

Teaching Parents via Online Asynchronous Training to Use Speech-Generating Devices with Their Autistic Children: A Pilot Study


Abstract
1. Online Modules to Teach Parents with Autistic Children to Implement an AAC Communication Strategy
1.1. Parent and Caregiver Communication Training for Autism
1.2. Utilizing POWR + SGD with Autistic Children
1.3. The Present Study
- (1a)
- Parent communication opportunities and parent responsiveness?
- (1b)
- Child communication when paired with an SGD?
- (1c)
- Parents’ implementation fidelity of the POWR strategy?
- (2a)
- Does this intervention impact family and child functioning?
- (2b)
- Do families find the intervention to be acceptable and feasible?
2. Method
2.1. Participants
2.2. Dyad A
2.3. Dyad B
2.4. Research Design
2.5. Setting and Materials
2.6. Procedures
2.6.1. Baseline Phase
2.6.2. Parent Training
2.6.3. Intervention Phase
2.6.4. Maintenance Phase
3. Results
3.1. Response Measurement and Interobserver Agreement
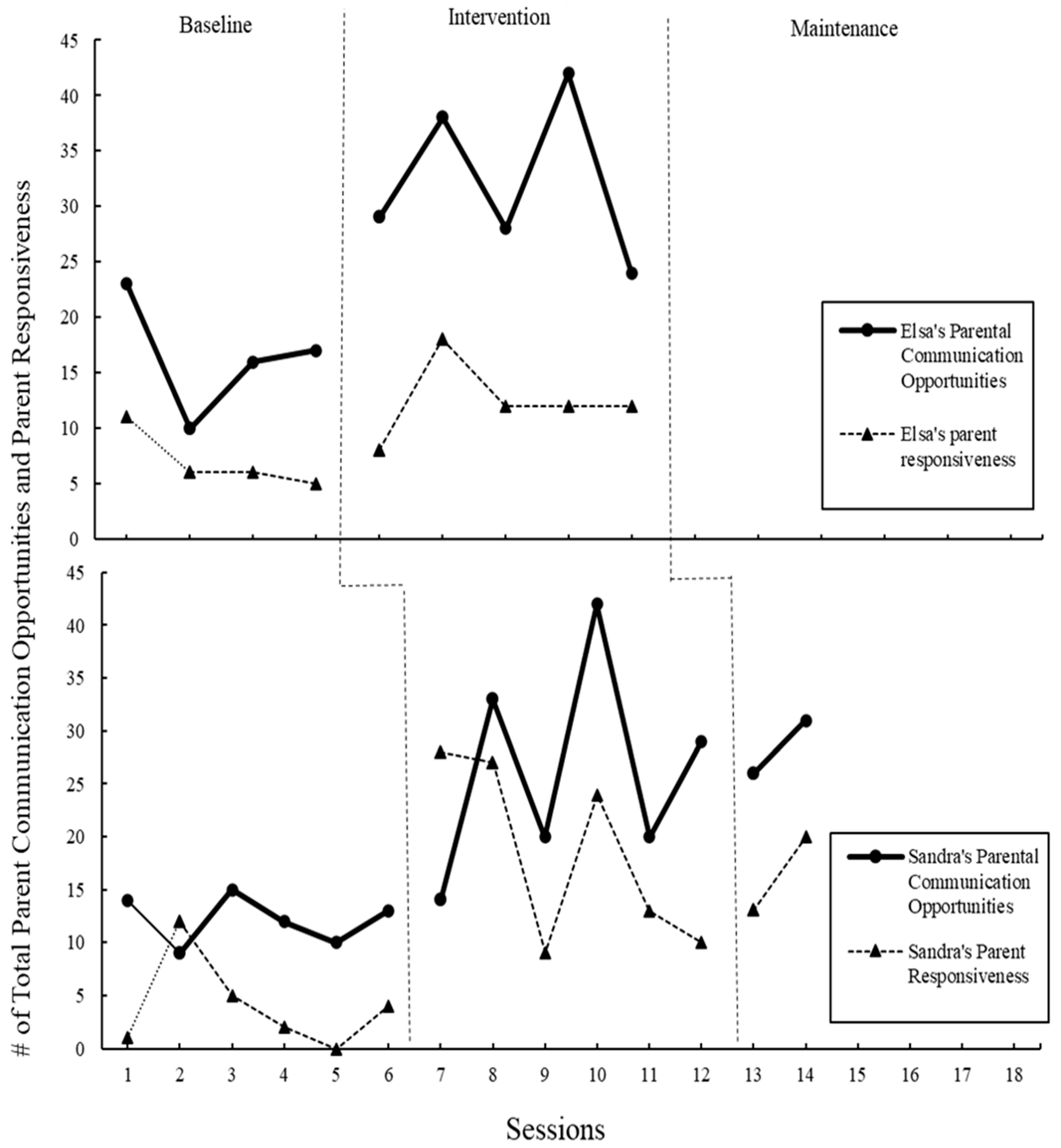
3.2. Parent’s Communication Opportunities
3.3. Parent Responsiveness
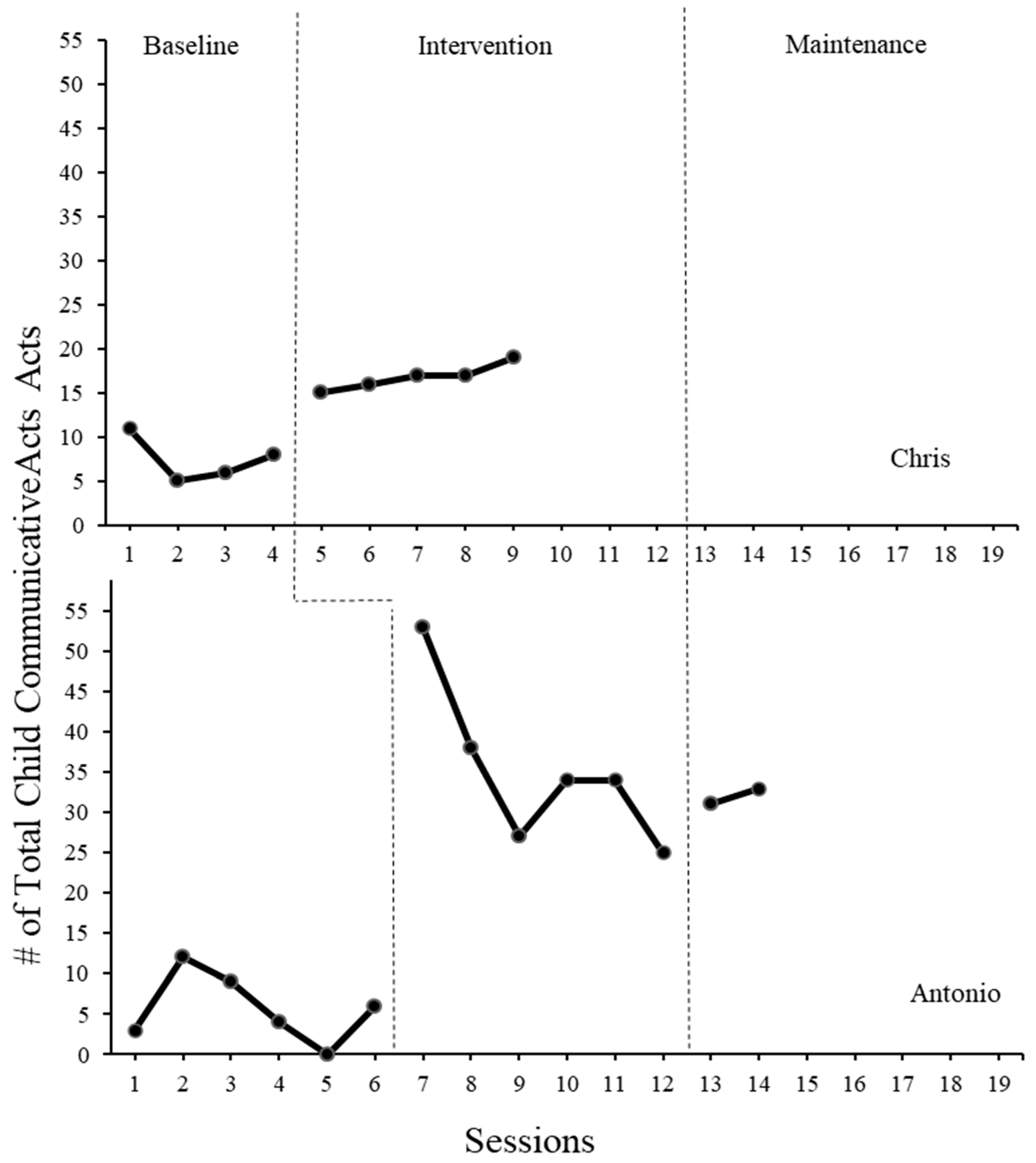
3.4. Child Communicative Acts
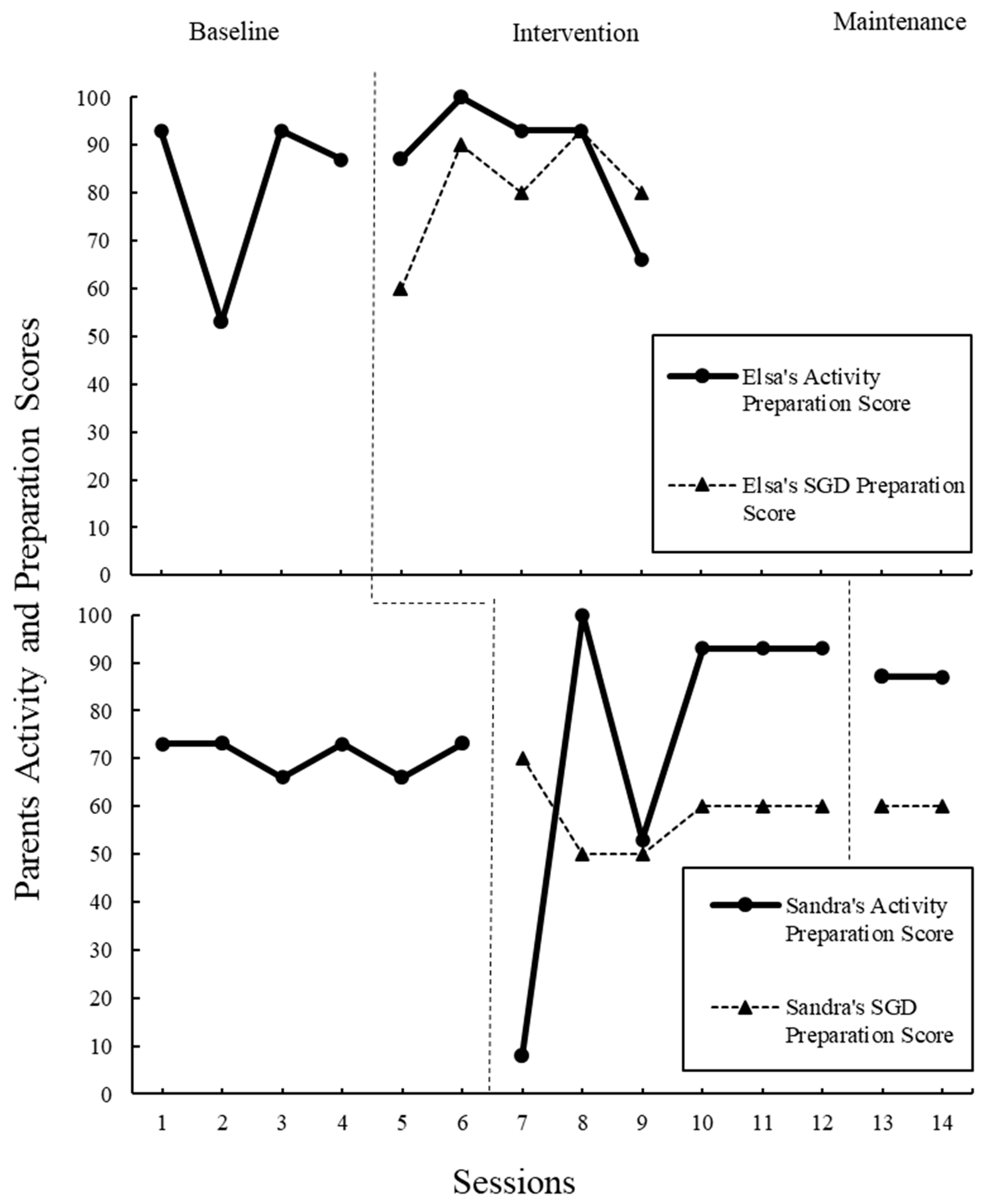
3.5. Parent Fidelity
3.6. Social Validity
3.6.1. Family Impact of Assistive Technology Scale for Augmentative and Alternative Communication
3.6.2. Interviews
4. Discussion
4.1. Central Research Question: Parent Communication and Responsiveness
4.2. Research Question Two: Child Communication Acts
4.3. Research Question Three: Parent Fidelity
4.4. Implications
4.4.1. Needs of Parent and Child: Are the Online Modules Alone Enough?
4.4.2. Child Communication Acts and Fit for Autistic Populations
4.4.3. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of Participant: | |||||
