

Visual Analysis of Panoramic Radiographs among Pediatric Dental Residents Using Eye-Tracking Technology: A Cross-Sectional Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Participants and Stimuli
2.3. Eye-Tracking System and Measures
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
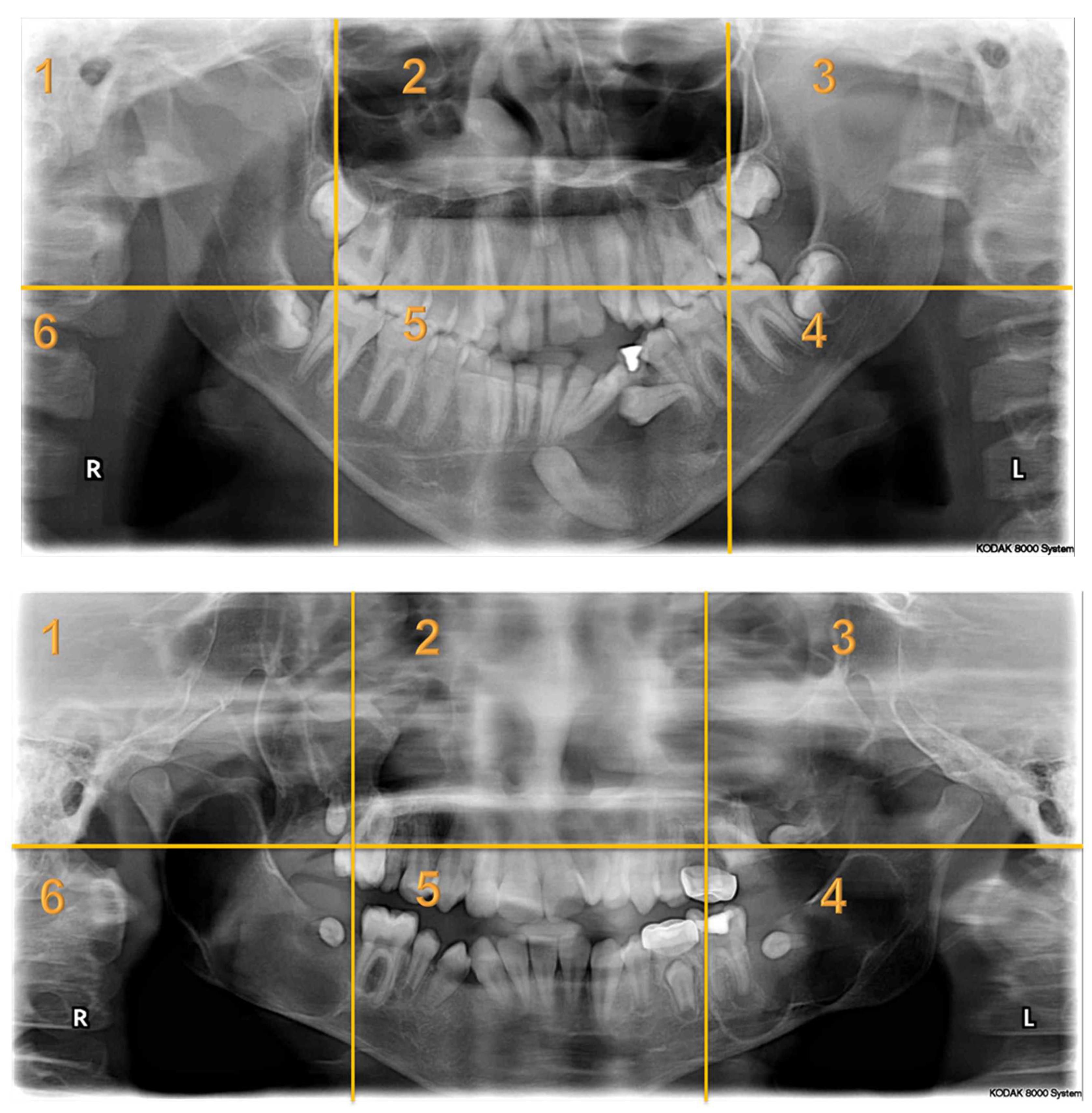
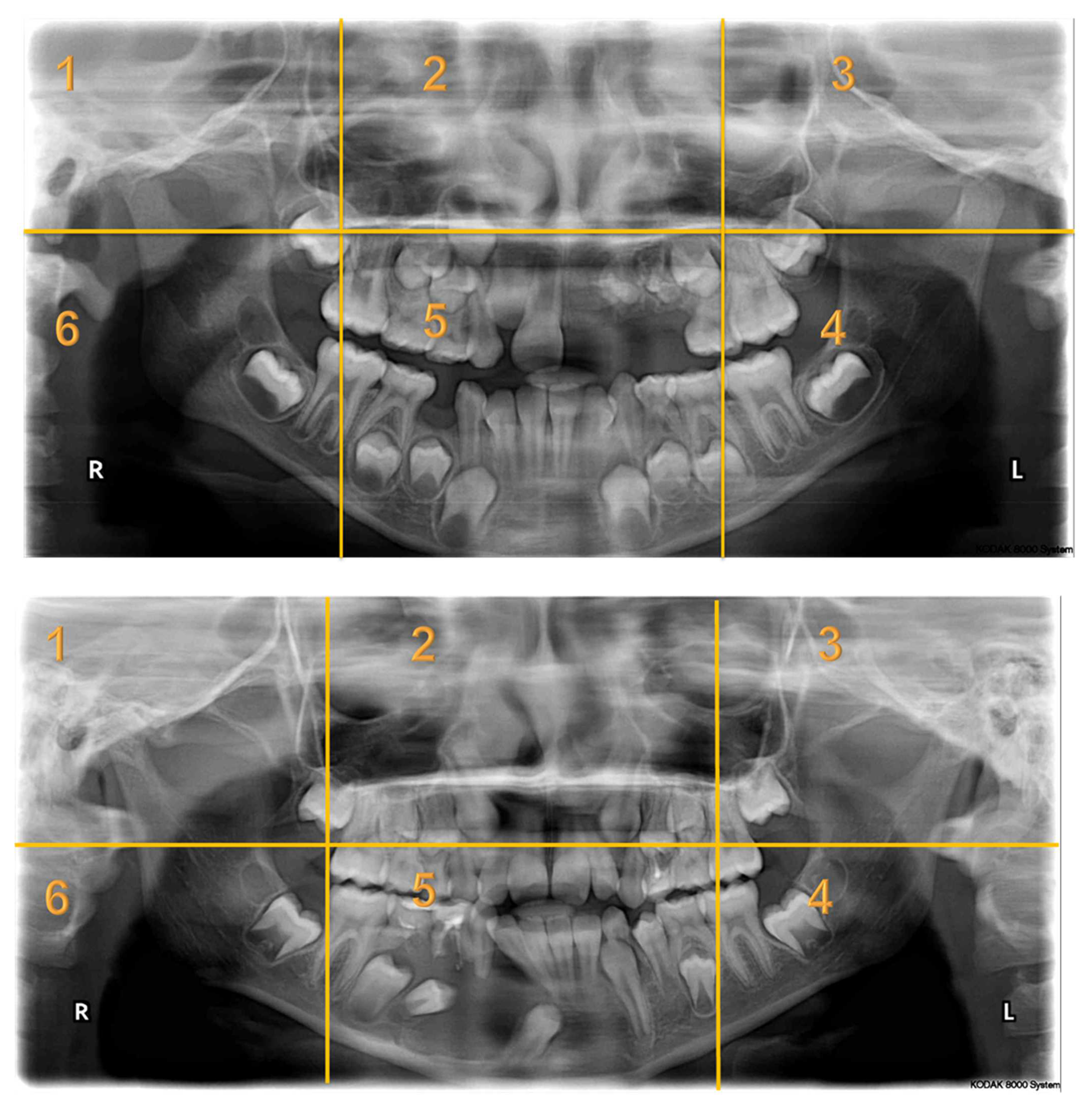
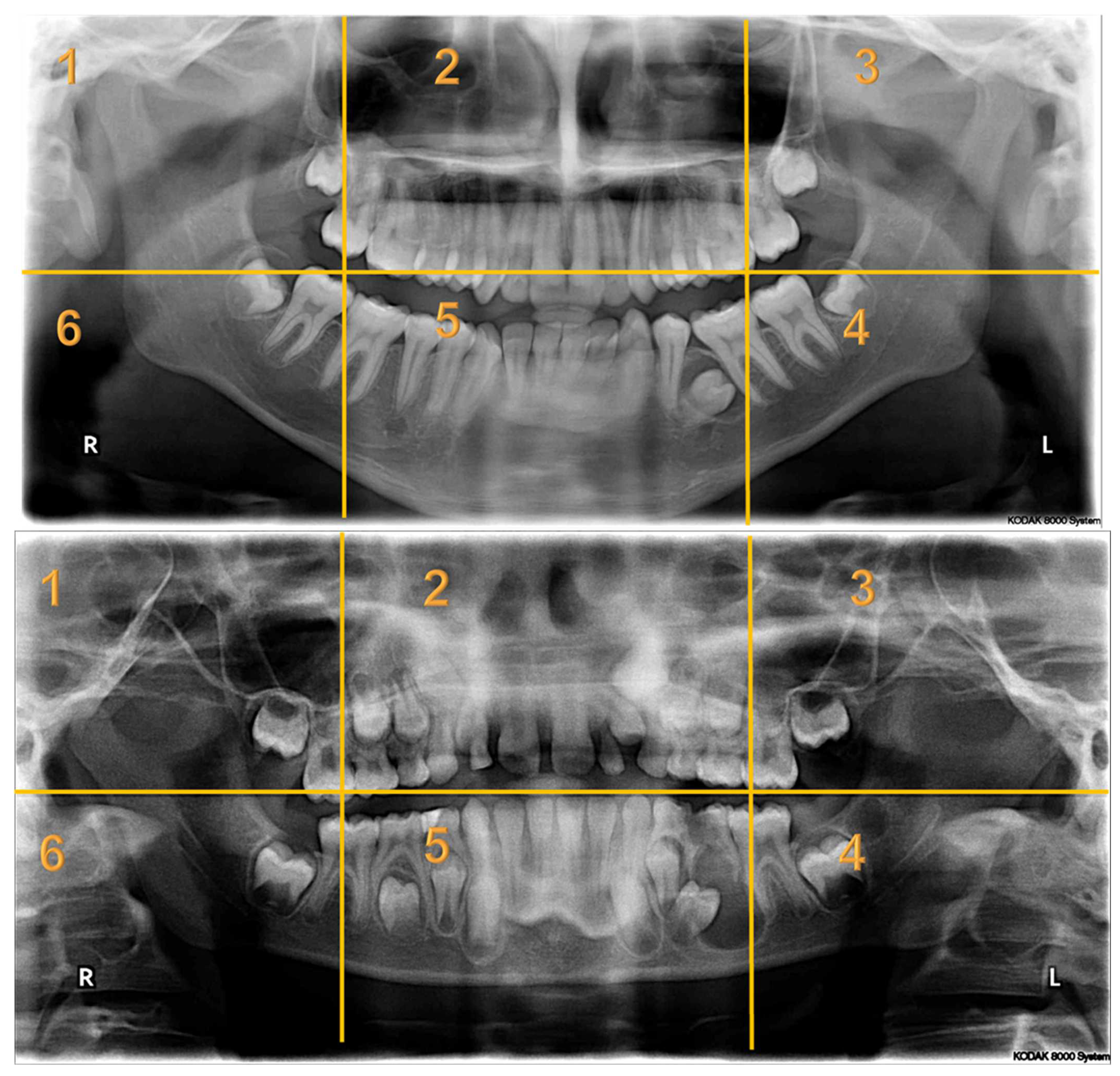
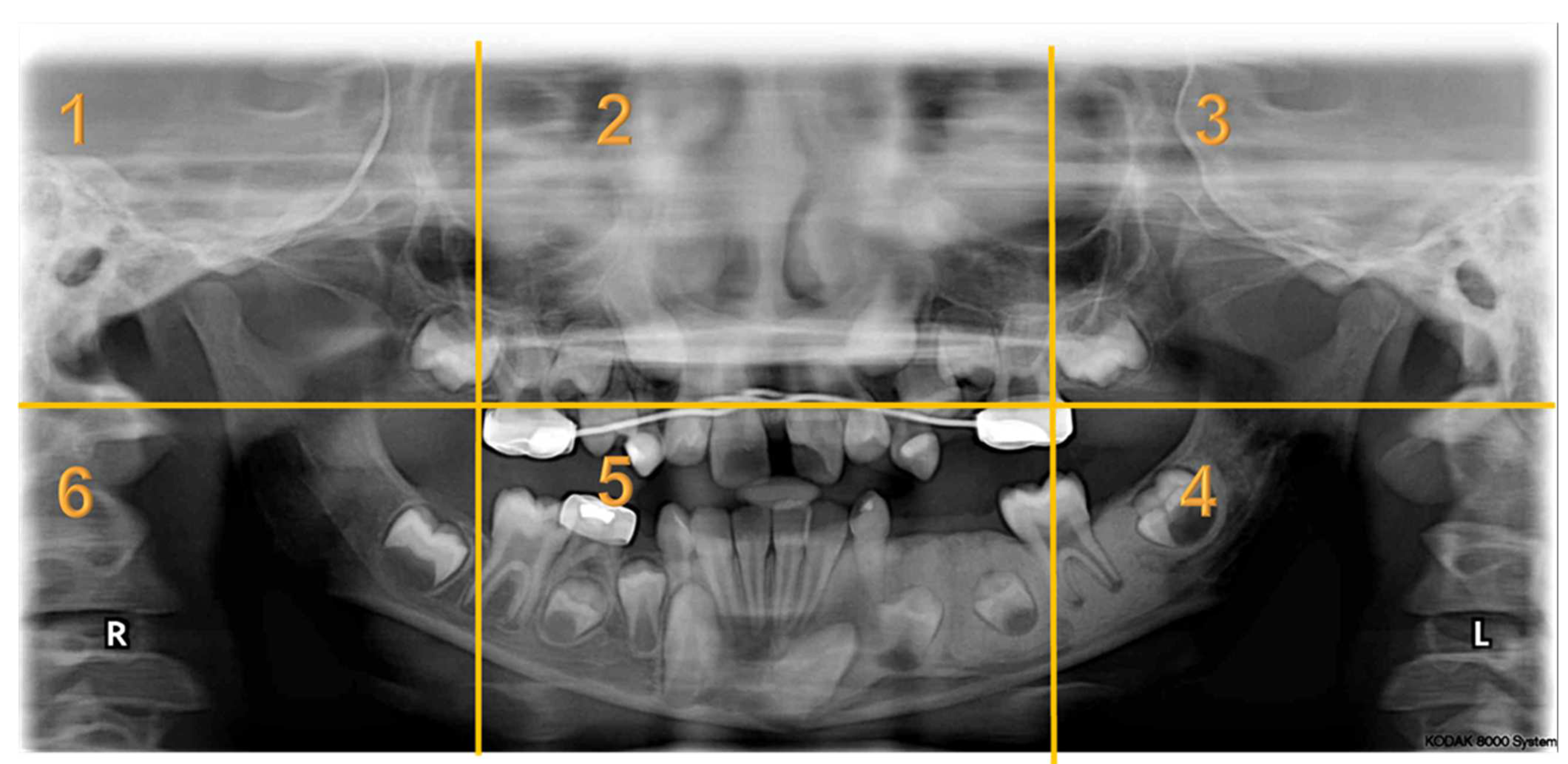
Appendix A. Radiographs Included in the Study
Appendix B. Instructions Prior to Commencing the Questionnaire
