
Association between Thyroid Function and Insulin Resistance Indices in Korean Adolescents: Findings from the 2014–2015 Korea National Health and Nutrition Examination Survey

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Data Source and Study Subjects
2.2. Measurements
2.3. Insulin Resistance Indices
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Participants
3.2. Association between Thyroid Function and IR Indices
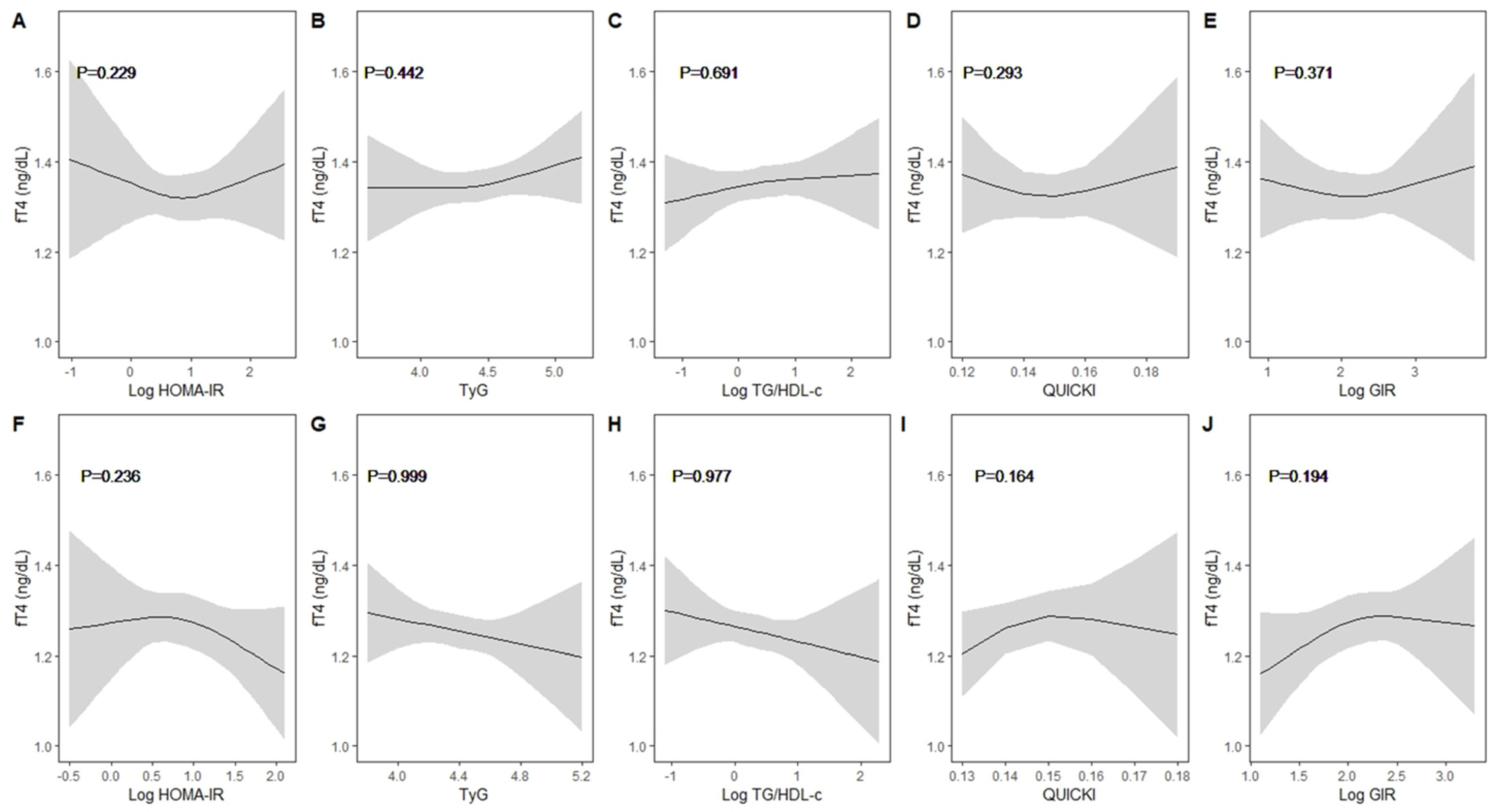
3.3. Nonlinearity Assessment between Thyroid Function Test and IR Indices by Sex
3.4. Association between Thyroid Function and IR Indices in the Presence or Absence of Obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lebovitz, H.E. Insulin resistance: Definition and consequences. Exp. Clin. Endocrinol. Diabetes 2001, 109 (Suppl. S2), S135–S148. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.M.; Kim, M.K.; Kwak, M.K.; Kim, D.; Hong, E.G. Association between thyroid hormones and insulin resistance indices based on the Korean National Health and Nutrition Examination Survey. Sci. Rep. 2021, 11, 21738. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Gautier, J.F.; Chon, S. Assessment of Insulin Secretion and Insulin Resistance in Human. Diabetes Metab. J. 2021, 45, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Saxena, A. Surrogate markers of insulin resistance: A review. World J. Diabetes 2010, 1, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Nur Zati Iwani, A.K.; Jalaludin, M.Y.; Yahya, A.; Mansor, F.; Md Zain, F.; Hong, J.Y.H.; Wan Mohd Zin, R.M.; Mokhtar, A.H. TG: HDL-C Ratio as Insulin Resistance Marker for Metabolic Syndrome in Children with Obesity. Front. Endocrinol. 2022, 13, 852290. [Google Scholar] [CrossRef]
- Choi, W.; Park, J.Y.; Hong, A.R.; Yoon, J.H.; Kim, H.K.; Kang, H.C. Association between triglyceride-glucose index and thyroid function in euthyroid adults: The Korea National Health and Nutritional Examination Survey 2015. PLoS ONE 2021, 16, e0254630. [Google Scholar] [CrossRef]
- Martinez, B.; Ortiz, R.M. Thyroid Hormone Regulation and Insulin Resistance: Insights from Animals Naturally Adapted to Fasting. Physiology 2017, 32, 141–151. [Google Scholar] [CrossRef]
- Santos, M.I.; Limbert, C.; Marques, F.C.; Rosario, F.; Lopes, L. Childhood obesity, thyroid function, and insulin resistance—Is there a link? A longitudinal study. J. Pediatr. Endocrinol. Metab. 2015, 28, 557–562. [Google Scholar] [CrossRef]
- Nader, N.S.; Bahn, R.S.; Johnson, M.D.; Weaver, A.L.; Singh, R.; Kumar, S. Relationships between thyroid function and lipid status or insulin resistance in a pediatric population. Thyroid 2010, 20, 1333–1339. [Google Scholar] [CrossRef]