|---|---|---|---|---|---|
| Session number: | |||||
| Prepare the activity and AAC Rating | 5 | 4 | 3 | 2 | 1 |
| Is the activity motivating for the child? | Strongly Agree | Disagree | Neutral | Disagree | Strongly Disagree |
| Is the activity developmentally appropriate? | Strongly Agree | Disagree | Neutral | Disagree | Strongly Disagree |
| Does the activity allow opportunities for communication? | Strongly Agree | Disagree | Neutral | Disagree | Strongly Disagree |
| ACTIVITY SCORE | |||||
| Is the selected vocabulary aligned with the activity? | Strongly Agree | Disagree | Neutral | Disagree | Strongly Disagree |
| Functional? | Strongly Agree | Disagree | Neutral | Disagree | Strongly Disagree |
| SGD PREP SCORE |
References
- Tager-Flusberg, H.; Paul, R.; Lord, C.E. Language and communication in autism. In Handbook of Autism and Pervasive Developmental Disorder, 3rd ed.; Volkmar, F., Paul, R., Klin, A., Cohen, D.J., Eds.; Wiley: Hoboken, NJ, USA, 2005; Volume 1, pp. 335–364. [Google Scholar]
- Fuller, E.A.; Kaiser, A.P. The effects of early intervention on social communication outcomes for children with autism spectrum disorder: A meta-analysis. J. Autism Dev. Disord. 2020, 50, 1683–1700. [Google Scholar] [CrossRef] [PubMed]
- Douglas, S.N.; Nordquist, E.; Kammes, R.; Gerde, H. Online parent training to support children with complex communication needs. Infants Young Child. 2017, 30, 288–303. [Google Scholar] [CrossRef]
- Douglas, S.N.; Kammes, R.; Nordquist, E. Online communication training for parents of children with autism spectrum disorder. Commun. Disord. Q. 2018, 39, 415–425. [Google Scholar] [CrossRef]
- Douglas, S.N.; Gerde, H.K. A strategy to support the communication of students with autism spectrum disorder. Interv. Sch. Clin. 2019, 55, 32–38. [Google Scholar] [CrossRef]
