Parents’ Knowledge of and Attitude toward Acute Otitis Media and Its Treatment in Children: A Survey at Primary Healthcare Centers in the Aseer Region

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Setting
2.2. Study Population and Sample Size
2.3. Study Outcome
2.4. Study Questionnaires and Data Collection
2.5. Questionnaire Validation
2.6. Ethical Apporval and Consent
2.7. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Parents and Children
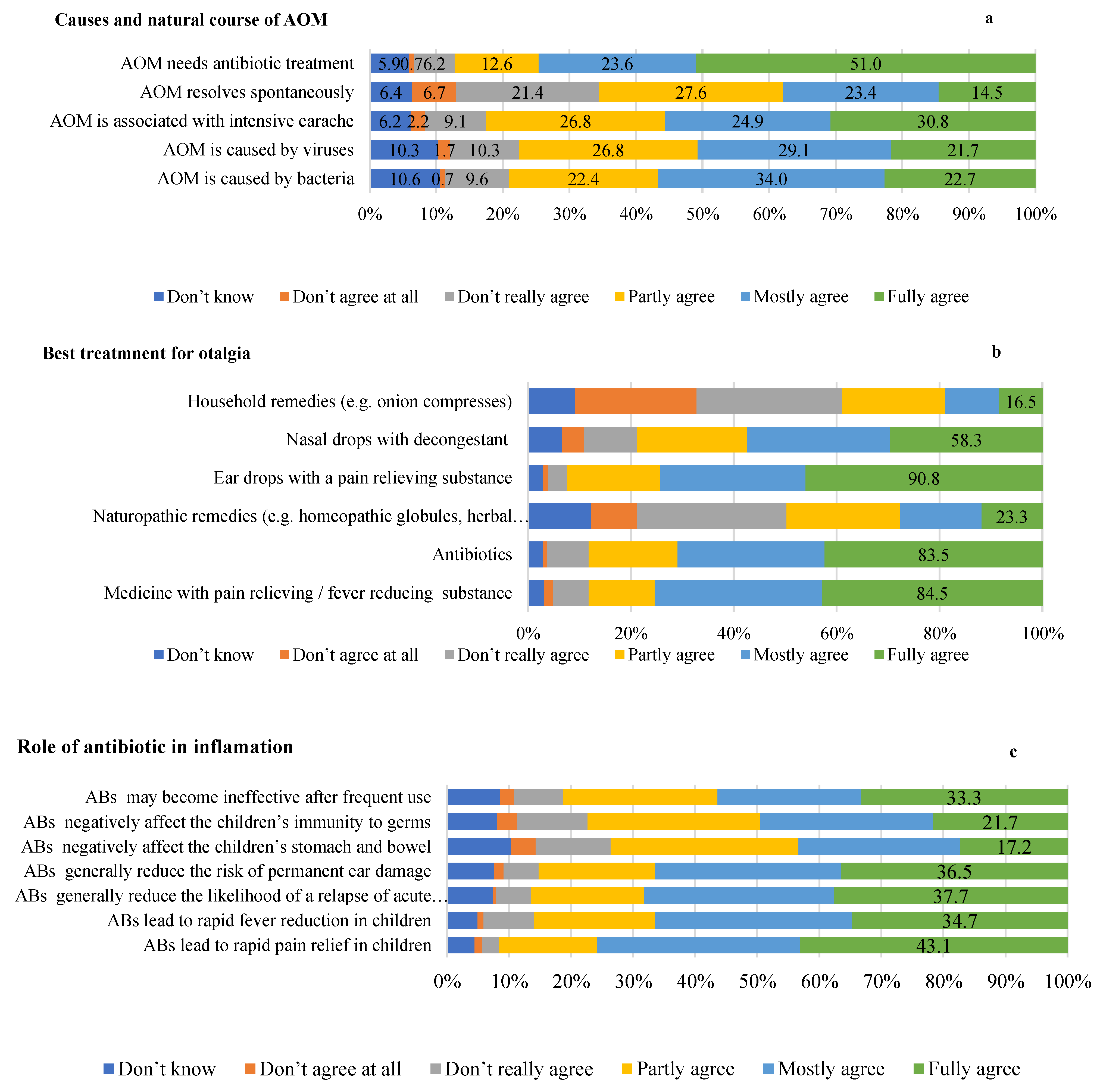
3.2. Parental Knowledge of Otitis Media
3.3. Parental Attitudes towards Otitis Media
3.4. Parent’s Experience with Acute Otitis Media
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schilder, A.G.M.; Chonmaitree, T.; Cripps, A.W.; Rosenfeld, R.M.; Casselbrant, M.L.; Haggard, M.P.; Venekamp, R.P. Otitis media. Nat. Rev. Dis. Primers 2016, 2, 16063. [Google Scholar] [CrossRef] [PubMed]
- Monasta, L.; Ronfani, L.; Marchetti, F.; Montico, M.; Vecchi Brumatti, L.; Bavcar, A.; Grasso, D.; Barbiero, C.; Tamburlini, G. Burden of disease caused by otitis media: Systematic review and global estimates. PLoS ONE 2012, 7, e36226. [Google Scholar] [CrossRef] [PubMed]
- Pichichero, M.E. Otitis media. Pediatr. Clin. N. Am. 2013, 60, 391–407. [Google Scholar] [CrossRef]
- Rosenfeld, R.M.; Shin, J.J.; Schwartz, S.R.; Coggins, R.; Gagnon, L.; Hackell, J.M.; Hoelting, D.; Hunter, L.L.; Kummer, A.W.; Payne, S.C. Clinical practice guideline: Otitis media with effusion (update). Otolaryngol.–Head Neck Surg. 2016, 154, S1–S41. [Google Scholar] [CrossRef] [PubMed]
- Verhoeff, M.; Van Der Veen, E.L.; Rovers, M.M.; Sanders, E.A.; Schilder, A.G. Chronic suppurative otitis media: A review. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1–12. [Google Scholar] [CrossRef]
- Kørvel-Hanquist, A.; Koch, A.; Lous, J.; Olsen, S.F.; Homøe, P. Risk of childhood otitis media with focus on potentially modifiable factors: A Danish follow-up cohort study. Int. J. Pediatr. Otorhinolaryngol. 2018, 106, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aldè, M.; Di Berardino, F.; Marchisio, P.; Cantarella, G.; Ambrosetti, U.; Consonni, D.; Zanetti, D. Effects of COVID-19 lockdown on otitis media with effusion in children: Future therapeutic implications. Otolaryngol.–Head Neck Surg. 2021, 165, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Mukara, K.B.; Waiswa, P.; Lilford, R.; Tucci, D.L. Knowledge and care seeking practices for ear infections among parents of under five children in Kigali, Rwanda: A cross-sectional study. BMC Ear Nose Throat Disord. 2017, 17, 7. [Google Scholar] [CrossRef]