- Ambrosi, B.; Masserini, B.; Iorio, L.; Delnevo, A.; Malavazos, A.E.; Morricone, L.; Sburlati, L.F.; Orsi, E. Relationship of thyroid function with body mass index and insulin-resistance in euthyroid obese subjects. J. Endocrinol. Investig. 2010, 33, 640–643. [Google Scholar] [CrossRef]
- Garduno-Garcia Jde, J.; Camarillo Romero, E.; Loe Ochoa, A.; Romero-Figueroa, S.; Huitron Bravo, G.; Torres Garcia, R.; Montenegro-Morales, P.; Mendieta-Zeron, H. Thyroid function is associated with insulin resistance markers in healthy adolescents with risk factors to develop diabetes. Diabetol. Metab. Syndr. 2015, 7, 16. [Google Scholar] [CrossRef]
- Lambadiari, V.; Mitrou, P.; Maratou, E.; Raptis, A.E.; Tountas, N.; Raptis, S.A.; Dimitriadis, G. Thyroid hormones are positively associated with insulin resistance early in the development of type 2 diabetes. Endocrine 2011, 39, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Hu, Y.; Zhao, H.; Zhou, G.; Wang, G.; Ma, C.; Xu, Y. Exploring the association between triglyceride-glucose index and thyroid function. Eur. J. Med. Res. 2023, 28, 508. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Chung, J.H. Update on Thyroid Hormone Levels and Thyroid Dysfunction in the Korean Population Based on Data from the Korea National Health and Nutrition Examination Survey VI (2013 to 2015). Endocrinol. Metab. 2020, 35, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Yun, S.; Hwang, S.S.; Shim, J.O.; Chae, H.W.; Lee, Y.J.; Lee, J.H.; Kim, S.C.; Lim, D.; Yang, S.W.; et al. The 2017 Korean National Growth Charts for children and adolescents: Development, improvement, and prospects. Korean J. Pediatr. 2018, 61, 135–149. [Google Scholar] [CrossRef]
- Dikaiakou, E.; Vlachopapadopoulou, E.A.; Paschou, S.A.; Athanasouli, F.; Panagiotopoulos, I.; Kafetzi, M.; Fotinou, A.; Michalacos, S. Tauriglycerides-glucose (TyG) index is a sensitive marker of insulin resistance in Greek children and adolescents. Endocrine 2020, 70, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J. An Overview of Current Physical Activity Recommendations in Primary Care. Korean J. Fam. Med. 2019, 40, 135–142. [Google Scholar] [CrossRef]
- Chae, J.; Seo, M.Y.; Kim, S.H.; Park, M.J. Trends and Risk Factors of Metabolic Syndrome among Korean Adolescents, 2007 to 2018. Diabetes Metab. J. 2021, 45, 880–889. [Google Scholar] [CrossRef]
- da Costa, V.M.; Moreira, D.G.; Rosenthal, D. Thyroid function and aging: Gender-related differences. J. Endocrinol. 2001, 171, 193–198. [Google Scholar] [CrossRef]
- Mitsumatsu, T.; Yoshimura Noh, J.; Iwaku, K.; Yoshihara, A.; Watanabe, N.; Aida, A.; Yoshimura, R.; Mikura, K.; Kinoshita, A.; Suzuki, A.; et al. Establishment of reference intervals for fT3, fT4, and TSH levels in Japanese children and adolescents. Endocr. J. 2023, 70, 815–823. [Google Scholar] [CrossRef]