- Marshall, J.; Goldbart, J. “Communication is everything I think” Parenting a child who needs augmentative and alternative communication (AAC). Int. J. Lang. Commun. Disord. 2008, 43, 77–98. [Google Scholar] [CrossRef]
- Hettiarachchi, S.; Kitnasamy, G.; Gopi, D. “Now I am a techie too”—Parental perceptions of using mobile technology for communication by children with complex communication needs in the Global South. Disabil. Rehabil. Assist. Technol. 2020, 15, 183–194. [Google Scholar] [CrossRef]
- Almirall, D.; DiStefano, C.; Chang, Y.-C.; Shire, S.; Kaiser, A.; Lu, X.; Nahum-Shani, I.; Landa, R.; Mathy, P.; Kasari, C. Longitudinal Effects of Adaptive Interventions with a Speech-Generating Device in Minimally Verbal Children with ASD. J. Clin. Child Adolesc. Psychol. 2016, 45, 442–456. [Google Scholar] [CrossRef]
- Meadan, H.; Snodgrass, M.R.; Meyer, L.E.; Fisher, K.W.; Chung, M.Y.; Halle, J.W. Internet-based parent-implemented intervention for young children with autism: A pilot study. J. Early Interv. 2016, 38, 3–23. [Google Scholar] [CrossRef]
- Yuan, W.; Kennedy, J.; Dunn, M.; Hsiao, Y.J.; Poppen, M. Impact of Speech Generating Device Interventions on Vocalizations of Individuals with Autism and Severe Communication Impairment: A Systematic Review of the Research. Educ. Train. Autism Dev. Disabil. 2024, 59, 233–256. [Google Scholar]
- Wainer, A.L.; Ingersoll, B.R. Increasing Access to an ASD Imitation Intervention via a Telehealth Parent Training Program. J. Autism Dev. Disord. 2015, 45, 3877–3890. [Google Scholar] [CrossRef]