- The test will take around 15 to 20 min to be completed.
- You will start with a calibration process that takes less than a minute.
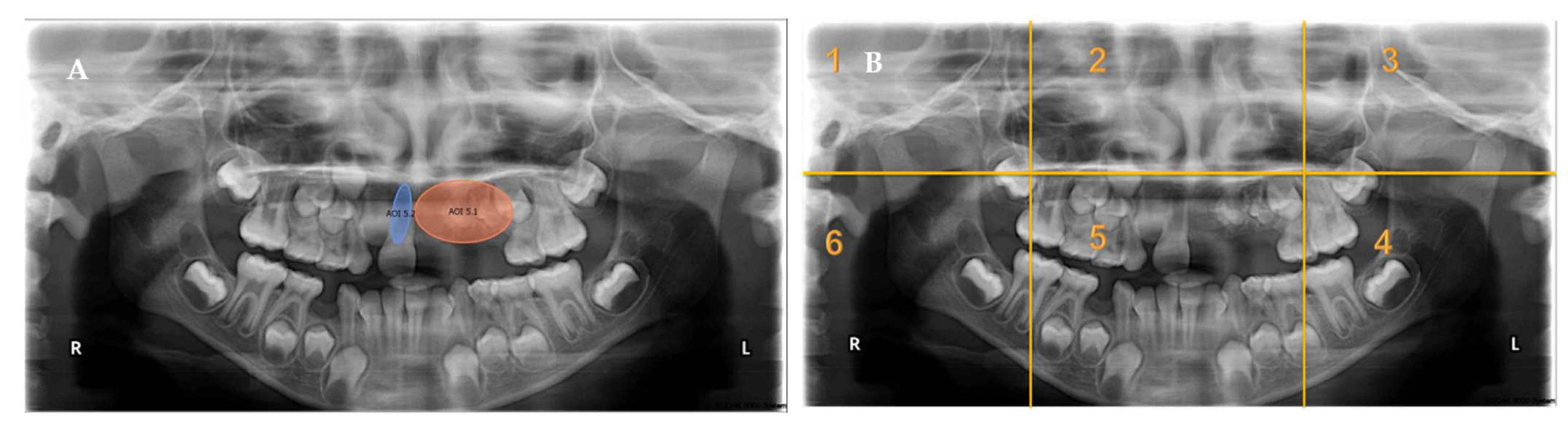
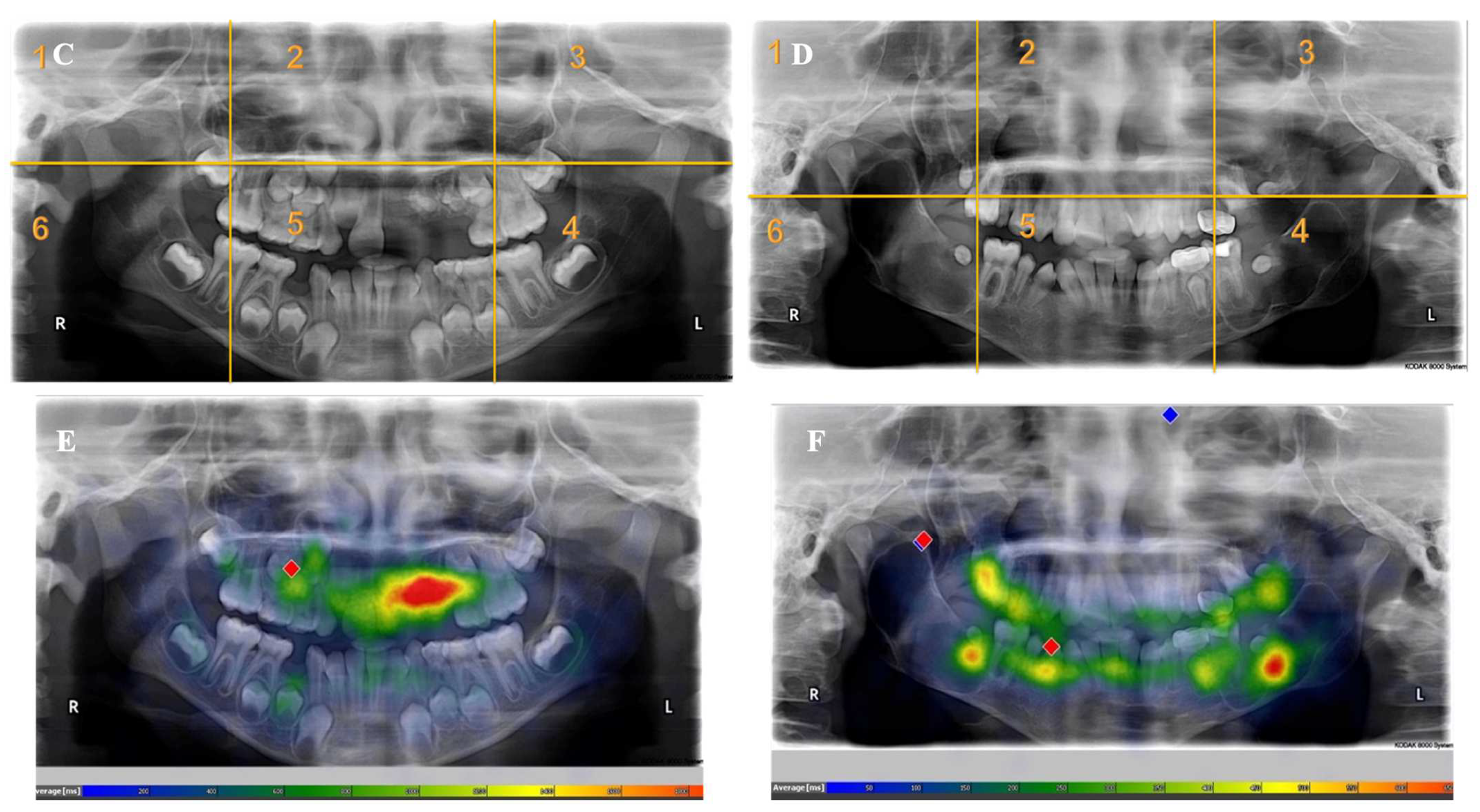
- Each panoramic radiograph displayed will be divided into sextants by yellow lines.
- The test contains seven cases, with three questions related to each case.
- Feel free to move to the next slide once the radiograph has been examined.
- This is a one-time test, and you cannot move backward on the slides.
- If you are wearing eyeglasses or lenses, or have had any kind of eye operation, please write them in the description box before starting the test.
- Clinical experience includes the internship year.
- You can press (F12) on the keyboard to exit the exam.
