
Using Virtual Reality Interventions to Promote Social and Emotional Learning for Children and Adolescents: A Systematic Review and Meta-Analysis




Abstract
:
1. Introduction
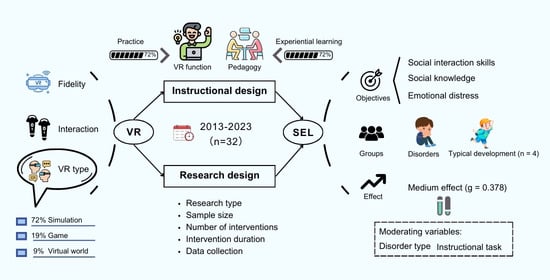
- Which groups were primarily targeted when using VR to promote SEL?
- What are the technical features of VR that support SEL for children and adolescents?
- What types of social and emotional skills for children and adolescents were taught in VR?
- What are the overall effects and possible moderating factors of VR-supported SEL interventions?
2. Methods
2.1. Search Procedure
2.2. Screening Procedure
2.3. Coding Procedure
3. Results
3.1. Participant Characteristics
3.2. Research Design
3.3. Technological Features
3.4. Instructional Design
3.5. Meta-Analysis Results
4. Conclusions and Implications
4.1. Conclusions
4.2. Practical Implications
4.3. Research Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fundamentals of SEL. Available online: https://casel.org/fundamentals-of-sel/ (accessed on 15 November 2023).
- Wang, Y.; Yang, Z.; Zhang, Y.; Wang, F.; Liu, T.; Xin, T. The effect of social-emotional competency on child development in Western China. Front. Psychol. 2019, 10, 1282. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Cheung, A.C.K. The impacts of a social emotional learning program on elementary school students in China: A quasi-experimental study. Asia-Pac. Edu. Res. 2022. [Google Scholar] [CrossRef]
- Kondrla, P.; Maturkanič, P.; Taraj, M.; Kurilenko, V. Philosophy of Education in Postmetaphysical Thinking. J. Educ. Cult. Soc. 2022, 13, 19–30. [Google Scholar] [CrossRef]
- Kondrla, P.; Lojan, R.; Maturkanič, P.; Biryukova, Y.; Gonzalez Mastrapa, E. The Philosophical Context of Curriculum Innovations with a Focus on Competence Development. J. Educ. Cult. Soc. 2023, 14, 78–92. [Google Scholar] [CrossRef]
- Jones, D.E.; Greenberg, M.; Crowley, M. Early social-emotional functioning and public health: The relationship between kindergarten social competence and future wellness. Am. J. Public Health 2015, 105, 2283–2290. [Google Scholar] [CrossRef]
- Dahl, R.E. Adolescent brain development: A period of vulnerabilities and opportunities. Keynote address. Ann. N. Y. Acad. Sci. 2004, 1021, 1–22. [Google Scholar] [CrossRef]
- Dowling, K.; Simpkin, A.J.; Barry, M.M. A cluster randomized-controlled trial of the mindout social and emotional learning program for disadvantaged post-primary school students. J. Youth Adolesc. 2019, 48, 1245–1263. [Google Scholar] [CrossRef]
- Weare, K.; Nind, M. Mental health promotion and problem prevention in schools: What does the evidence say? Health Promot. Int. 2011, 26, i29–i69. [Google Scholar] [CrossRef]
- Zins, J.E.; Weissberg, R.P.; Walberg, H.J.; Wang, M.C. Building School Success through Social and Emotional Learning; Teachers College Press: New York, NY, USA, 2004. [Google Scholar]
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef]
- Králik, R. The Influence of Family and School in Shaping the Values of Children and Young People in the Theory of Free Time and Pedagogy. J. Educ. Cult. Soc. 2023, 14, 249–268. [Google Scholar] [CrossRef]
- Xiong, J.; Hsiang, E.-L.; He, Z.; Zhan, T.; Wu, S.-T. Augmented reality and virtual reality displays: Emerging technologies and future perspectives. Light Sci. Appl. 2021, 10, 216. [Google Scholar] [CrossRef] [PubMed]
- Anthes, C.; Garcia-Hernandez, R.J.; Wiedemann, M.; Kranzlmuller, D. State of the art of virtual reality technology. In Proceedings of the 2016 IEEE Aerospace Conference, Big Sky, MT, USA, 5–12 March 2016. [Google Scholar] [CrossRef]
- Coburn, J.Q.; Freeman, I.; Salmon, J.L. A review of the capabilities of current low-cost virtual reality technology and its potential to enhance the design process. J. Comput. Inf. Sci. Eng. 2017, 17, 031013. [Google Scholar] [CrossRef]