- Anderson, K.L.; Balandin, S.; Stancliffe, R.J. Alternative service delivery models for families with a new speech generating device: Perspectives of parents and therapists. Int. J. Speech-Lang. Pathol. 2015, 17, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Hume, K.; Steinbrenner, J.R.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Szendrey, S.; McIntyre, N.S.; Yücesoy-Özkan, S.; Savage, M.N. Evidence-Based Practices for Children, Youth, and Young Adults with Autism: Third Generation Review. J. Autism. Dev. Disord. 2021, 51, 4013–4032, Erratum in: J. Autism. Dev. Disord. 2023, 53, 514. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ganz, J.B.; Earles-Vollrath, T.L.; Heath, A.K.; Parker, R.I.; Rispoli, M.J.; Duran, J.B. A meta-analysis of single case research studies on aided augmentative and alternative communication systems with individuals with autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 60–74. [Google Scholar] [CrossRef] [PubMed]
- Alston, E.; St James-Roberts, I. Home environments of 10-month-old infants selected by the WILSTAAR screen for pre-language difficulties. Int. J. Lang. Commun. Disord. 2005, 40, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Salmon, K.; O’Kearney, R.; Reese, E.; Fortune, C.A. The role of language skill in child psychopathology: Implications for intervention in the early years. Clin. Child Fam. Psychol. Rev. 2016, 19, 352–367. [Google Scholar] [CrossRef]
- Hammer, C.; Tomblin, B.; Zhang, X.; Weiss, A. Relationships between parenting behaviors and specific language impairment in children. Int. J. Lang. Commun. Disord. 2001, 36, 185–205. [Google Scholar] [CrossRef]
- Roberts, M.Y.; Kaiser, A.P. The effectiveness of parent-implemented language interventions: A meta-analysis. Am. J. Speech-Lang. Pathol. 2011, 20, 180–199. [Google Scholar] [CrossRef]
- Karaaslan, O.; Diken, I.; Mahoney, G. A randomized control study of responsive teaching with young Turkish children and their mothers. Top. Early Child. Spec. Educ. 2013, 33, 18–27. [Google Scholar] [CrossRef]
