

The Role of Skin-to-Skin Contact and Breastfeeding in the First Hour Post Delivery in Reducing Excessive Weight Loss



Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Setting and Relevant Context
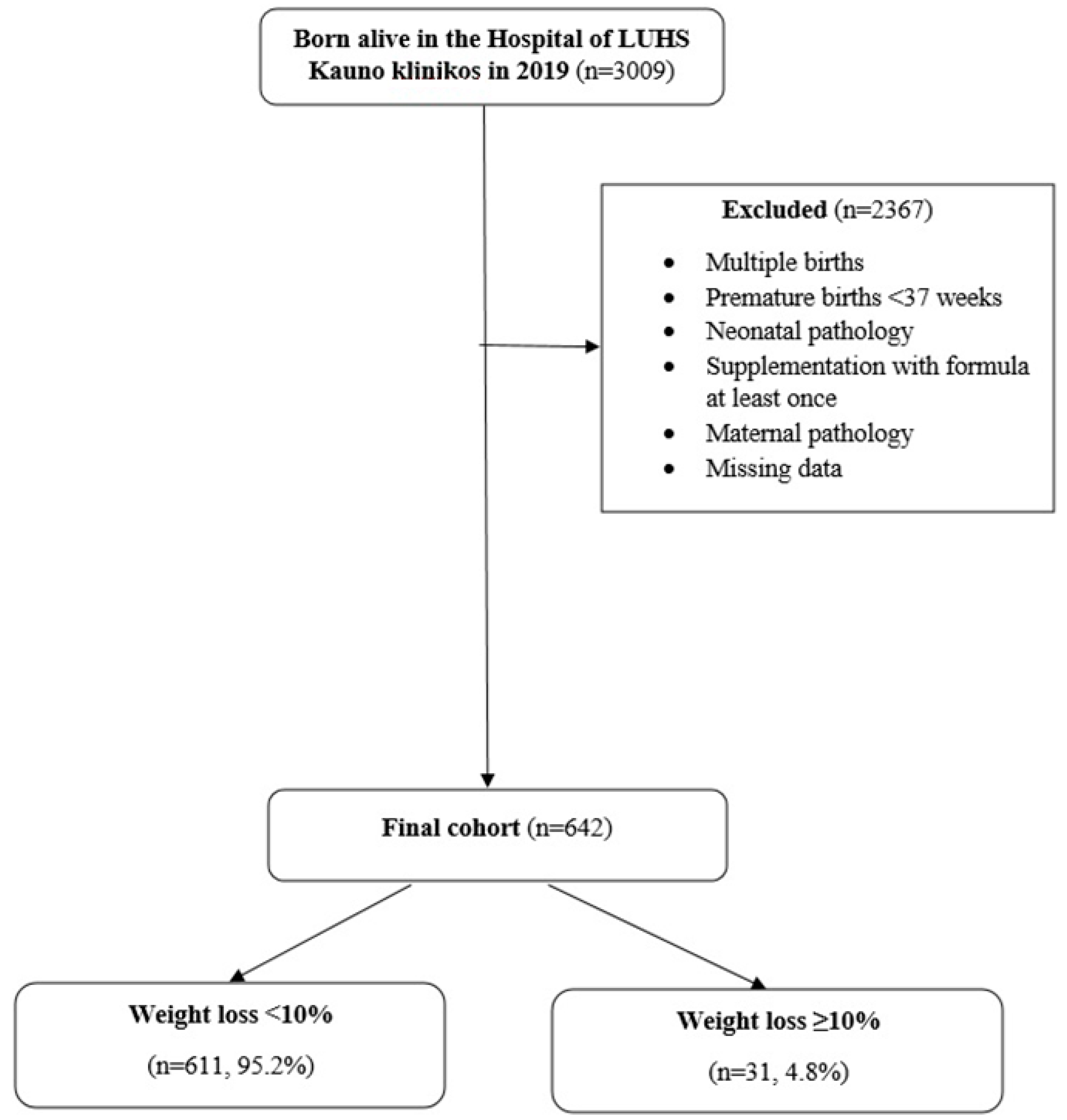
2.3. Sample
2.4. Measurement
2.5. Data Collection
2.6. Data Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNICEF. Baby-Friendly Hospital Initiative. Available online: https://www.unicef.org/documents/baby-friendly-hospital-initiative (accessed on 21 January 2024).
- World Health Organisation. Skin-to-Skin Contact Helps Newborns Breastfeed. Available online: https://www.who.int/westernpacific/news-room/feature-stories/item/skin-to-skin-contact-helps-newborns-breastfeed (accessed on 21 January 2024).