- Bisso, E.; Signorelli, M.S.; Milazzo, M.; Maglia, M.; Polosa, R.; Aguglia, E.; Caponnetto, P. Immersive virtual reality applications in schizophrenia spectrum therapy: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6111. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Davide, F.; Ijsselsteijn, W. Being There: The experience of presence in mediated environments. Being There Concepts Eff. Meas. User Presence Synth. Environ. 2003, 5. [Google Scholar]
- Beidel, D.C.; Tuerk, P.W.; Spitalnick, J.; Bowers, C.A.; Morrison, K. Treating childhood social anxiety disorder with virtual environments and serious games: A randomized trial. Behav. Ther. 2021, 52, 1351–1363. [Google Scholar] [CrossRef] [PubMed]
- Ip, H.H.S.; Wong, S.W.L.; Chan, D.F.Y.; Byrne, J.; Li, C.; Yuan, V.S.N.; Lau, K.S.Y.; Wong, J.Y.W. Enhance emotional and social adaptation skills for children with autism spectrum disorder: A virtual reality enabled approach. Comput. Educ. 2018, 117, 1–15. [Google Scholar] [CrossRef]
- Amat, A.Z.; Zhao, H.; Swanson, A.; Weitlauf, A.S.; Warren, Z.; Sarkar, N. Design of an interactive virtual reality system, invirs, for joint attention practice in autistic children. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1866–1876. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.O.; Bailenson, J.N.; Obradović, J.; Aguiar, N.R. Virtual reality’s effect on children’s inhibitory control, social compliance, and sharing. J. Appl. Dev. Psychol. 2019, 64, 101052. [Google Scholar] [CrossRef]
- Battistich, V.; Schaps, E.; Watson, M.; Solomon, D. Prevention effects of the child development project. J. Adolesc. Res. 1996, 11, 12–35. [Google Scholar] [CrossRef]
- Malhotra, N.; Ayele, Z.E.; Zheng, D.; Ben Amor, Y. Improving social and emotional learning for schoolgirls: An impact study of curriculum-based socio-emotional education in rural Uganda. Int. J. Educ. Res. 2021, 108, 101778. [Google Scholar] [CrossRef]
- Taylor, R.D.; Oberle, E.; Durlak, J.A.; Weissberg, R.P. Promoting positive youth development through school-based social and emotional learning interventions: A meta-analysis of follow-up effects. Child Dev. 2017, 88, 1156–1171. [Google Scholar] [CrossRef] [PubMed]
- Blewitt, C.; O’Connor, A.; May, T.; Morris, H.; Mousa, A.; Bergmeier, H.; Jackson, K.; Barrett, H.; Skouteris, H. Strengthening the social and emotional skills of pre-schoolers with mental health and developmental challenges in inclusive early childhood education and care settings: A narrative review of educator-led interventions. Early Child Dev. Care 2021, 191, 2311–2332. [Google Scholar] [CrossRef]
- Parsons, S. Authenticity in virtual reality for assessment and intervention in autism: A conceptual review. Educ. Res. Rev. 2016, 19, 138–157. [Google Scholar] [CrossRef]
- Ke, F.; Im, T. Virtual-reality-based social interaction training for children with high-functioning autism. J. Edu. Res. 2013, 106, 441–461. [Google Scholar] [CrossRef]
- Montoya-Rodríguez, M.M.; de Souza Franco, V.; Tomás Llerena, C.; Molina Cobos, F.J.; Pizzarossa, S.; García, A.C.; Martínez-Valderrey, V. Virtual reality and augmented reality as strategies for teaching social skills to individuals with intellectual disability: A systematic review. J. Intellect. Disabil. 2022, 27, 1062–1084. [Google Scholar] [CrossRef] [PubMed]
- Farashi, S.; Bashirian, S.; Jenabi, E.; Razjouyan, K. Effectiveness of virtual reality and computerized training programs for enhancing emotion recognition in people with autism spectrum disorder: A systematic review and meta-analysis. Int. J. Dev. Disabil. 2022, 1–17. [Google Scholar] [CrossRef]