- Dabholkar, Y.G.; Wadhwa, A.; Deshmukh, A. A study of knowledge, attitude and practices about otitis media in parents in Navi-Mumbai. J. Otol. 2021, 16, 89–94. [Google Scholar] [CrossRef]
- DeAntonio, R.; Yarzabal, J.-P.; Cruz, J.P.; Schmidt, J.E.; Kleijnen, J. Epidemiology of otitis media in children from developing countries: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2016, 85, 65–74. [Google Scholar] [CrossRef]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed]
- Kung, K.; Wong, C.K.M.; Wong, S.Y.S.; Lam, A.; Chan, C.K.Y.; Griffiths, S.; Butler, C. Patient presentation and physician management of upper respiratory tract infections: A retrospective review of over 5 million primary clinic consultations in Hong Kong. BMC Fam. Pract. 2014, 15, 95. [Google Scholar] [CrossRef]
- Alsuhaibani, M.; Almijmaj, M.; Almushaigeh, A.; Alhomidani, R.; Aldakheel, Y.; Alaqeel, A. Awareness and attitudes of Saudi parents toward otitis media in children. J. Fam. Med. Prim. Care 2020, 9, 6177–6182. [Google Scholar] [CrossRef]
- Yin, H.S.; Dreyer, B.P.; Vivar, K.L.; MacFarland, S.; van Schaick, L.; Mendelsohn, A.L. Perceived barriers to care and attitudes towards shared decision-making among low socioeconomic status parents: Role of health literacy. Acad. Pediatr. 2012, 12, 117–124. [Google Scholar] [CrossRef]
- Zakzouk, S.M.; Jamal, T.S.; Daghistani, K.J. Epidemiology of acute otitis media among Saudi children. Int. J. Pediatr. Otorhinolaryngol. 2002, 62, 219–222. [Google Scholar] [CrossRef]
- Al-Hammar, A.E.; Albrahim, N.M.; AlAli, F.B.; AlHabeeb, Z.A.; Al-Hammar, L.; AlYahya, K.A.; AlJarudi, S.H. Awareness of otitis media risk factors in children among Saudi population in Al-Ahsa. Egypt. J. Hosp. Med. 2018, 70, 1936–1942. [Google Scholar] [CrossRef]
- Kautz-Freimuth, S.; Redaèlli, M.; Samel, C.; Civello, D.; Altin, S.V.; Stock, S. Parental views on acute otitis media (AOM) and its therapy in children-results of an exploratory survey in German childcare facilities. BMC Pediatr. 2015, 15, 199. [Google Scholar] [CrossRef] [PubMed]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Barber, C.; Ille, S.; Vergison, A.; Coates, H. Acute otitis media in young children–what do parents say? Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Venekamp, R.P.; Sanders, S.L.; Glasziou, P.P.; Del Mar, C.B.; Rovers, M.M. Antibiotics for acute otitis media in children. Cochrane Database Syst. Rev. 2015, 2015, CD000219. [Google Scholar] [CrossRef]