- Kasari, C.; Kaiser, A.; Goods, K.; Nietfeld, J.; Mathy, P.; Landa, R.; Murphy, S.; Almirall, D. Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 635–646. [Google Scholar] [CrossRef]
- Mahoney, G.; Perales, F. Using relationship-focused intervention to enhance the social-emotional functioning of young children with autism spectrum disorders. Top. Early Child. Spec. Educ. 2003, 23, 74–86. [Google Scholar] [CrossRef]
- Dunst, C.J.; Raab, M.; Trivette, C.M. Characteristics of naturalistic language intervention strategies. (Report). J. Speech-Lang. Pathol. Appl. Behav. Anal. 2012, 5, 8–16. [Google Scholar]
- Edmunds, S.R.; Kover, S.T.; Stone, W.L. The relation between parent verbal responsiveness and child communication in young children with or at risk for autism spectrum disorder: A systematic review and meta-analysis. Autism Res. 2019, 12, 715–731. [Google Scholar] [CrossRef] [PubMed]
- McDuffie, A.; Yoder, P. Types of parent verbal responsiveness that predict language in young children with autism spectrum disorder. J. Speech Lang. Hear. Res. 2010, 53, 1026–1039. [Google Scholar] [CrossRef] [PubMed]
- Yoder, P.; Watson, L.R.; Lambert, W. Value-added predictors of expressive and receptive language growth in initially nonverbal preschoolers with autism spectrum disorders. J. Autism. Dev. Disord. 2015, 45, 1254–1270. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Thistle, J.J.; Wilkinson, K.M. What are the attention demands of aided aac? Perspect. Augment. Altern. Commun. 2012, 21, 17–22. [Google Scholar] [CrossRef]
- CoughDrop. CoughDrop—Every Voice Should Be Heard. Available online: https://www.mycoughdrop.com/ (accessed on 1 January 2014).