- Moore, E.R.; Anderson, G.C. Randomized Controlled Trial of Very Early Mother-Infant Skin-To-Skin Contact and Breastfeeding Status. J. Midwifery Women’s Health 2007, 52, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo-Hegyi, C.; Achilles, J.; Segrave-Daly, B.J.; Hafken, L. Fatal Hypernatremic Dehydration in a Term Exclusively Breastfed Newborn. Children 2022, 9, 1379. [Google Scholar] [CrossRef]
- Miyoshi, Y.; Suenaga, H.; Aoki, M.; Tanaka, S. Determinants of Excessive Weight Loss in Breastfed Full-Term Newborns at a Baby-Friendly Hospital: A Retrospective Cohort Study. Int. Breastfeed. J. 2020, 15, 19. [Google Scholar] [CrossRef]
- Geddes, D.T.; Gridneva, Z.; Perrella, S.L.; Mitoulas, L.R.; Kent, J.C.; Stinson, L.F.; Lai, C.T.; Sakalidis, V.; Twigger, A.-J.; Hartmann, P.E. 25 Years of Research in Human Lactation: From Discovery to Translation. Nutrients 2021, 13, 3071. [Google Scholar] [CrossRef] [PubMed]
- Kelly, N.M.; Keane, J.V.; Gallimore, R.B.; Bick, D.; Tribe, R.M. Neonatal Weight Loss and Gain Patterns in Caesarean Section Born Infants: Integrative Systematic Review. Matern. Child Nutr. 2020, 16, e12914. [Google Scholar] [CrossRef] [PubMed]
- Jayaraj, D.; Rao, S.; Balachander, B. Predisposing Factors for Excessive Loss of Weight in Exclusively Breastfed Term and Late Preterm Neonates—A Case Control Study. J. Matern.-Fetal Neonatal Med. 2020, 35, 3083–3088. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics; American College of Obstetricians and Gynecologists. Guidelines for Perinatal Care, 8th ed.; American Academy of Pediatrics: Washington, DC, USA; Elk Grove Village, IL, USA, 2017; pp. 347–408. [Google Scholar]
- World Health Organisation. Pregnancy, Childbirth, Postpartum and Newborn Care: A Guide for Essential Practice, 3rd ed.; United Nations Population Fund, UNICEF, Ed.; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- NICE. Faltering Growth: Recognition and Faltering Growth: Recognition and Management of Faltering Growth in Management of Faltering Growth in Children; NICE Guideline; NICE: Nice, France, 2017; pp. 5–6. Available online: https://www.nice.org.uk/guidance/ng75/resources/faltering-growth-recognition-and-management-of-faltering-growth-in-children-pdf-1837635907525 (accessed on 21 January 2024).
- Mezzacappa, M.A.; Ferreira, B.G. Excessive Weight Loss in Exclusively Breastfed Full-Term Newborns in a Baby-Friendly Hospital. Rev. Paul. Pediatr. 2016, 34, 281–286. [Google Scholar] [CrossRef]
- World Health Organization. Caesarean Section Rates Continue to Rise, Amid Growing Inequalities in Access. Available online: https://www.who.int/news/item/16-06-2021-caesarean-section-rates-continue-to-rise-amid-growing-inequalities-in-access (accessed on 21 January 2024).
- The Organization for Economic Cooperation and Development. Health Care Use—Caesarean Sections—OECD Data. The OECD. Available online: https://data.oecd.org/healthcare/caesarean-sections.htm (accessed on 21 January 2024).
