
Comparison of Percutaneous Internal Ring Suturing (PIRS) versus Open Ligation of the Patent Processus Vaginalis for the Treatment of Communicating Pediatric Hydrocele



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Ethical Aspects
2.3. Outcomes of the Study
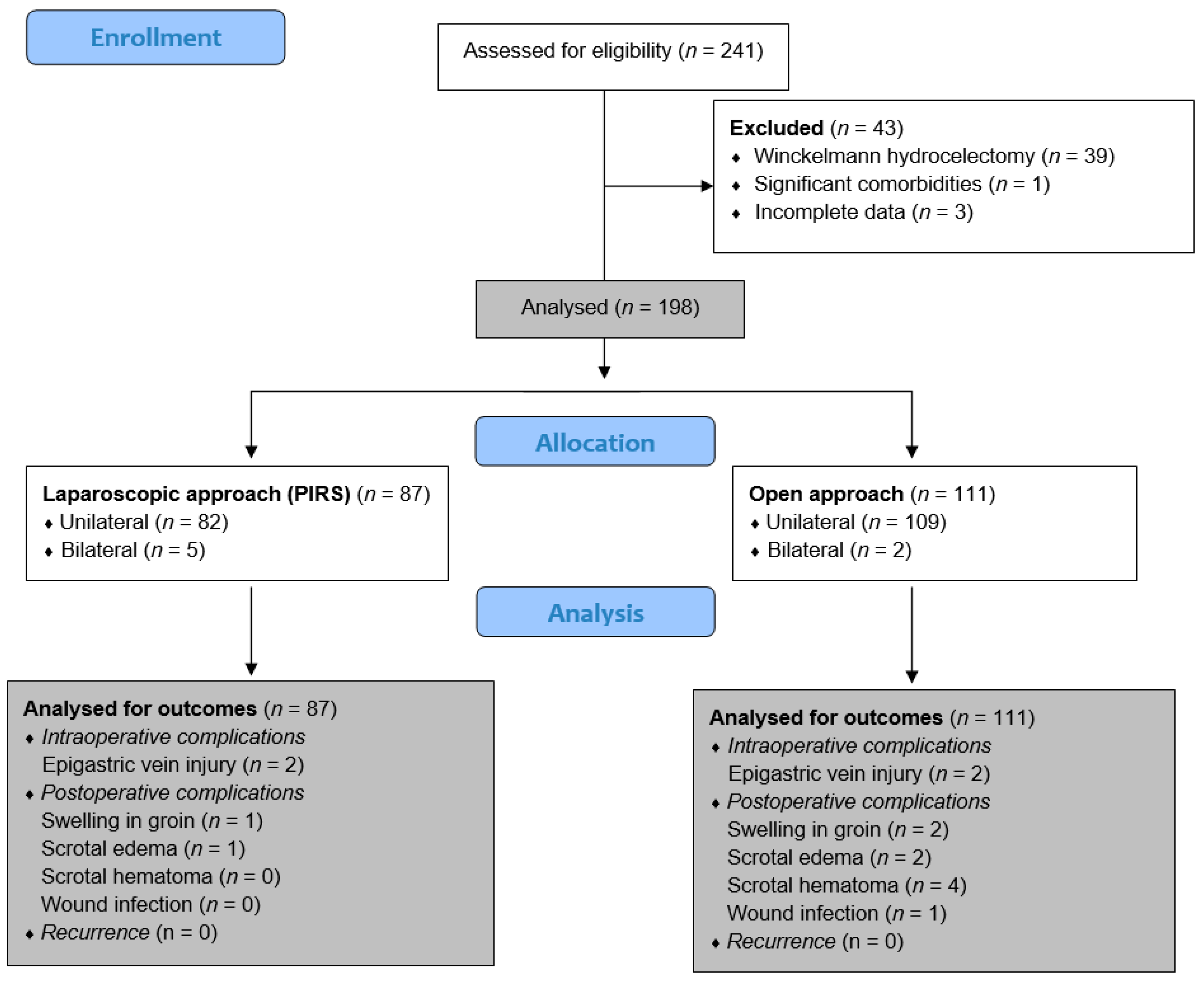
2.4. Study Design
2.5. Surgical Techniques
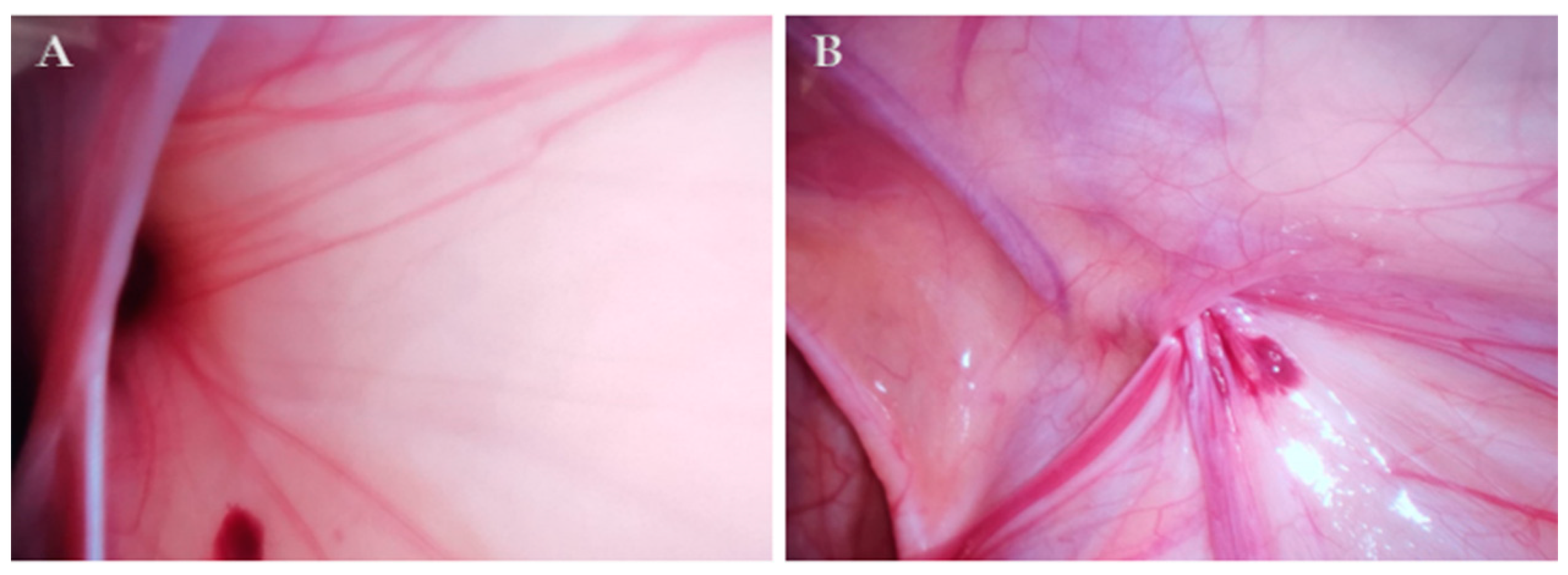
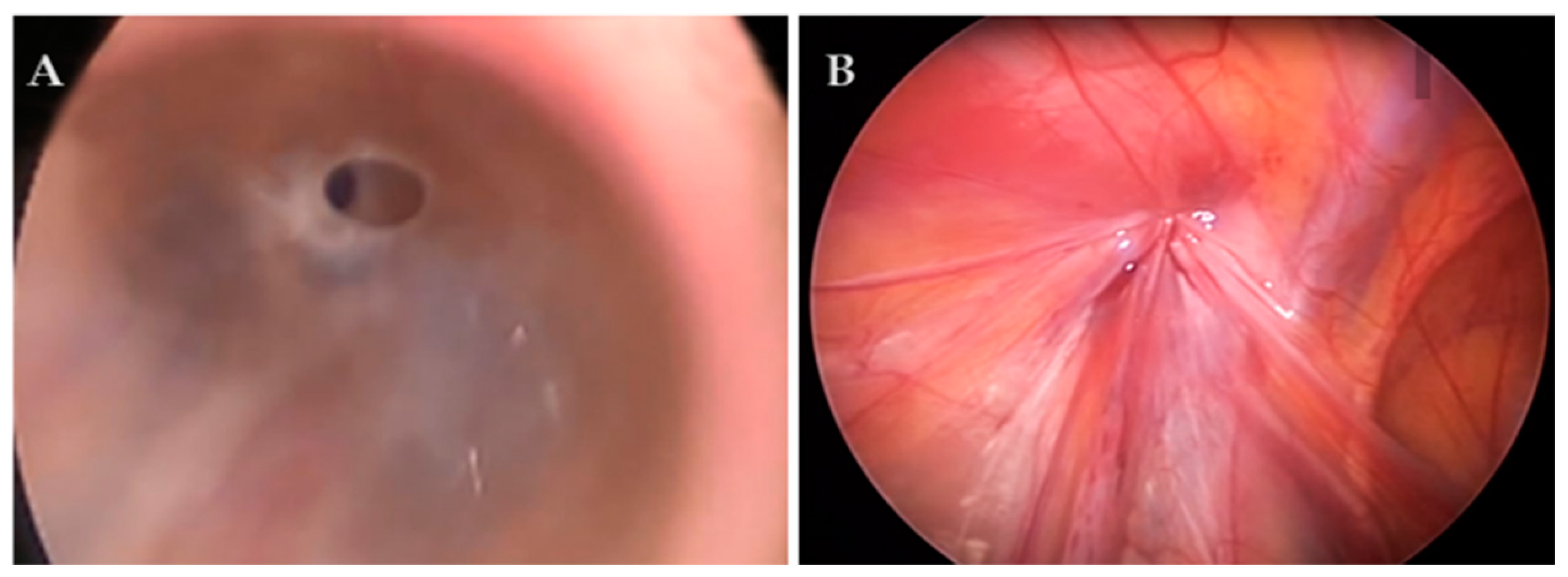
2.5.1. Percutaneous Internal Ring Suturing (PIRS)
2.5.2. Ligation of Patent Processus Vaginalis (PPV)
2.6. Postoperative Protocol and Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Clinical Data of the Patients
3.2. Outcomes of Treatment of the Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cimador, M.; Castagnetti, M.; De Grazia, E. Management of hydrocele in adolescent patients. Nat. Rev. Urol. 2010, 7, 379–385. [Google Scholar] [CrossRef]
- Hoang, V.T.; Van, H.A.T.; Hoang, T.H.; Nguyen, T.T.T.; Trinh, C.T. A review of classification, diagnosis, and management of hydrocele. J. Ultrasound Med. 2023, 43, 599–607. [Google Scholar] [CrossRef]
- Patil, V.; Shetty, S.M.; Das, S. Common and uncommon presentation of fluid within the scrotal spaces. Ultrasound Int. Open. 2015, 1, E34–E40. [Google Scholar] [CrossRef] [PubMed]
- Patoulias, I.; Koutsogiannis, E.; Panopoulos, I.; Michou, P.; Feidantsis, T.; Patoulias, D. Hydrocele in pediatric population. Acta Medica (Hradec Kralove) 2020, 63, 57–62. [Google Scholar] [CrossRef]
- Elhaddad, A.; Awad, M.; Shehata, S.M.; Shehata, M.A. Laparoscopic management of infantile hydrocele in pediatric age group. Pediatr. Surg. Int. 2022, 38, 581–587. [Google Scholar] [CrossRef]
- Christensen, T.; Cartwright, P.C.; Devries, C.; Snow, B.W. New onset of hydroceles in boys over 1 year of age. Int. J. Urol. 2006, 13, 1425–1427. [Google Scholar] [CrossRef]
- International Pediatric Endosurgery Group. IPEG guidelines for inguinal hernia and hydrocele. J. Laparoendosc. Adv. Surg. Technol. A 2010, 20, x–xiv. [Google Scholar] [CrossRef]