- Please do not share the questions after completing the test.
References
- Maeda, N.; Hosoki, H.; Yoshida, M.; Suito, H.; Honda, E. Dental students’ levels of understanding normal panoramic anatomy. J. Dent. Sci. 2018, 13, 374–377. [Google Scholar] [CrossRef]
- Razmus, T.F.; Williamson, G.F.; Van Dis, M.L. Assessment of the knowledge of graduating American dental students about the panoramic image. Oral Surg. Oral Med. Oral Pathol. 1993, 76, 397–402. [Google Scholar] [CrossRef]
- Gnanasekaran, F.; Nirmal, L.; Sujitha, P.; Bhavyaa, R.; Muthu, M.; Cho, V.Y.; King, N.M.; Anthonappa, R.P. Visual interpretation of panoramic radiographs in dental students using eye-tracking technology. J. Dent. Educ. 2022, 86, 887–892. [Google Scholar] [CrossRef]
- Kwong, J.W.; Cai, L.Z.; Azad, A.D.; Lorenz, H.P.; Khosla, R.K.; Lee, G.K.; Nazerali, R.S. Assessing the Fisher, Mohler, and Millard Techniques of Cleft Lip Repair Surgery With Eye-Tracking Technology. Ann. Plast. Surg. 2019, 82, S313–S319. [Google Scholar] [CrossRef] [PubMed]
- Vogel, D.; Schulze, R. Viewing patterns regarding panoramic radiographs with different pathological lesions: An eye-tracking study. Dentomaxillofacial Radiol. 2021, 50, 20210019. [Google Scholar] [CrossRef] [PubMed]
- Cho, V.Y.; Loh, X.H.; Abbott, L.; Mohd-Isa, N.A.; Anthonappa, R.P. Reporting Eye-tracking Studies In DEntistry (RESIDE) checklist. J. Dent. 2023, 129, 104359. [Google Scholar] [CrossRef] [PubMed]
- Crowe, E.M.; Gilchrist, I.D.; Kent, C. New approaches to the analysis of eye movement behaviour across expertise while viewing brain MRIs. Cogn. Res. Princ. Implic. 2018, 3, 12. [Google Scholar] [CrossRef]
- Oyama, A.; Takeda, S.; Ito, Y.; Nakajima, T.; Takami, Y.; Takeya, Y.; Yamamoto, K.; Sugimoto, K.; Shimizu, H.; Shimamura, M.; et al. Novel Method for Rapid Assessment of Cognitive Impairment Using High-Performance Eye-Tracking Technology. Sci. Rep. 2019, 9, 12932. [Google Scholar] [CrossRef]
- Asaad, M.; Dey, J.K.; Al-Mouakeh, A.; Manjouna, M.B.; Nashed, M.A.; Rajesh, A.; Boonipat, T.; Bite, U. Eye-Tracking Technology in Plastic and Reconstructive Surgery: A Systematic Review. Aesthetic Surg. J. 2020, 40, 1022–1034. [Google Scholar] [CrossRef]
- Gil, A.M.; Birdi, S.; Kishibe, T.; Grantcharov, T.P. Eye Tracking Use in Surgical Research: A Systematic Review. J. Surg. Res. 2022, 279, 774–787. [Google Scholar] [CrossRef]
- Hartmann, G.C.; Guimarães, L.K.; Maggioni, C.G.; Gasparello, G.G.; Júnior, S.L.M.; Pithon, M.M.; Tanaka, O.M. Social attractiveness perception of a cleft lip repair in an adolescent via eye-tracking. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e526–e532. [Google Scholar] [CrossRef] [PubMed]
- Kawagoe, T.; Matsushita, M.; Hashimoto, M.; Ikeda, M.; Sekiyama, K. Face-specific memory deficits and changes in eye scanning patterns among patients with amnestic mild cognitive impairment. Sci. Rep. 2017, 7, 14344. [Google Scholar] [CrossRef]
- Zhang, J.; Troulis, M.J.; August, M. Diagnosis and Treatment of Pediatric Primary Jaw Lesions at Massachusetts General Hospital. J. Oral Maxillofac. Surg. 2021, 79, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Oreamuno, Y.V.B.; Soto, A.L. Clinical and Histopathological Concordance of oral Bone Lesions. Retrospective Study. Odovtos-Int. J. Dent. Sci. 2020, 22, 163–173. [Google Scholar]
- Cholitgul, W.; Drummond, B.K. Jaw and tooth abnormalities detected on panoramic radiographs in New Zealand children aged 10-15 years. N. Z. Dent. J. 2000, 96, 10–13. [Google Scholar] [PubMed]