- Mohebati, L.M.; Hilpert, P.; Bath, S.; Rayman, M.P.; Raats, M.M.; Martinez, H.; Caulfield, L.E. Perceived Insufficient Milk among Primiparous, Fully Breastfeeding Women: Is Infant Crying Important? Matern. Child Nutr. 2021, 17, e13133. [Google Scholar] [CrossRef]
- Sheedy, G.M.; Stulz, V.M.; Stevens, J. Exploring Outcomes for Women and Neonates Having Skin-To-Skin Contact during Caesarean Birth: A Quasi-Experimental Design and Qualitative Study. Women Birth 2022, 35, e530–e538. [Google Scholar] [CrossRef]
- Huang, X.; Chen, L.; Zhang, L. Effects of Paternal Skin-To-Skin Contact in Newborns and Fathers after Cesarean Delivery. J. Perinat. Neonatal Nurs. 2019, 33, 68–73. [Google Scholar] [CrossRef]
- World Health Organization. Impact of Continuous Kangaroo Mother Care Initiated Immediately after Birth (IKMC) on Survival of Newborns with Birth Weight between 1.0 to <1.8 Kg: Study Protocol for a Randomized Controlled Trial. Trials 2020, 21, 280. [Google Scholar] [CrossRef]
- Saxton, A.; Fahy, K.; Hastie, C. Pronurturance plus at Birth: A Risk Reduction Strategy for Preventing Postpartum Haemorrhage. Women Birth 2016, 29, 279–284. [Google Scholar] [CrossRef]
- Khan, J.; Vesel, L.; Bahl, R.; Martines, J.C. Timing of Breastfeeding Initiation and Exclusivity of Breastfeeding during the First Month of Life: Effects on Neonatal Mortality and Morbidity—A Systematic Review and Meta-Analysis. Matern. Child Health J. 2014, 19, 468–479. [Google Scholar] [CrossRef]
- Ekubay, M.; Berhe, A.; Yisma, E. Initiation of Breastfeeding within One Hour of Birth among Mothers with Infants Younger than or Equal to 6 Months of Age Attending Public Health Institutions in Addis Ababa, Ethiopia. Int. Breastfeed. J. 2018, 13, 4. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Gupta, A.; Bhatnagar, A.; Dutta, S. Effect of Very Early Skin to Skin Contact on Success at Breastfeeding and Preventing Early Hypothermia in Neonates. Indian J. Public Health 2014, 58, 22. [Google Scholar] [CrossRef] [PubMed]
- Edmond, K.M. Delayed Breastfeeding Initiation Increases Risk of Neonatal Mortality. Pediatrics 2006, 117, e380–e386. [Google Scholar] [CrossRef]
- Abdulghani, N.; Edvardsson, K.; Amir, L.H. Worldwide Prevalence of Mother-Infant Skin-To-Skin Contact after Vaginal Birth: A Systematic Review. PLoS ONE 2018, 13, e0205696. [Google Scholar] [CrossRef]
- Stevens, J.; Schmied, V.; Burns, E.; Dahlen, H. Immediate or Early Skin-To-Skin Contact after a Caesarean Section: A Review of the Literature. Matern. Child Nutr. 2014, 10, 456–473. [Google Scholar] [CrossRef] [PubMed]
- Ulfa, Y.; Maruyama, N.; Igarashi, Y.; Horiuchi, S. Early Initiation of Breastfeeding up to Six Months among Mothers after Cesarean Section or Vaginal Birth: A Scoping Review. Heliyon 2023, 9, e16235. [Google Scholar] [CrossRef]
- Guala, A.; Boscardini, L.; Visentin, R.; Angellotti, P.; Grugni, L.; Barbaglia, M.; Chapin, E.; Castelli, E.; Finale, E. Skin-To-Skin Contact in Cesarean Birth and Duration of Breastfeeding: A Cohort Study. Sci. World J. 2017, 2017, 1940756. [Google Scholar] [CrossRef]
- Widström, A.-M.; Lilja, G.; Aaltomaa-Michalias, P.; Dahllöf, A.; Lintula, M.; Nissen, E. Newborn Behaviour to Locate the Breast When Skin-To-Skin: A Possible Method for Enabling Early Self-Regulation. Acta Paediatr. 2010, 100, 79–85. [Google Scholar] [CrossRef]
- Kahalon, R.; Preis, H.; Benyamini, Y. Mother-Infant Contact after Birth Can Reduce Postpartum Post-Traumatic Stress Symptoms through a Reduction in Birth-Related Fear and Guilt. J. Psychosom. Res. 2022, 154, 110716. [Google Scholar] [CrossRef] [PubMed]
- Hardin, J.S.; Jones, N.A.; Mize, K.D.; Platt, M. Affectionate Touch in the Context of Breastfeeding and Maternal Depression Influences Infant Neurodevelopmental and Temperamental Substrates. Neuropsychobiology 2021, 80, 158–175. [Google Scholar] [CrossRef]
- Grisbrook, M.-A.; Dewey, D.; Cuthbert, C.; McDonald, S.; Ntanda, H.; Giesbrecht, G.F.; Letourneau, N. Associations among Caesarean Section Birth, Post-Traumatic Stress, and Postpartum Depression Symptoms. Int. J. Environ. Res. Public Health 2022, 19, 4900. [Google Scholar] [CrossRef]
- Mughal, S.; Azhar, Y.; Siddiqui, W. Postpartum Depression. National Library of Medicine. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519070/ (accessed on 21 January 2024).