- Zhang, Y.; Chao, M.; Zhang, X.; Wang, Z.; Fan, D.; Zhang, K.; Cai, Y.; Liang, C. Does the laparoscopic treatment of paediatric hydroceles represent a better alternative to the traditional open repair technique? A retrospective study of 1332 surgeries performed at two centres in China. Hernia 2018, 22, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Li, C.; Lin, W.; Xu, L. Application of a laparoscopic, single-port, double-needle technique for pediatric hydroceles with multiple peritoneal folds: A trial from a single-center 5-year experience. Urology 2015, 85, 1466–1470. [Google Scholar] [CrossRef]
- Janetschek, G.; Reissigl, A.; Bartsch, G. Laparoscopic repair of pediatric hydroceles. J. Endourol. 1994, 8, 415–417. [Google Scholar] [CrossRef]
- Wang, Z.; Xu, L.; Chen, Z.; Yao, C.; Su, Z. Modified single-port minilaparoscopic extraperitoneal repair for pediatric hydrocele: A single-center experience with 279 surgeries. World J. Urol. 2014, 32, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wu, R.; Du, G. Single-port laparoscopic extraperitoneal repair of pediatric inguinal hernias and hydroceles by using modified Kirschner pin: A novel technique. Hernia 2014, 18, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Tang, R.; Wang, X.; Sui, B.; Jin, Z.; Xu, X.; Zhu, Q.; Chen, J.; Ma, H.; Duan, G. Laparoscopic vs. open repair surgery for the treatment of communicating hydrocele in children: A retrospective study from a single center. Front. Surg. 2021, 8, 671301. [Google Scholar] [CrossRef] [PubMed]
- Baradaran, N.; Wood, C.M.; McCoy, O.O.; Prasad, M.M.; Stec, A.A. Laparoscopic intra-abdominal patent processus vaginalis ligation in pediatric urology practice. J. Pediatr. Urol. 2017, 13, 512.e1–512.e6. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; Escolino, M.; Turrà, F.; Roberti, A.; Cerulo, M.; Farina, A.; Caiazzo, S.; Cortese, G.; Servillo, G.; Settimi, A. Current concepts in the management of inguinal hernia and hydrocele in pediatric patients in laparoscopic era. Semin. Pediatr. Surg. 2016, 25, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Alp, B.F.; Irkilata, H.C.; Kibar, Y.; Zorba, U.; Sancaktutar, A.A.; Kaya, E.; Dayanc, M. Comparison of the inguinal and scrotal approaches for the treatment of communicating hydrocele in children. Kaohsiung J. Med. Sci. 2014, 30, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Jukic, M.; Pogorelic, Z.; Supe-Domic, D.; Jeroncic, A. Comparison of inflammatory stress response between laparoscopic and open approach for pediatric inguinal hernia repair in children. Surg. Endosc. 2019, 33, 3243–3250. [Google Scholar] [CrossRef] [PubMed]
- Srsen, D.; Druzijanic, N.; Pogorelić, Z.; Perko, Z.; Juricic, J.; Kraljevic, D.; Krnic, D.; Bilan, K.; Mimica, Z. Quality of life analysis after open and laparoscopic inguinal hernia repair-retrospective study. Hepatogastroenterology 2008, 55, 2112–2115. [Google Scholar]
- Oral, A.; Karaca, L.; Ahiskalioglu, A.; Yildiz, A.; Yigiter, M.; Celikkaya, M.E.; Chyndolotov, T.; Salman, A.B. Effects of laparoscopic hernia repair by PIRS (Percutan Internal Ring Suturing) technique on testicular artery blood supply. J. Invest. Surg. 2019, 32, 343–347. [Google Scholar] [CrossRef]
- Wu, S.; Xing, X.; He, R.; Zhao, H.; Zhong, L.; Sun, J. Comparison of laparoscope-assisted single-needle laparoscopic percutaneous extraperitoneal closure versus open repair for pediatric inguinal hernia. BMC Surg. 2022, 22, 334. [Google Scholar] [CrossRef]
- Patkowski, D.; Czernik, J.; Chrzan, R.; Jaworski, W.; Apoznański, W. Percutaneous internal ring suturing: A simple minimally invasive technique for inguinal hernia repair in children. J. Laparoendosc. Adv. Surg. Technol. A 2006, 16, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Erginel, B.; Akin, M.; Yildiz, A.; Karadag, C.A.; Sever, N.; Dokucu, A.I. Percutaneous internal ring suturing as a first choice laparoscopic inguinal hernia repair method in girls: A single-center study in 148 patients. Pediatr. Surg. Int. 2016, 32, 697–700. [Google Scholar] [CrossRef] [PubMed]