- Campbell, P.J.; Brown, S.J.; Kendrew, P.; Lewer, M.; Lim, E.M.; Joseph, J.; Cross, S.M.; Wright, M.J.; Martin, N.G.; Wilson, S.G.; et al. Changes in Thyroid Function Across Adolescence: A Longitudinal Study. J. Clin. Endocrinol. Metab. 2020, 105, e1162–e1170. [Google Scholar] [CrossRef] [PubMed]
- Kapelari, K.; Kirchlechner, C.; Högler, W.; Schweitzer, K.; Virgolini, I.; Moncayo, R. Pediatric reference intervals for thyroid hormone levels from birth to adulthood: A retrospective study. BMC Endocr. Disord. 2008, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Soldin, S.J.; Cheng, L.L.; Lam, L.Y.; Werner, A.; Le, A.D.; Soldin, O.P. Comparison of FT4 with log TSH on the Abbott Architect ci8200: Pediatric reference intervals for free thyroxine and thyroid-stimulating hormone. Clin. Chim. Acta 2010, 411, 250–252. [Google Scholar] [CrossRef] [PubMed]
- Gierach, M.; Gierach, J.; Junik, R. Insulin resistance and thyroid disorders. Endokrynol. Pol. 2014, 65, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Alevizaki, M.; Saltiki, K.; Voidonikola, P.; Mantzou, E.; Papamichael, C.; Stamatelopoulos, K. Free thyroxine is an independent predictor of subcutaneous fat in euthyroid individuals. Eur. J. Endocrinol. 2009, 161, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Abiri, B.; Ahmadi, A.R.; Mahdavi, M.; Amouzegar, A.; Valizadeh, M. Association between thyroid function and obesity phenotypes in healthy euthyroid individuals: An investigation based on Tehran Thyroid Study. Eur. J. Med. Res. 2023, 28, 179. [Google Scholar] [CrossRef] [PubMed]
- Burman, K.D.; Latham, K.R.; Djuh, Y.Y.; Smallridge, R.C.; Tseng, Y.C.; Lukes, Y.G.; Maunder, R.; Wartofsky, L. Solubilized nuclear thyroid hormone receptors in circulating human mononuclear cells. J. Clin. Endocrinol. Metab. 1980, 51, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Cho, W.K.; Nam, H.K.; Kim, J.H.; Rhie, Y.J.; Chung, S.; Lee, K.H.; Suh, B.K. Thyroid Function in Korean Adolescents with Obesity: Results from the Korea National Health and Nutrition Examination Survey VI (2013–2015). Int. J. Endocrinol. 2018, 2018, 6874395. [Google Scholar] [CrossRef]
- An, Y.M.; Moon, S.J.; Kim, S.K.; Suh, Y.J.; Lee, J.E. Thyroid function in obese Korean children and adolescents: Korea National Health and Nutrition Examination Survey 2013–2015. Ann. Pediatr. Endocrinol. Metab. 2018, 23, 141–147. [Google Scholar] [CrossRef]
- Baik, S.J.; Park, B.H.; Lee, H.A.; Kim, H.S.; Hong, Y.S.; Park, H. Negative Association between Obesity Index and Thyroid Hormones in Euthyroid Children. Korean J. Obes. 2015, 24, 212–218. [Google Scholar] [CrossRef]