- Romski, M.; Sevcik, R.A. The complexities of AAC intervention research: Emergingtrends to consider. Augment. Altern. Commun. 2018, 34, 258–264. [Google Scholar] [CrossRef]
- Ryan, S.E.; Renzoni, A.M. Family Impact of Assistive Technology Scale for Augmentative and Alternative Communication-Volume 2 (FIATS-AAC) Technical manual. Holl-Bloorview Kids Rehabil. Hosp. 2015, 10, 2015. [Google Scholar]
- Sigafoos, J.; Arthur-Kelly, M.; Butterfield, N. Inventory of potential communicative acts. In Enhancing Everyday Communication for Children with Disabilities; Sigafoos, J., Arthur-Kelly, M., Butterfield, N., Eds.; Brookes: Baltimore, MD, USA, 2006; Appendix A. [Google Scholar]
- MacWhinney, B. The CHILDES Project: Tools for Analyzing Talk: Volume I: Transcription format and programs, Volume II: The database. Comput. Linguist. 2000, 26, 657. [Google Scholar] [CrossRef]
- Barker, R.M.; Akaba, S.; Brady, N.C.; Thiemann-Bourque, K. Support for AAC use in preschool, and growth in language skills, for young children with developmental disabilities. Augment. Altern. Commun. 2013, 29, 334–346. [Google Scholar] [CrossRef]
- Schlosser, R.W.; Wendt, O. Effects of augmentative and alternative communication intervention on speech production in children with autism: A systematic review. Am. J. Speech-Lang. Pathol. 2008, 17, 212–230. [Google Scholar] [CrossRef]
- Fettig, A.; Schultz, T.R.; Sreckovic, M.A. Effects of coaching on the implementation of functional assessment–based parent intervention in reducing challenging behaviors. J. Posit. Behav. Interv. 2015, 17, 170–180. [Google Scholar] [CrossRef]
- Glenn, E.; Taiwo, A.; Arbuckle, S.; Riehl, H.; McIntyre, L.L. Self-directed web-based parent-mediated interventions for autistic children: A systematic review. Rev. J. Autism Dev. Disord. 2023, 10, 505–522. [Google Scholar] [CrossRef]
- Beukelman, D.R.; Mirenda, P. Augmentative and Alternative Communication: Supporting Children and Adults with Complex Communication Needs, 4th ed.; Paul H. Brookes Publishing Co.: Baltimore, MD, USA, 2013. [Google Scholar]
- Light, J.; McNaughton, D. Communicative competence for individuals who require augmentative and alternative communication: A new definition for a new era of communication? Augment. Altern. Commun. 2014, 30, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Sapiets, S.J.; Hastings, R.P.; Stanford, C.; Totsika, V. Families’ access to early intervention and supports for children with developmental disabilities. J. Early Interv. 2023, 45, 103–121. [Google Scholar] [CrossRef]
- Kasari, C.; Siller, M.; Huynh, L.N.; Shih, W.; Swanson, M.; Hellemann, G.S.; Sugar, C.A. Randomized controlled trial of parental responsiveness intervention for toddlers at high risk for autism. Infant Behav. Dev. 2014, 37, 711. [Google Scholar] [CrossRef]
- Watson, L.R. Following the child’s lead: Mothers’ interactions with children with autism. J. Autism Dev. Disord. 1998, 28, 51–59. [Google Scholar] [CrossRef]