- Rao, R.; Smith, M.; Markel, T.A.; Gray, B.W.; Landman, M.P. Modified percutaneous internal ring suturing with peritoneal injury in children: Matched comparison to open hernia repair. Surg. Endosc. 2021, 35, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Wolak, P.K.; Strzelecka, A.; Piotrowska-Gall, A.; Wolak, P.P.; Piotrowska, I.; Dąbrowska, K.; Wróbel, J.; Nowak-Starz, G. Percutaneous Internal Ring Suturing (PIRS)—The Benefits of Laparoscopic Inguinal Hernia Repair. Ther. Clin. Risk Manag. 2022, 18, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Meguid, R.A.; Hosokawa, P.W.; Henderson, W.G.; Hammermeister, K.E.; Schulick, R.D.; Shelstad, R.C.; Wild, T.T.; McIntyre, R.C., Jr. An institutional analysis of unplanned return to the operating room to identify areas for quality improvement. Am. J. Surg. 2017, 214, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mears, A.L.; Bisharat, M.; Murphy, F.; Sinha, C.K. Readmission within 30 days of discharge (ReAd): A quality-of-care indicator in paediatric surgery. Pediatr. Surg. Int. 2019, 35, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Kurobe, M.; Harada, A.; Sugihara, T.; Baba, Y.; Hiramatsu, T.; Ohashi, S.; Otsuka, M. The outcomes of conservative management and the natural history of asymptomatic hydroceles in children. Pediatr. Surg. Int. 2020, 36, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Rikalo, M.; Jukić, M.; Katić, J.; Jurić, I.; Furlan, D.; Budimir, D.; Biočić, M. Modified Marcy repair for indirect inguinal hernia in children: A 24-year single-center experience of 6826 pediatric patients. Surg. Today 2017, 47, 108–113. [Google Scholar] [CrossRef]
- Chang, Y.T.; Lee, J.Y.; Wang, J.Y.; Chiou, C.S.; Chang, C.C. Hydrocele of the spermatic cord in infants and children: Its particular characteristics. Urology 2010, 76, 82–86. [Google Scholar] [CrossRef]