- Jin, H.Y. Prevalence of subclinical hypothyroidism in obese children or adolescents and association between thyroid hormone and the components of metabolic syndrome. J. Paediatr. Child. Health 2018, 54, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.A.; Kim, E.J. Association between thyroid hormone and components of metabolic syndrome in euthyroid Korean adults: A population-based study. Medicine 2021, 100, e28409. [Google Scholar] [CrossRef]
- Locateli, J.C.; Lopes, W.A.; Simões, C.F.; de Oliveira, G.H.; Oltramari, K.; Bim, R.H.; de Souza Mendes, V.H.; Remor, J.M.; Lopera, C.A.; Nardo Junior, N. Triglyceride/glucose index is a reliable alternative marker for insulin resistance in South American overweight and obese children and adolescents. J. Pediatr. Endocrinol. Metab. 2019, 32, 1163–1170. [Google Scholar] [CrossRef]
- Kang, B.; Yang, Y.; Lee, E.Y.; Yang, H.K.; Kim, H.S.; Lim, S.Y.; Lee, J.H.; Lee, S.S.; Suh, B.K.; Yoon, K.H. Triglycerides/glucose index is a useful surrogate marker of insulin resistance among adolescents. Int. J. Obes. 2017, 41, 789–792. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 465) | Boys (n = 255, 54.89%) | Girls (n = 210, 45.11%) | p | |
|---|---|---|---|---|
| Age (yrs) | 15.08 (14.8–815.28) | 15.18 (14.93–15.44) | 14.95 (14.64–15.26) | 0.253 |
| Household income | ||||
| Q1 (low) | 51 (11.50%) | 22 (9.01%) | 29 (14.57%) | 0.367 |
| Q2 | 122 (25.81%) | 67 (26.17%) | 55 (25.36%) | |
| Q3 | 166 (36.74%) | 95 (38.68%) | 71 (34.35%) | |
| Q4 (high) | 122 (25.95%) | 70 (26.13%) | 52 (25.71%) | |
| Aerobic exercise | 314 (70.08%) | 187 (77.36%) | 127 (61.50%) | 0.001 |
| Muscle exercise | 121 (25.28%) | 89 (34.97%) | 32 (13.64%) | <0.001 |
| Parental history of DM | 28 (6.38%) | 19 (8.26%) | 9 (4.11%) | 0.086 |
| TSH (uIU/mL) | 2.70 (2.57–2.84) | 2.86 (2.68–3.03) | 2.52 (2.32–2.72) | 0.013 |
| fT4 (ng/dL) | 1.29 (1.28–1.31) | 1.33 (1.31–1.35) | 1.24 (1.22–1.26) | <0.001 |
| Waist circumference (cm) | 73.33 (72.29–74.36) | 75.77 (74.39–77.15) | 70.36 (68.96–71.75) | <0.001 |
| Waist circumference (≥90th) | 59 (13.97%) | 31 (12.88%) | 28 (15.30%) | 0.540 |
| BMI (kg/m2) | 21.93 (21.52–22.34) | 22.32 (21.78–22.87) | 21.45 (20.88–22.03) | 0.028 |
| Normal weight | 354 (75.20%) | 192 (74.60%) | 162 (75.93%) | 0.954 |
| Overweight (85–94th) | 51 (10.30%) | 29 (10.46%) | 22 (10.11%) | |
| Obesity (≥95th) | 60 (14.49%) | 34 (14.93%) | 26 (13.96%) | |
| FBG (mg/dL) | 91.59 (90.91–92.28) | 92.9 (92–93.81) | 90 (88.98–91.03) | <0.001 |
| Insulin (uIU/mL) | 10.98 (10.21–11.81) | 10.80 (9.79–11.91) | 11.20 (10.02–12.52) | 0.629 |
| Total cholesterol (mg/dL) | 158.63 (155.91–161.35) | 154.46 (150.59–158.33) | 163.71 (159.52–167.89) | 0.003 |
| TG (mg/dL) | 73.46 (69.66–77.47) | 74.70 (68.89–80.99) | 71.98 (67.59–76.66) | 0.475 |
| HDL-C (mg/dL) | 51.50 (50.45–52.54) | 49.78 (48.39–51.18) | 53.58 (52.12–55.05) | <0.001 |