- Cooijmans, K.H.M.; Beijers, R.; Rovers, A.C.; de Weerth, C. Effectiveness of Skin-To-Skin Contact versus Care-As-Usual in Mothers and Their Full-Term Infants: Study Protocol for a Parallel-Group Randomized Controlled Trial. BMC Pediatr. 2017, 17, 154. [Google Scholar] [CrossRef]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for Screening to Detect Major Depression among Pregnant and Postpartum Women: Systematic Review and Meta-Analysis of Individual Participant Data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.H.; Roshan, R.; Parikh, T.; Sathe, S.; Vaidya, U.; Pandit, A. LATCH Score at Discharge: A Predictor of Weight Gain and Exclusive Breastfeeding at 6 Weeks in Term Healthy Babies. J. Pediatr. Gastroenterol. Nutr. 2021, 72, e48. [Google Scholar] [CrossRef]
- Samayam, P. Study of Weight Patterns in Exclusively Breast Fed Neonates- Does the Route of Delivery Have an Impact? J. Clin. Diagn. Res. 2016, 10, sc01–sc03. [Google Scholar] [CrossRef]
- Flaherman, V.J.; Schaefer, E.W.; Kuzniewicz, M.W.; Li, S.X.; Walsh, E.M.; Paul, I.M. Early Weight Loss Nomograms for Exclusively Breastfed Newborns. Pediatrics 2014, 135, e16–e23. [Google Scholar] [CrossRef] [PubMed]
- Tagi, N.; Ergin, A.; Bilgen, H.S.; Ozek, E. The Use of the “Early Weight Loss Nomograms” as Compared to a Standard Weight Loss Percentage Protocol Will Decrease Postnatal Formula Supplementation. Breastfeed. Med. 2021, 17, 137–142. [Google Scholar] [CrossRef]
- Giudicelli, M.; Hassler, M.; Blanc, J.; Zakarian, C.; Tosello, B. Influence of Intrapartum Maternal Fluids on Weight Loss in Breastfed Newborns. J. Matern.-Fetal Neonatal Med. 2020, 35, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Lindower, J.B. Water Balance in the Fetus and Neonate. Semin. Fetal Neonatal Med. 2017, 22, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Eltonsy, S.; Blinn, A.; Sonier, B.; DeRoche, S.; Mulaja, A.; Hynes, W.; Barrieau, A.; Belanger, M. Intrapartum Intravenous Fluids for Caesarean Delivery and Newborn Weight Loss: A Retrospective Cohort Study. BMJ Paediatr. Open 2017, 1, e000070. [Google Scholar] [CrossRef] [PubMed]
- Lian, W.; Ding, J.; Xiong, T.; Liuding, J.; Nie, L. Determinants of Delayed Onset of Lactogenesis II among Women Who Delivered via Cesarean Section at a Tertiary Hospital in China: A Prospective Cohort Study. Int. Breastfeed. J. 2022, 17, 81. [Google Scholar] [CrossRef] [PubMed]
- Chantry, C.J.; Dewey, K.G.; Peerson, J.M.; Wagner, E.A.; Nommsen-Rivers, L.A. In-Hospital Formula Use Increases Early Breastfeeding Cessation among First-Time Mothers Intending to Exclusively Breastfeed. J. Pediatr. 2014, 164, 1339–1345.e5. [Google Scholar] [CrossRef] [PubMed]
- Bookhart, L.H.; Anstey, E.H.; Kramer, M.R.; Perrine, C.G.; Reis-Reilly, H.; Ramakrishnan, U.; Young, M.F. A Nation-Wide Study on the Common Reasons for Infant Formula Supplementation among Healthy, Term, Breastfed Infants in US Hospitals. Matern. Child Nutr. 2021, 18, e13294. [Google Scholar] [CrossRef]