- Nevešćanin, A.; Vickov, J.; Elezović Baloević, S.; Pogorelić, Z. Laryngeal mask airway versus tracheal intubation for laparoscopic hernia repair in children: Analysis of respiratory complications. J. Laparoendosc. Adv. Surg. Technol. A 2020, 30, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Čohadžić, T.; Jukić, M.; Nevešćanin Biliškov, A. Percutaneous Internal Ring Suturing for the minimal invasive treatment of pediatric inguinal hernia: A 5-year single surgeon experience. Surg. Laparosc. Endosc. Percutan Technol. 2021, 31, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.D.; Wu, Y.; Xiang, B.; Wong, K.; Pei, J.; Li, F.Y. Ten year experience of laparoscopic repair of pediatric hydrocele and the long-term follow-up results. J. Pediatr. Surg. 2015, 50, 1987–1990. [Google Scholar] [CrossRef] [PubMed]
- Montupet, P.; Esposito, C. Fifteen years experience in laparoscopic inguinal hernia repair in pediatric patients. Results Consid. A Debated Procedure. Surg. Endosc. 2011, 25, 450–453. [Google Scholar] [CrossRef]
- Chang, H.K. Percutaneous Internal Ring Suturing for indirect inguinal hernia in pediatric patients. J. Minim. Invasive Surg. 2020, 23, 63–64. [Google Scholar] [CrossRef]
- Wang, K.; Cai, J.; Lu, Y.C.; Li, X.W.; Zhai, G.M.; He, W.B.; Guo, X.S.; Wu, G.Q. A faster and simpler operation method for laparoscopic inguinal hernia repair in children. J. Laparoendosc. Adv. Surg. Technol. A 2020, 30, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Huskić, D.; Čohadžić, T.; Jukić, M.; Šušnjar, T. Learning curve for laparoscopic repair of pediatric inguinal hernia using percutaneous internal ring suturing. Children 2021, 8, 294. [Google Scholar] [CrossRef]
- Thomas, D.T.; Göcmen, K.B.; Tulgar, S.; Boga, I. Percutaneous internal ring suturing is a safe and effective method for the minimal invasive treatment of pediatric inguinal hernia: Experience with 250 cases. J. Pediatr. Surg. 2016, 51, 1330–1335. [Google Scholar] [CrossRef]
- Choi, B.S.; Byun, G.Y.; Hwang, S.B.; Koo, B.H.; Lee, S.R. A comparison between totally laparoscopic hydrocelectomy and scrotal incision hydrocelectomy with laparoscopic high ligation for pediatric cord hydrocele. Surg. Endosc. 2017, 31, 5159–5165. [Google Scholar] [CrossRef]