- Kent-Walsh, J.; Murza, K.A.; Malani, M.D.; Binger, C. Effects of Communication Partner Instruction on the Communication of Individuals using AAC: A Meta-Analysis. Augment. Altern. Commun. 2015, 31, 271–284. [Google Scholar] [CrossRef] [PubMed]

| Session | Elsa and Chris | Sandra and Antonio |
|---|---|---|
| Baseline | ||
| 1 | Toys, light-up penguin, ball | Bus, letter popsicles, Lego blocks |
| 2 | reading books | Eggs with shapes inside, Legos |
| 3 | Toys, ball, light-up penguin, owl | Sticker books |
| 4 | Toys, light-up penguin, owl | Legos |
| 5 | — | Blank dominos |
| 6 | — | Zipper and buckles/sticker book |
| Intervention | ||
| 1 | Cars + light-up penguin | Truck + letter popsicles |
| 2 | Steering wheel toy, ball, and snacks | Number cards |
| 3 | Dump truck +penguin | Reading picture books and toy cars |
| 4 | Penguin + cars | Marker + paper, writing letters |
| 5 | Penguin, cars, reading | Marker + paper, writing numbers |
| 6 | — | Marker + paper, writing |
| Maintenance | ||
| 1 | — | Blocks + cars |
| 2 | — | Jenga blocks |
| Verbal | AAC-SGD | Sign Language | Point/Gesture | Object | |
|---|---|---|---|---|---|
| B1 Chris | 0 | 0 | 2 | 5 | 4 |
| B2 Chris | 1 | 0 | 0 | 1 | 3 |
| B3 Chris | 0 | 0 | 1 | 0 | 5 |
| B4 Chris | 0 | 0 | 3 | 0 | 5 |
| I1 Chris | 0 | 8 | 1 | 2 | 4 |
| I2 Chris | 0 | 7 | 1 | 2 | 6 |
| I3 Chris | 0 | 12 | 0 | 2 | 3 |
| I4 Chris | 0 | 7 | 1 | 2 | 7 |
| I5 Chris | 0 | 10 | 2 | 4 | 3 |
| B1 Antonio | 3 | 0 | 0 | 0 | 0 |
| B2 Antonio | 11 | 0 | 0 | 0 | 1 |
| B3 Antonio | 7 | 0 | 0 | 0 | 2 |
| B4 Antonio | 4 | 0 | 0 | 0 | 0 |
| B5 Antonio | 0 | 0 | 0 | 0 | 0 |
| B6 Antonio | 5 | 0 | 0 | 0 | 1 |
| I1 Antonio | 50 | 3 | 0 | 0 | 0 |
| I2 Antonio | 35 | 2 | 0 | 0 | 1 |
| I3 Antonio | 11 | 11 | 0 | 4 | 1 |
| I4 Antonio | 30 | 3 | 0 | 1 | 0 |
| I5 Antonio | 34 | 0 | 0 | 0 | 0 |
| I6 Antonio | 24 | 1 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fischbacher, L.; Dodds, R.L.; Tien, I.S. Teaching Parents via Online Asynchronous Training to Use Speech-Generating Devices with Their Autistic Children: A Pilot Study. Children 2024, 11, 1194. https://doi.org/10.3390/children11101194
Fischbacher L, Dodds RL, Tien IS. Teaching Parents via Online Asynchronous Training to Use Speech-Generating Devices with Their Autistic Children: A Pilot Study. Children. 2024; 11(10):1194. https://doi.org/10.3390/children11101194
Chicago/Turabian StyleFischbacher, Lauren, Robin L. Dodds, and Ingrid Shiyin Tien. 2024. "Teaching Parents via Online Asynchronous Training to Use Speech-Generating Devices with Their Autistic Children: A Pilot Study" Children 11, no. 10: 1194. https://doi.org/10.3390/children11101194
APA StyleFischbacher, L., Dodds, R. L., & Tien, I. S. (2024). Teaching Parents via Online Asynchronous Training to Use Speech-Generating Devices with Their Autistic Children: A Pilot Study. Children, 11(10), 1194. https://doi.org/10.3390/children11101194