- Finkelstein, J.A.; Dutta-Linn, M.; Meyer, R.; Goldman, R. Childhood infections, antibiotics, and resistance: What are parents saying now? Clin. Pediatr. 2014, 53, 145–150. [Google Scholar] [CrossRef]
- Panagakou, S.G.; Spyridis, Ν.; Papaevangelou, V.; Theodoridou, K.M.; Goutziana, G.P.; Theodoridou, M.N.; Syrogiannopoulos, G.A.; Hadjichristodoulou, C.S. Antibiotic use for upper respiratory tract infections in children: A cross-sectional survey of knowledge, attitudes, and practices (KAP) of parents in Greece. BMC Pediatr. 2011, 11, 60. [Google Scholar] [CrossRef]
- André, M.; Vernby, Å.; Berg, J.; Lundborg, C.S. A survey of public knowledge and awareness related to antibiotic use and resistance in Sweden. J. Antimicrob. Chemother. 2010, 65, 1292–1296. [Google Scholar] [CrossRef]
- Nokso-Koivisto, J.; Hovi, T.; Pitkäranta, A. Viral upper respiratory tract infections in young children with emphasis on acute otitis media. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1333–1342. [Google Scholar] [CrossRef]
- Thomas, J.P.; Berner, R.; Zahnert, T.; Dazert, S. Strukturiertes Vorgehen bei akuter Otitis media. Dtsch. Arztebl. Int. 2014, 111, 151–160. [Google Scholar]
- McNulty, C.A.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. Don’t wear me out—The public’s knowledge of and attitudes to antibiotic use. J. Antimicrob. Chemother. 2007, 59, 727–738. [Google Scholar] [CrossRef]
- Tähtinen, P.A.; Boonacker, C.W.; Rovers, M.M.; Schilder, A.G.; Huovinen, P.; Liuksila, P.-R.; Ruuskanen, O.; Ruohola, A. Parental experiences and attitudes regarding the management of acute otitis media—A comparative questionnaire between Finland and The Netherlands. Fam. Pract. 2009, 26, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Glaeske, G.; Hoffmann, F.; Koller, D.; Tholen, K.; Windt, R. Faktencheck Gesundheit. Antibiotika-Verordnungen bei Kindern; University of Bremen: Bremen, Germany, 2012; Available online: https://faktencheck-gesundheit.de/fileadmin/files/BSt/Publikationen/GrauePublikationen/GP_Faktencheck_Gesundheit_Antibiotika.pdf (accessed on 22 August 2023).