- Skjoldborg, N.M.; Bender, P.K.; Jensen de López, K.M. The efficacy of head-mounted-display virtual reality intervention to improve life skills of individuals with autism spectrum disorders: A systematic review. Neuropsychiatr. Dis. Treat. 2022, 18, 2295–2310. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, P.; Triscari, S.; Maglia, M.; Quattropani, M.C. The simulation game-virtual reality therapy for the treatment of social anxiety disorder: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 13209. [Google Scholar] [CrossRef]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of virtual reality for children and adolescents with autism spectrum disorder: An evidence-based systematic review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef]
- Adabla, S.; Nabors, L.; Hamblin, K. A scoping review of virtual reality interventions for youth with attention-deficit/hyperactivity disorder. Adv. Neurodev. Disord. 2021, 5, 304–315. [Google Scholar] [CrossRef]
- Merchant, Z.; Goetz, E.T.; Cifuentes, L.; Keeney-Kennicutt, W.; Davis, T.J. Effectiveness of virtual reality-based instruction on students’ learning outcomes in K-12 and higher education: A meta-analysis. Comput. Educ. 2014, 70, 29–40. [Google Scholar] [CrossRef]
- Hedges, L.V. Distribution theory for glass’s estimator of effect size and related estimators. J. Edu. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Zieher, A.K.; Cipriano, C.; Meyer, J.L.; Strambler, M.J. Educators’ implementation and use of social and emotional learning early in the COVID-19 pandemic. Sch. Psychol. 2021, 36, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Belter, M.; Liu, J.; Lukosch, H. Immersive virtual reality enabled interventions for autism spectrum disorder: A systematic review and meta-analysis. Electronics 2023, 12, 2497. [Google Scholar] [CrossRef]
- Lorenzo, G.; Lledó, A.; Pomares, J.; Roig, R. Design and application of an immersive virtual reality system to enhance emotional skills for children with autism spectrum disorders. Comput. Educ. 2016, 98, 192–205. [Google Scholar] [CrossRef]
- Sarver, N.W.; Beidel, D.C.; Spitalnick, J.S. The feasibility and acceptability of virtual environments in the treatment of childhood social anxiety disorder. J. Clin. Child Adolesc. Psychol. 2014, 43, 63–73. [Google Scholar] [CrossRef]
- Rosenfield, N.S.; Lamkin, K.; Re, J.; Day, K.; Boyd, L.; Linstead, E. A virtual reality system for practicing conversation skills for children with autism. Multimodal Technol. Interact. 2019, 3, 28. [Google Scholar] [CrossRef]
- Irish, J.E.N. Can I sit here? A review of the literature supporting the use of single-user virtual environments to help adolescents with autism learn appropriate social communication skills. Comput. Human Behav. 2013, 29, A17–A24. [Google Scholar] [CrossRef]
- Ip, H.H.S.; Wong, S.W.L.; Chan, D.F.Y.; Li, C.; Kon, L.L.; Ma, P.K.; Lau, K.S.Y.; Byrne, J. Enhance affective expression and social reciprocity for children with autism spectrum disorder: Using virtual reality headsets at schools. Interact. Learn. Environ. 2022, 1–24. [Google Scholar] [CrossRef]
- Lorenzo, G.; Lledó, A.; Arráez-Vera, G.; Lorenzo-Lledó, A. The application of immersive virtual reality for students with ASD: A review between 1990–2017. Educ. Inf. Technol. 2019, 24, 127–151. [Google Scholar] [CrossRef]
- Newbutt, N.; Sung, C.; Kuo, H.-J.; Leahy, M.J.; Lin, C.-C.; Tong, B. Brief report: A pilot study of the use of a virtual reality headset in autism populations. J. Autism Dev. Disord. 2016, 46, 3166–3176. [Google Scholar] [CrossRef] [PubMed]
- Soltani Kouhbanani, S.; Khosrorad, R.; Zarenezhad, S.; Arabi, S.M. Comparing the effect of risperidone, virtual reality and risperidone on social skills, and behavioral problems in children with autism: A follow-up randomized clinical trial. Arch. Iran. Med. 2021, 24, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Frolli, A.; Savarese, G.; Di Carmine, F.; Bosco, A.; Saviano, E.; Rega, A.; Carotenuto, M.; Ricci, M.C. Children on the autism spectrum and the use of virtual reality for supporting social skills. Children 2022, 9, 181. [Google Scholar] [CrossRef] [PubMed]