- Agudelo, S.I.; Gamboa, O.A.; Acuña, E.; Aguirre, L.; Bastidas, S.; Guijarro, J.; Jaller, M.; Valderrama, M.; Padrón, M.L.; Gualdrón, N.; et al. Randomized Clinical Trial of the Effect of the Onset Time of Skin-To-Skin Contact at Birth, Immediate Compared to Early, on the Duration of Breastfeeding in Full Term Newborns. Int. Breastfeed. J. 2021, 16, 33. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, X.; Juan, J.; Yang, H.; Sobel, H.L.; Li, Z.; Narayan, A.; Huang, X.; Tian, X.; Zhang, L.; et al. Association of Duration of Skin-To-Skin Contact after Cesarean Section in China: A Superiority, Multi-Centric Randomized Controlled Trial. Am. J. Obstet. Gynecol. MFM 2023, 5, 101033. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Total Population, n = 642 | Delivery Mode | p | |
|---|---|---|---|---|
| VD, n = 529 | CS, n = 113 | |||
| Maternal age (years), Mdn [95% CI] | 31 [30.5–31.3] | 30.5 [30.4–31.2] | 31 [30.6–32.5] | 0.201 |
| Parity, Mdn [95% CI] | 2 [2.1–2.3] | 2 [2–2.3] | 2 [2.2–2.7] | 0.006 |
| Delivery, Mdn [95% CI] | 2 [1.8–1.9] | 2 [1.8–1.9] | 2 [1.7–2.1] | 0.395 |
| Gestational weeks, Mdn [95% CI] | 40 [39.4–39.6] | 40 [39.4–39.6] | 39 [39.1–39.5] | 0.019 |
| Variable | Total Population, n = 642 | Delivery Mode | p | |
|---|---|---|---|---|
| VD, n = 529 | CS, n = 113 | |||
| Male, % (n) | 50.8 (326) | 48.6 (257) | 61.1 (69) | 0.016 + |
| Birth weight (g), Mdn [95% CI] | 3540 [3509.6–3581.5] | 3545 [3494.9–3573] | 3540 [3508.6–3691.7] | 0.169 |
| Apgar score at 1 min., Mdn [95% CI] | 9 [9.2–9.3] * | 9 [9.2–9.4] ** | 9 [8.8–9.2] *** | <0.001 |
| Apgar score at 5 min., Mdn [95% CI] | 10 [9.8–10] * | 10 [9.7–10] ** | 10 [9.4–9.7] *** | <0.001 |
| SSC, % (n) ^ | 91.0 (548) | 95.5 (489) | 65.6 (59) | <0.001 |
| Breastfed in 1 h, % (n) ^ | 89.6 (516) | 95.4 (481) | 48.6 (35) | <0.001 |
| Weight Loss | Total Population, n = 642 | Delivery Mode | p | OR [95% CI] | |
|---|---|---|---|---|---|
| VD, n = 529 | CS, n = 113 | ||||
| ≥7% | |||||
| After 24 h, % (n) | 22.1 (142) | 18.0 (95) | 41.6 (47) | <0.001 | 3.3 [2.1–5.02] |
| After 48 h, % (n) | 43.8 (281) | 39.3 (208) | 64.6 (73) | <0.001 | 2.8 [1.8–4.3] |
| ≥10% | |||||
| After 24 h, % (n) | 1.4 (9) | 0.9 (5) | 3.5 (4) | 0.033 | 3.8 [1–14.6] |
| After 48 h, % (n) | 4.4 (28) | 2.8 (15) | 11.5 (13) | <0.001 | 4.5 [2.1–9.7] |
| Weight Reduction | VD+SSC+BF n = 475 | CS+SSC+BF n = 33 | p | OR [95% CI] |
|---|---|---|---|---|
| ≥7% | ||||
| After 24 h, % (n) | 18.3 (87) | 33.3 (11) | 0.035 | 2.23 [1.04–4.77] |
| After 48 h, % (n) | 39.6 (188) | 63.6 (21) | 0.007 | 2.67 [1.28–5.55] |
| ≥10% | ||||
| After 24 h, % (n) | 1.1 (5) | 0 (0) | NS | |
| After 48 h, % (n) | 2.7 (13) | 9.1 (3) | 0.043 | 3.55 [0.96–13.15] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurgelėnė, V.; Kuzmickienė, V.; Stonienė, D. The Role of Skin-to-Skin Contact and Breastfeeding in the First Hour Post Delivery in Reducing Excessive Weight Loss. Children 2024, 11, 232. https://doi.org/10.3390/children11020232
Jurgelėnė V, Kuzmickienė V, Stonienė D. The Role of Skin-to-Skin Contact and Breastfeeding in the First Hour Post Delivery in Reducing Excessive Weight Loss. Children. 2024; 11(2):232. https://doi.org/10.3390/children11020232
Chicago/Turabian StyleJurgelėnė, Valentina, Vilma Kuzmickienė, and Dalia Stonienė. 2024. "The Role of Skin-to-Skin Contact and Breastfeeding in the First Hour Post Delivery in Reducing Excessive Weight Loss" Children 11, no. 2: 232. https://doi.org/10.3390/children11020232
APA StyleJurgelėnė, V., Kuzmickienė, V., & Stonienė, D. (2024). The Role of Skin-to-Skin Contact and Breastfeeding in the First Hour Post Delivery in Reducing Excessive Weight Loss. Children, 11(2), 232. https://doi.org/10.3390/children11020232