- Dentistry, A.A.O.P. Prescribing dental radiographs for infants, children, adolescents, and individuals with special health care needs. Pediatr. Dent. 2018, 40, 213. [Google Scholar]
- Kok, E.M.; Jarodzka, H.; de Bruin, A.B.; BinAmir, H.A.; Robben, S.G.; van Merriënboer, J.J. Systematic viewing in radiology: Seeing more, missing less? Adv. Health Sci. Educ. Theory Pract. 2016, 21, 189–205. [Google Scholar] [CrossRef]
- Alsufyani, N.; Alnamlah, S.; Mutaieb, S.; Alageel, R.; AlQarni, M.; Bukhari, A.; Alhajri, M.; AlSubaie, A.; Alabdulkarim, M.; Faden, A. Virtual reality simulation of panoramic radiographic anatomy for dental students. J. Dent. Educ. 2023, 87, 1200–1209. [Google Scholar] [CrossRef]
- Ayekinam, K.; Saliha, C.; Wafaa, E. Surgical management of oroantral fistula due to dental procedures-two case reports. Asian Pac. J. Health Sci. 2018, 5, 85–90. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- Tee, Q.X.; Nambiar, M.; Stuckey, S. Error and cognitive bias in diagnostic radiology. J. Med. Imaging Radiat. Oncol. 2022, 66, 202–207. [Google Scholar] [CrossRef]
- Harezlak, K.; Kasprowski, P. Application of eye tracking in medicine: A survey, research issues and challenges. Comput. Med. Imaging Graph. 2018, 65, 176–190. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.R.; Brooks, L.R.; Colle, C.L.; Hatala, R.M. The benefit of diagnostic hypotheses in clinical reasoning: Experimental study of an instructional intervention for forward and backward reasoning. Cogn. Instr. 1999, 17, 433–448. [Google Scholar] [CrossRef]
- Matsumoto, H.; Terao, Y.; Yugeta, A.; Fukuda, H.; Emoto, M.; Furubayashi, T.; Okano, T.; Hanajima, R.; Ugawa, Y. Where do neurologists look when viewing brain CT images? An eye-tracking study involving stroke cases. PLoS ONE 2011, 6, e28928. [Google Scholar] [CrossRef]
- Ganesan, A.; Alakhras, M.; Brennan, P.C.; Mello-Thoms, C. A review of factors influencing radiologists’ visual search behaviour. J. Med. Imaging Radiat. Oncol. 2018, 62, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Mello-Thoms, C.; Trieu, P.D.; Brennan, P.C. Going on with false beliefs: What if satisfaction of search was really suppression of recognition? In Proceedings of Medical Imaging 2014: Image Perception, Observer Performance, and Technology Assessment; SPIE: Bellingham, WA, USA, 2014; pp. 46–52. [Google Scholar]
- Huynh, J.D.; Rhodes, S.C.; Hatton, J.F.; Khademi, J.A. Satisfaction of Search in Periapical Radiograph Interpretation. J. Endod. 2021, 47, 291–296. [Google Scholar] [CrossRef]
- Celine, G.; Cho, V.; Kogan, A.; Anthonappa, R.; King, N. Eye-tracking in dentistry: What do children notice in the dentist? J. Dent. 2018, 78, 72–75. [Google Scholar] [CrossRef]
- Perschbacher, S. Interpretation of panoramic radiographs. Aust. Dent. J. 2012, 57 (Suppl. 1), 40–45. [Google Scholar] [CrossRef]
- Tanaka, S.; Karibe, H.; Kato, Y.; Komatsuzaki, A.; Sekimoto, T.; Shimomura-Kuroki, J. Evaluation of eye movement patterns during reading of mixed dentition panoramic radiographs in dental students. Pediatr. Dent. J. 2023, 33, 33–41. [Google Scholar] [CrossRef]
- Radianti, J.; Majchrzak, T.A.; Fromm, J.; Wohlgenannt, I. A systematic review of immersive virtual reality applications for higher education: Design elements, lessons learned, and research agenda. Comput. Educ. 2020, 147, 103778. [Google Scholar] [CrossRef]
- Adhanom, I.B.; MacNeilage, P.; Folmer, E. Eye Tracking in virtual reality: A broad review of applications and challenges. Virtual Real. 2023, 27, 1481–1505. [Google Scholar] [CrossRef] [PubMed]