- Kuriakose, S.; Lahiri, U. Design of a physiology-sensitive VR-based social communication platform for children with autism. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, U.; Bekele, E.; Dohrmann, E.; Warren, Z.; Sarkar, N. Design of a virtual reality based adaptive response technology for children with autism. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 55–64. [Google Scholar] [CrossRef]
- He, J.; Zhang, H.; Zhao, H. Research on the auxiliary treatment system of childhood autism based on virtual reality. J. Decis. Syst. 2021, 1–18. [Google Scholar] [CrossRef]
- Wu, B.; Yu, X.; Gu, X. Effectiveness of immersive virtual reality using head-mounted displays on learning performance: A meta-analysis. Br. J. Educ. Technol. 2020, 51, 1991–2005. [Google Scholar] [CrossRef]
- Tsai, W.-T.; Lee, I.J.; Chen, C.-H. Inclusion of third-person perspective in CAVE-like immersive 3D virtual reality role-playing games for social reciprocity training of children with an autism spectrum disorder. Univers. Access Inf. Soc. 2020, 20, 375–389. [Google Scholar] [CrossRef]
- Johnson, M.T.; Troy, A.H.; Tate, K.M.; Allen, T.T.; Tate, A.M.; Chapman, S.B. Improving classroom communication: The effects of virtual social training on communication and assertion skills in middle school students. Front. Educ. 2021, 6, 678640. [Google Scholar] [CrossRef]
- Zhao, H.; Swanson, A.R.; Weitlauf, A.S.; Warren, Z.E.; Sarkar, N. Hand-in-Hand: A communication-enhancement collaborative virtual reality system for promoting social interaction in children with autism spectrum disorders. IEEE Trans. Hum. Mach. Syst. 2018, 48, 136–148. [Google Scholar] [CrossRef]
- DeRosier, M.E.; Thomas, J.M. Hall of Heroes: A digital game for social skills training with young adolescents. Int. J. Comput. Games Technol. 2019, 2019, 1–12. [Google Scholar] [CrossRef]
- Carreon, A.; Smith, S.J.; Frey, B.; Rowland, A.; Mosher, M. Comparing immersive VR and non-immersive VR on social skill acquisition for students in middle school with ASD. J. Res. Technol. Edu. 2023, 1–14. [Google Scholar] [CrossRef]
- Kolk, A.; Saard, M.; Roštšinskaja, A.; Sepp, K.; Kööp, C. Power of combined modern technology: Multitouch-multiuser tabletops and virtual reality platforms (PowerVR) in social communication skills training for children with neurological disorders: A pilot study. Appl. Neuropsychol. Child 2023, 12, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Babu, P.R.K.; Sinha, S.; Roshaan, A.S.; Lahiri, U. Multiuser digital platform to promote interaction skill in individuals with autism. IEEE Trans. Learn. Technol. 2022, 15, 798–811. [Google Scholar] [CrossRef]
- Lorusso, M.L.; Travellini, S.; Giorgetti, M.; Negrini, P.; Reni, G.; Biffi, E. Semi-immersive virtual reality as a tool to improve cognitive and social abilities in preschool children. Appl. Sci. 2020, 10, 2948. [Google Scholar] [CrossRef]
- Dechsling, A.; Orm, S.; Kalandadze, T.; Sütterlin, S.; Øien, R.A.; Shic, F.; Nordahl-Hansen, A. Virtual and augmented reality in social skills interventions for individuals with autism spectrum disorder: A scoping review. J. Autism Dev. Disord. 2022, 52, 4692–4707. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Sotos, P.; Fernández-Caballero, A.; Rodriguez-Jimenez, R. Virtual reality for psychosocial remediation in schizophrenia: A systematic review. Eur. J. Psychiatry 2020, 34, 1–10. [Google Scholar] [CrossRef]
