy) * | 17 (33.3) | 16 (32.7) | |
| Special types of dressings comprise those that could not be included in the two abovementioned categories (e.g., VAC) * | 9 (17.6) | 8 (16.3) | |
| Room in whichthe dressing change was performed | 0.85 && | ||
| The patients room * | 43 (84.3) | 42 (85.7) | |
| The examination room * | 8 (15.7) | 7 (14.3) | |
| Sedation of the child for the dressing change | 0.58 && | ||
| No sedation * | 49 (96.1) | 48 (98.0) | |
| Sedation * | 2 (3.9) | 1 (2.0) | |
| Multiresistant Bacteria | 0.16 && | ||
| Patients without multiresistant bacteriae * | 50 (98.0) | 45 (91.8) | |
| Patients with multiresistant bacteriae * | 1 (2.0) | 4 (8.2) | |
| Preparation time (minutes) | 1:16 (0:32/3:43) | 0:00 (0:00/0:10) | <0.001 $$ |
| Duration of the dressing change (minutes) | 3:42 (1:48/8:09) | 1:46 (1:05/7:53) | 0.05 $$ |
| Frequency of leaving the patient’s room to retrieve missing materials | 0.022 && | ||
| Never left the patients room to retreive missing materials * | 26 (51) | 41 (83.7) | |
| Left once | 17 (33.3) | 5 (10.2) | |
| Left 2 times * | 5 (9.8) | 2 (4.1) | |
| Left 3 times * | 1 (2.0) | 1 (2.0) | |
| Left 4 times * | 1 (2.0) | 0 (0.0) | |
| Left 5 times * | 0 (0.0) | 0 (0.0) | |
| Left 6 times * | 1 (2.0) | 0 (0.0) | |
| Time spent outside the patient’s room for retrieving missing materials (seconds) | 46 (27–117) | 18.5 (13.5–85) | 0.048 $$ |
| Total duration of the dressing change consisting of its preparation, execution and cleanup (minutes) $ | 7:04 (3:45–20:26) | 1:55 (1:05–7:58) | 0.001 $$ |
| Missing data | 21 | 0 | |
| Satisfaction of the surgeons with the dressing change (VAS, mm) $ | 85.0 (65.0–96.5) | 97 (88.5–98.5) | <0.001 $$ |
| Satisfaction of the parents with the dressing change (VAS, mm) $ | 94 (75–98) | 96.5 (94–98.125) | 0.042 $$ |
| Missing data | 12 | 7 | |
| Satisfaction of the nursing staff with the dressing change (VAS, mm) $ | 81 (58.5–90.0) | 90.25 (IQR 77.375–97.875) | 0.015 $$ |
| Missing data | 8 | 13 | |
| Satisfaction of the observer with the dressing change (VAS, mm) $ | 79.5 (69.5–87) | 93 (90.75–96) | <0.001 $$ |
| Satisfaction of the children, ifolder than 12 years, with the dressing change (VAS, mm) $ | 87.5 (77.0–94.25) | 93.25 (70.875–96.75) | 0.7 $$ |
| Missing data | 42 | 41 |
| N | Minimum | Maximum | Mean | |
|---|---|---|---|---|
| Selection of bandage material? | 47 | 1 | 3 | 1.34 |
| Number of bandages? | 47 | 1 | 2 | 1.09 |
| Manageability? | 47 | 1 | 3 | 1.60 |
| Cleanliness? | 47 | 1 | 5 | 1.21 |
| Work facilitation? | 47 | 1 | 6 | 1.70 |
| Probability that you will use the dressing trolley in the future? | 47 | 1 | 5 | 1.45 |
| Overall grade | 1.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franck, H.; Dempfle, A.; Reischig, K.; Baastrup, J.; Meinzer, A.; Kossakowski, M.; Krebs, T.F.; Bergholz, R. Mobile Dressing Trolleys Improve Satisfaction and Logistics on Pediatric Surgery Wards. Children 2023, 10, 1089. https://doi.org/10.3390/children10071089
Franck H, Dempfle A, Reischig K, Baastrup J, Meinzer A, Kossakowski M, Krebs TF, Bergholz R. Mobile Dressing Trolleys Improve Satisfaction and Logistics on Pediatric Surgery Wards. Children. 2023; 10(7):1089. https://doi.org/10.3390/children10071089
Chicago/Turabian StyleFranck, Hannes, Astrid Dempfle, Katja Reischig, Jonas Baastrup, Andreas Meinzer, Meike Kossakowski, Thomas Franz Krebs, and Robert Bergholz. 2023. "Mobile Dressing Trolleys Improve Satisfaction and Logistics on Pediatric Surgery Wards" Children 10, no. 7: 1089. https://doi.org/10.3390/children10071089