- Suarez-Lledo, V.; Alvarez-Galvez, J. Prevalence of Health Misinformation on Social Media: Systematic Review. J. Med. Internet Res. 2021, 23, e17187. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, N. Internet and information technology use in treatment of diabetes. Int. J. Clin. Pract. 2010, 64, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, Q. Social Media Use, eHealth Literacy, Disease Knowledge, and Preventive Behaviors in the COVID-19 Pandemic: Cross-Sectional Study on Chinese Netizens. J. Med. Internet Res. 2020, 22, e19684. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 406 | Variables | ||
|---|---|---|---|
| Parents criteria | Gender | Female | 263 (64.8%) |
| Male | 143 (35.2%) | ||
| Age | From 18 to 24 years | 26 (6.4%) | |
| From 25 to 34 years | 184 (45.3%) | ||
| From 35 to 44 years | 162 (39.9%) | ||
| From 45 to 54 years | 27 (6.7%) | ||
| From 55 to 64 years | 7 (1.7%) | ||
| Residence | Rural | 40 (9.9%) | |
| Urban | 366 (90.1%) | ||
| Education | Below university | 113 (27.8%) | |
| University | 293 (72.2%) | ||
| Child criteria | Health insurance | Governmental | 206 (50.7%) |
| Private | 43 (10.6%) | ||
| None | 157 (38.7%) | ||
| Age child | Below one year | 54 (13.3%) | |
| One year | 60 (14.8%) | ||
| Two years | 52 (12.8%) | ||
| Three years | 73 (18.0%) | ||
| Four years | 80 (19.7%) | ||
| Five years | 87 (21.4%) | ||
| Attend nursery | 55(13.5%) | ||
| Use a pacifiers | 66(13.5%) | ||
| Dependent: | Did Not Experience AOM | Experienced AOM | p | |
|---|---|---|---|---|
| Antibiotics negatively affect children’s immunity to germs. | Don’t know | 28 (8.8) | 5 (5.8) | 0.029 |
| Don’t agree at all | 13 (4.1) | 0 (0.0) | ||
| Don’t really agree | 31 (9.7) | 15 (17.4) | ||
| Partly agree | 95 (29.7) | 18 (20.9) | ||
| Mostly agree | 90 (28.1) | 23 (26.7) | ||
| Fully agree | 63 (19.7) | 25 (29.1) | ||
| I am not willing to wait and use antibiotics immediately because I am concerned that the disease could get worse. | Don’t know | 16 (5.0) | 0 (0.0) | 0.008 |
| Don’t agree at all | 21 (6.6) | 7 (8.1) | ||
| Don’t really agree | 55 (17.2) | 9 (10.5) | ||
| Partly agree | 65 (20.3) | 29 (33.7) | ||
| Mostly agree | 75 (23.4) | 12 (14.0) | ||
| Fully agree | 88 (27.5) | 29 (33.7) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlHefdhi, H.A.; Al Qout, M.M.; Alqahtani, A.Y.; Alqahtani, M.M.; Asiri, R.M.; Alshahrani, O.M.; Almoghamer, H.D.; Youssef, N.; Ghazy, R.M. Parents’ Knowledge of and Attitude toward Acute Otitis Media and Its Treatment in Children: A Survey at Primary Healthcare Centers in the Aseer Region. Children 2023, 10, 1573. https://doi.org/10.3390/children10091573
AlHefdhi HA, Al Qout MM, Alqahtani AY, Alqahtani MM, Asiri RM, Alshahrani OM, Almoghamer HD, Youssef N, Ghazy RM. Parents’ Knowledge of and Attitude toward Acute Otitis Media and Its Treatment in Children: A Survey at Primary Healthcare Centers in the Aseer Region. Children. 2023; 10(9):1573. https://doi.org/10.3390/children10091573
Chicago/Turabian StyleAlHefdhi, Hayfa Abdulkhaleq, Maraam Mohammed Al Qout, Alhanouf Yahya Alqahtani, Meshal Mohammed Alqahtani, Roaa Mohammed Asiri, Omair Mohammed Alshahrani, Hanan Delem Almoghamer, Naglaa Youssef, and Ramy Mohamed Ghazy. 2023. "Parents’ Knowledge of and Attitude toward Acute Otitis Media and Its Treatment in Children: A Survey at Primary Healthcare Centers in the Aseer Region" Children 10, no. 9: 1573. https://doi.org/10.3390/children10091573
APA StyleAlHefdhi, H. A., Al Qout, M. M., Alqahtani, A. Y., Alqahtani, M. M., Asiri, R. M., Alshahrani, O. M., Almoghamer, H. D., Youssef, N., & Ghazy, R. M. (2023). Parents’ Knowledge of and Attitude toward Acute Otitis Media and Its Treatment in Children: A Survey at Primary Healthcare Centers in the Aseer Region. Children, 10(9), 1573. https://doi.org/10.3390/children10091573