| Insulin resistance indices | ||||
| HOMA-IR | 2.48 (2.29–2.67) | 2.47 (2.23–2.73) | 2.49 (2.21–2.79) | 0.923 |
| QUICKI | 0.15 (0.14–0.15) | 0.15 (0.14–0.15) | 0.15 (0.14–0.15) | 0.838 |
| GIR | 8.31 (7.74–8.93) | 8.57 (7.79–9.42) | 8.03 (7.20–8.95) | 0.373 |
| TyG | 4.41 (4.38–4.43) | 4.42 (4.38–4.46) | 4.39 (4.35–4.42) | 0.189 |
| TG/HDL-C ratio | 1.45 (1.36–1.55) | 1.53 (1.39–1.68) | 1.37 (1.27–1.47) | 0.064 |
| Independent Variables | Outcomes | Unadjusted Model | Adjusted Model a | |||||
|---|---|---|---|---|---|---|---|---|
| β | 95% CI | p Value | β | 95% CI | p | |||
| Boys | log HOMA-IR | TSH | −0.21 | (−0.64, 0.22) | 0.337 | −0.17 | (−0.65, 0.31) | 0.488 |
| log HOMA-IR | fT4 | −0.03 | (−0.07, 0.00) | 0.053 | 0.01 | (−0.04, 0.05) | 0.798 | |
| TyG | TSH | 0.41 | (−0.18, 0.99) | 0.172 | 0.53 | (−0.05, 1.12) | 0.075 | |
| TyG | fT4 | 0.04 | (−0.03, 0.11) | 0.254 | 0.05 | (−0.02, 0.11) | 0.173 | |
| log TG/HDL-C | TSH | 0.09 | (−0.17, 0.36) | 0.482 | 0.14 | (−0.12, 0.41) | 0.288 | |
| log TG/HDL-C | fT4 | 0.02 | (−0.02, 0.05) | 0.321 | 0.02 | (−0.01, 0.05) | 0.237 | |
| QUICKI | TSH | 10.08 | (−10.83, 31.00) | 0.343 | 7.88 | (−15.72, 31.48) | 0.511 | |
| QUICKI | fT4 | 1.66 | (0.02, 3.30) | 0.047 | −0.12 | (−2.18, 1.93) | 0.908 | |
| log GIR | TSH | 0.27 | (−0.19, 0.73) | 0.244 | 0.26 | (−0.24, 0.75) | 0.311 | |
| log GIR | fT4 | 0.04 | (0.00, 0.08) | 0.049 | 0.00 | (−0.05, 0.05) | 0.928 | |
| Girls | log HOMA-IR | TSH | −0.25 | (−0.73, 0.23) | 0.300 | −0.30 | (−0.81, 0.20) | 0.232 |
| log HOMA-IR | fT4 | −0.04 | (−0.10, 0.01) | 0.141 | −0.05 | (−0.11, 0.00) | 0.045 | |
| TyG | TSH | 0.50 | (−0.28, 1.28) | 0.210 | 0.49 | (−0.36, 1.34) | 0.261 | |
| TyG | fT4 | −0.05 | (−0.15, 0.05) | 0.327 | −0.07 | (−0.17, 0.03) | 0.173 | |
| log TG/HDL-C | TSH | 0.17 | (−0.16, 0.51) | 0.310 | 0.17 | (−0.20, 0.54) | 0.362 | |
| log TG/HDL-C | fT4 | −0.02 | (−0.07, 0.02) | 0.276 | −0.03 | (−0.07, 0.01) | 0.103 | |
| QUICKI | TSH | 12.42 | (−11.35, 36.19) | 0.304 | 15.86 | (−9.31, 41.04) | 0.215 | |
| QUICKI | fT4 | 1.78 | (−0.93, 4.48) | 0.197 | 2.30 | (−0.26, 4.87) | 0.078 | |
| log GIR | TSH | 0.20 | (−0.28, 0.68) | 0.416 | 0.24 | (−0.27, 0.75) | 0.347 | |
| log GIR | fT4 | 0.05 | (−0.01, 0.11) | 0.082 | 0.06 | (0.01, 0.12) | 0.022 | |
| Normal Weight | Overweight & Obesity | |||||||
|---|---|---|---|---|---|---|---|---|
| Independent Variables | Outcomes | β | 95% CI | p | β | 95% CI | p | |
| Boys | log HOMA-IR | TSH | −0.17 | (−0.69, 0.36) | 0.534 | −0.15 | (−1.16, 0.86) | 0.770 |
| log HOMA-IR | fT4 | −0.01 | (−0.06, 0.04) | 0.773 | 0.08 | (0.00, 0.15) | 0.037 | |
| TyG | TSH | 0.24 | (−0.52, 1.00) | 0.537 | 1.01 | (0.07, 1.95) | 0.035 | |