- Cheng, Y.; Huang, C.-L.; Yang, C.-S. Using a 3D immersive virtual environment system to enhance social understanding and social skills for children with autism spectrum disorders. Focus Autism Other Dev. Disabl. 2015, 30, 222–236. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Rosenthal, R. The file drawer problem and tolerance for null results. Psychol. Bull. 1979, 86, 638–641. [Google Scholar] [CrossRef]
- Dalgarno, B.; Lee, M.J.W. What are the learning affordances of 3-D virtual environments? Br. J. Educ. Technol. 2010, 41, 10–32. [Google Scholar] [CrossRef]
- Liber, D.B.; Frea, W.D.; Symon, J.B. Using time-delay to improve social play skills with peers for children with autism. J. Autism Dev. Disord. 2008, 38, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Elsabbagh, M.; Divan, G.; Koh, Y.-J.; Kim, Y.S.; Kauchali, S.; Marcín, C.; Montiel-Nava, C.; Patel, V.; Paula, C.S.; Wang, C.; et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012, 5, 160–179. [Google Scholar] [CrossRef] [PubMed]
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef]
- Satu, P.; Minna, L.; Satu, S. Immersive VR assessment and intervention research of individuals with neurodevelopmental disorders is dominated by ASD and ADHD: A scoping review. Rev. J. Autism Dev. Disord. 2023. [Google Scholar] [CrossRef]
- Mosher, M.A.; Carreon, A.C.; Craig, S.L.; Ruhter, L.C. Immersive technology to teach social skills to students with autism spectrum disorder: A literature review. Rev. J. Autism Dev. Disord. 2022, 9, 334–350. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Published from January 2013 to May 2023 | Publication date of the article is not within this range |
| Written in English | Written in other languages |
| Participants are children or adolescents | Participants over 18 years of age |
| Empirical studies | Non-empirical studies and literature reviews |
| Participants use VR technology to learn | VR is not used during the intervention |
| Research focuses on one or more social emotional learning skills | Research does not focus on social emotional learning |
| Category | Code | Description |
|---|---|---|
| Metadata | Title | Full title |
| Authors | Author names | |
| Year | Publication year | |
| Source | Journal information | |
| Article type | Journal/conference | |
| Country/region | Experimental location | |
| Participant characteristics | Age | Age range of participants |
| Gender | Male only/female only/mostly male/mostly female/Co-Ed | |
| Grade level | Preschool/primary school/secondary school | |
| IQ | Below 80/more than 80 | |
| Disorder type | Autism spectrum disorders/neurological disorder/social anxiety disorder/ADHD/TD | |
| Research design | Research type | Experimental/quantitative/qualitative/mixed method/survey/design-based research |
| Sample size | Number of participants | |
| Number of interventions | Number of VR interventions | |
| Intervention duration | Total duration of the intervention | |
| Data collection | Content tests/surveys/interviews/physiological indexes/video recordings/score/observations/other | |
| Technological features | Technological type | Simulation/game/virtual world |
| Equipment | Computer/head-mounted display/glasses/projector | |
| Immersion level | Full immersion/semi-immersion | |
| Interaction level | None/low/medium/high | |
| Fidelity | None/low/medium/high | |
| Instructional design | VR function | Content delivery/practice/engagement |
| Pedagogy | Game-based learning/collaborative/experiential learning/direct instruction | |
| Learning objectives | Social interaction skills/social knowledge/positive social behavior/emotional distress/attitudes toward self and others | |
| Scenario | Room/school/bus/park/natural environment/game | |
| Task | Social task/cognitive task (low/high/metacognition)/psychomotor task | |
| Theoretical foundation | Record if mentioned |