- Donmez, M. A systematic literature review for the use of eye-tracking in special education. Educ. Inf. Technol. 2023, 28, 6515–6540. [Google Scholar] [CrossRef]
- García-Baos, A.; D’Amelio, T.; Oliveira, I.; Collins, P.; Echevarria, C.; Zapata, L.P.; Liddle, E.; Supèr, H. Novel Interactive Eye-Tracking Game for Training Attention in Children With Attention-Deficit/Hyperactivity Disorder. Prim. Care Companion CNS Disord. 2019, 21, 22cr03477. [Google Scholar] [CrossRef]
- Lee, T.L.; Yeung, M.K.; Sze, S.L.; Chan, A.S. Computerized Eye-Tracking Training Improves the Saccadic Eye Movements of Children with Attention-Deficit/Hyperactivity Disorder. Brain Sci. 2020, 10, 1016. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Radiographs with Abnormalities | Number of Sextants Involved | Number of AOI a | Number of Participants | Total Recorded Observation b |
|---|---|---|---|---|
| Radiograph 1 | Multiple | 3 | 30 | 90 |
| Radiograph 2 | Multiple | 8 | 30 | 240 |
| Radiograph 3 | Single | 2 | 30 | 60 |
| Radiograph 4 | Single | 2 | 30 | 60 |
| Radiograph 5 | Single | 1 | 30 | 30 |
| Radiograph 6 | Single | 1 | 30 | 30 |
| Radiograph 7 | Single | 1 | 30 | 30 |
| Overall Observations | 540 |
| Participants’ Characteristics | n (%) |
|---|---|
| Pediatric Postgraduate | |
| Dental Students | |
| Overall | 30 (100) |
| Sex | |
| Female | 22 (73.3) |
| Male | 8 (26.7) |
| Age Categories (Years) | |
| 20–25 | 0 (0.0) |
| 26–30 | 20 (66.7) |
| 31–35 | 7 (23.3) |
| 36–40 | 3 (10.0) |
| Clinical Experience (Including Internship Year) | |
| 1 year or less | 0 (0.0) |
| 2–4 years | 17 (56.7) |
| 5 or more years | 13 (43.3) |
| Eye Tracking Measures | Median Score (25th–75th IQR) | Mann–Whitney U Test Test Statistic [p-Value *] | ||
|---|---|---|---|---|
| Overall | AOIs Located in One Sextant | AOIs Located in Multiple Sextants | ||
| Revisit Count (Frequency Count) | 4 (1–8) | 5 (3–10) | 2 (0.5–5) | 7.338 [<0.001] |
| Fixation Count (Frequency Count) | 4 (0–11) | 9 (4–20) | 1 (0–6) | 10.273 [<0.001] |
| Entry Time (Milliseconds) | 3551.9 (1073.3–11,721.4) | 2878 (941.4–11,062.7) | 4000.1 (1227–13,907.25) | −1.918 [0.055] |
| Fixation Time (Milliseconds) | 1389.15 (0–3591.9) | 2736.8 (1335–6040.6) | 550.7 (0–2269.3) | 9.740 [<0.001] |
| Dwell Time (Milliseconds) | 1414.15 (0–3696.35) | 2820.35 (1335–6207.5) | 550.7 (0–2286.1) | 9.782 [<0.001] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhadila, G.Y.; Alsharif, S.I.; Almarei, S.; Almashaikhi, J.A.; Bahdila, D. Visual Analysis of Panoramic Radiographs among Pediatric Dental Residents Using Eye-Tracking Technology: A Cross-Sectional Study. Children 2023, 10, 1476. https://doi.org/10.3390/children10091476
Bhadila GY, Alsharif SI, Almarei S, Almashaikhi JA, Bahdila D. Visual Analysis of Panoramic Radiographs among Pediatric Dental Residents Using Eye-Tracking Technology: A Cross-Sectional Study. Children. 2023; 10(9):1476. https://doi.org/10.3390/children10091476
Chicago/Turabian StyleBhadila, Ghalia Y., Safiya I. Alsharif, Seba Almarei, Jamila A. Almashaikhi, and Dania Bahdila. 2023. "Visual Analysis of Panoramic Radiographs among Pediatric Dental Residents Using Eye-Tracking Technology: A Cross-Sectional Study" Children 10, no. 9: 1476. https://doi.org/10.3390/children10091476
APA StyleBhadila, G. Y., Alsharif, S. I., Almarei, S., Almashaikhi, J. A., & Bahdila, D. (2023). Visual Analysis of Panoramic Radiographs among Pediatric Dental Residents Using Eye-Tracking Technology: A Cross-Sectional Study. Children, 10(9), 1476. https://doi.org/10.3390/children10091476