| TyG | fT4 | 0.05 | (−0.03, 0.13) | 0.204 | 0.03 | (−0.08, 0.13) | 0.617 | |
| log TG/HDL-C | TSH | −0.04 | (−0.36, 0.28) | 0.804 | 0.42 | (0.00, 0.84) | 0.051 | |
| log TG/HDL-C | fT4 | 0.02 | (−0.02, 0.06) | 0.287 | 0.01 | (−0.04, 0.05) | 0.753 | |
| QUICKI | TSH | 7.12 | (−18.66, 32.89) | 0.586 | 7.18 | (−49.19, 63.56) | 0.801 | |
| QUICKI | fT4 | 0.40 | (−1.90, 2.70) | 0.732 | −4.14 | (−7.97, −0.31) | 0.034 | |
| log GIR | TSH | 0.28 | (−0.22, 0.78) | 0.267 | 0.22 | (−0.93, 1.38) | 0.704 | |
| log GIR | fT4 | 0.01 | (−0.05, 0.06) | 0.812 | −0.07 | (−0.16, 0.01) | 0.092 | |
| Girls | log HOMA-IR | TSH | −0.29 | (−0.99, 0.40) | 0.408 | −0.15 | (−0.66, 0.36) | 0.573 |
| log HOMA-IR | fT4 | −0.01 | (−0.08, 0.06) | 0.736 | −0.12 | (−0.19, −0.05) | 0.002 | |
| TyG | TSH | 0.13 | (−0.96, 1.22) | 0.815 | 1.38 | (0.32, 2.44) | 0.011 | |
| TyG | fT4 | −0.05 | (−0.18, 0.07) | 0.408 | −0.12 | (−0.25, 0.01) | 0.079 | |
| log TG/HDL-C | TSH | 0.03 | (−0.45, 0.52) | 0.894 | 0.44 | (−0.05, 0.93) | 0.081 | |
| log TG/HDL-C | fT4 | −0.03 | (−0.08, 0.02) | 0.305 | −0.06 | (−0.11, 0.00) | 0.046 | |
| QUICKI | TSH | 15.12 | (−18.08, 48.32) | 0.369 | 7.68 | (−17.00, 32.36) | 0.540 | |
| QUICKI | fT4 | 0.44 | (−2.85, 3.74) | 0.791 | 6.60 | (2.46, 10.73) | 0.002 | |
| log GIR | TSH | 0.14 | (−0.63, 0.91) | 0.719 | 0.39 | (−0.07, 0.84) | 0.095 | |
| log GIR | fT4 | 0.03 | (−0.05, 0.11) | 0.498 | 0.14 | (0.06, 0.22) | 0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mun, E.; Lee, H.A.; Choi, J.E.; Lee, R.; Kim, K.H.; Park, H.; Kim, H.S. Association between Thyroid Function and Insulin Resistance Indices in Korean Adolescents: Findings from the 2014–2015 Korea National Health and Nutrition Examination Survey. Children 2024, 11, 370. https://doi.org/10.3390/children11030370
Mun E, Lee HA, Choi JE, Lee R, Kim KH, Park H, Kim HS. Association between Thyroid Function and Insulin Resistance Indices in Korean Adolescents: Findings from the 2014–2015 Korea National Health and Nutrition Examination Survey. Children. 2024; 11(3):370. https://doi.org/10.3390/children11030370
Chicago/Turabian StyleMun, Eunji, Hye Ah Lee, Jung Eun Choi, Rosie Lee, Kyung Hee Kim, Hyesook Park, and Hae Soon Kim. 2024. "Association between Thyroid Function and Insulin Resistance Indices in Korean Adolescents: Findings from the 2014–2015 Korea National Health and Nutrition Examination Survey" Children 11, no. 3: 370. https://doi.org/10.3390/children11030370
APA StyleMun, E., Lee, H. A., Choi, J. E., Lee, R., Kim, K. H., Park, H., & Kim, H. S. (2024). Association between Thyroid Function and Insulin Resistance Indices in Korean Adolescents: Findings from the 2014–2015 Korea National Health and Nutrition Examination Survey. Children, 11(3), 370. https://doi.org/10.3390/children11030370