| Model | No. of Studies | Hedge’s g | 95% Confidence Interval | Test of Null | Heterogeneity | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | Z | p | Q | df | p | I2 | |||
| Fixed | 31 | 0.387 | 0.317 | 0.457 | 10.786 | 0.000 | 120.053 | 30 | 0.000 | 75.011 |
| Random | 31 | 0.378 | 0.226 | 0.531 | 4.861 | 0.000 | ||||
| Moderator | k | g | 95% CI | QB | p Value |
|---|---|---|---|---|---|
| Number of interventions | 1.525 | 0.677 | |||
| 1 | 11 | 0.252 | [−0.050–0.553] | ||
| 2–10 | 6 | 0.354 | [0.249–0.460] *** | ||
| 11–30 | 9 | 0.346 | [−0.033–0.726] | ||
| >30 | 5 | 0.698 | [0.050–1.347] * | ||
| Disorder type | 28.117 *** | 0.000 | |||
| ASD | 19 | 0.469 | [0.254–0.684] *** | ||
| SAD | 1 | −0.854 | [−1.319–−0.388] *** | ||
| Social problem | 2 | 0.543 | [0.134–0.951] ** | ||
| Mixed | 3 | 0.410 | [0.162–0.658] ** | ||
| TD | 6 | 0.262 | [0.010–0.515] * | ||
| Technological type | 2.905 | 0.234 | |||
| Game | 7 | 0.061 | [−0.420–0.542] | ||
| Simulation | 20 | 0.370 | [0.218–0.523] *** | ||
| Virtual world | 4 | 0.822 | [0.056–1.588] * | ||
| Equipment | 2.682 | 0.443 | |||
| Computer | 17 | 0.275 | [0.074–0.476] ** | ||
| Glasses | 3 | 0.455 | [0.212–0.698] *** | ||
| HMD | 7 | 0.387 | [0.088–0.687] ** | ||
| Projector | 4 | 0.822 | [0.236–0.506] * | ||
| Interaction level | 1.597 | 0.660 | |||
| Low | 2 | 0.333 | [−0.101–0.767] | ||
| Medium | 3 | 0.337 | [0.216–0.459] *** | ||
| High | 22 | 0.312 | [0.110–0.515] ** | ||
| None | 4 | 0.822 | [0.239–0.440] * | ||
| Fidelity | 2.824 | 0.588 | |||
| Low | 3 | −0.167 | [−0.979–0.645] | ||
| Medium | 3 | 0.410 | [0.162–0.658] | ||
| High | 14 | 0.348 | [0.141–0.555] | ||
| None | 3 | 0.483 | [0.262–0.704] | ||
| Not mentioned | 8 | 0.498 | [0.024–0.973] | ||
| Theoretical basis | 2.508 | 0.113 | |||
| Yes | 4 | 0.545 | [0.372–0.719] *** | ||
| No | 27 | 0.346 | [0.169–0.522] *** | ||
| Task | 15.126 * | 0.010 | |||
| Social task | 12 | 0.622 | [0.370–0.875] *** | ||
| Cognitive task (low) | 10 | 0.190 | [−0.104–0.521] | ||
| Cognitive task (high) | 1 | −2.124 | [−3.759–−0.489] ** | ||
| Psychomotor task | 3 | 0.120 | [−0.885–1.126] | ||
| Mixed | 3 | 0.337 | [0.216–0.459] *** | ||
| Not mentioned | 2 | 0.495 | [0.205–0.785] ** | ||
| Function | 1.683 | 0.413 | |||
| Practice | 26 | 0.322 | [0.170–0.474] *** | ||
| Engagement | 1 | 0.438 | [−0.117–0.993] | ||
| Content deliver | 4 | 0.391 | [0.056–1.588] * | ||
| Pedagogy | 2.618 | 0.454 | |||
| Experiential learning | 19 | 0.360 | [0.204–0.515] *** | ||
| Game-based learning | 7 | 0.082 | [−0.427–0.591] | ||
| Collaborative learning | 1 | 0.438 | [−0.117–0.993] | ||
| Direct instruction | 4 | 0.822 | [0.056–1.588] * | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, F.; Zhang, Y.; Li, G.; Luo, H. Using Virtual Reality Interventions to Promote Social and Emotional Learning for Children and Adolescents: A Systematic Review and Meta-Analysis. Children 2024, 11, 41. https://doi.org/10.3390/children11010041
Zhang F, Zhang Y, Li G, Luo H. Using Virtual Reality Interventions to Promote Social and Emotional Learning for Children and Adolescents: A Systematic Review and Meta-Analysis. Children. 2024; 11(1):41. https://doi.org/10.3390/children11010041
Chicago/Turabian StyleZhang, Feng, Yan Zhang, Gege Li, and Heng Luo. 2024. "Using Virtual Reality Interventions to Promote Social and Emotional Learning for Children and Adolescents: A Systematic Review and Meta-Analysis" Children 11, no. 1: 41. https://doi.org/10.3390/children11010041
APA StyleZhang, F., Zhang, Y., Li, G., & Luo, H. (2024). Using Virtual Reality Interventions to Promote Social and Emotional Learning for Children and Adolescents: A Systematic Review and Meta-Analysis. Children, 11(1), 41. https://doi.org/10.3390/children11010041