- Saka, R.; Okuyama, H.; Sasaki, T.; Nose, S.; Yoneyama, C.; Tsukada, R. Laparoscopic treatment of pediatric hydrocele and the evaluation of the internal inguinal ring. J. Laparoendosc. Adv. Surg. Technol. A 2014, 24, 664–668. [Google Scholar] [CrossRef]
- Horeman-Franse, T.; Postema, R.R.; Fischer, T.; Calleja-Agius, J.; Camenzuli, C.; Alvino, L.; Hardon, S.F.; Bonjer, H.J. The relevance of reducing Veress needle overshooting. Sci. Rep. 2023, 13, 17471. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables Median (IQR) or n (%) | Group I (n = 87) | Group II (n = 111) | p |
|---|---|---|---|
| PIRS | Open Surgery | ||
| Age (months) | 3 (3, 4) | 4 (3, 5) | 0.002 * |
| Weight (kg) | 19 (16, 21) | 21 (20, 26) | <0.001 * |
| Height (cm) | 111 (101, 117) | 120 (111, 131) | <0.001 * |
| BMI (kg/m2) | 15.2 (14, 16.4) | 15.5 (14.3, 16.3) | 0.447 * |
| Lateralization | |||
| Right | 59 (67.8) | 70 (63.1) | 0.174 † |
| Left | 23 (26.4) | 39 (35.1) | |
| Bilateral | 5 (5.8) | 2 (1.8) | |
| ASA classification | 0.891 ‡ | ||
| ASA I | 82 (94.2) | 104 (93.7) | |
| ASA II | 5 (5.8) | 7 (6.3) | |
| Comorbidities | 7 (8.1) | 7 (6.3) | 0.771 ‡ |
| Type of Hydrocele | Group I (n = 92) * |
|---|---|
| PIRS; n (%) | |
| Type I (Closed ring—No communication to PC) | 0 (0) |
| Type II (Patent ring—Direct communication to PC) | |
| Type II A (Wide opening) | 69 (75) |
| Type II B (Ring covered by peritoneal seal) | 4 (4.3) |
| Type II C (Pinhole) | 14 (15.3) |
| Type III (Patent ring—No communication to PC) | |
| Type III A (Solitary cyst) | 4 (4.3) |
| Type III B (Multiple cysts) | 1 (1.1) |
| Variables Median (IQR) or n (%) | Group I (n = 87) ‡ | Group II (n = 111) ‡ | p |
|---|---|---|---|
| PIRS | Open Surgery | ||
| Duration of surgery (min) | 15 (10, 17) | 21 (15, 25) | <0.001 * |
| Duration of anesthesia (min) | 30 (25, 40) | 40 (35, 40) | <0.001 * |
| Intraoperative complications | >0.999 † | ||
| Epigastric vein injury | 2 (2.3) | 2 (1.8) | |
| Postoperative complications | 2 (2.3) | 7 (6.3) | 0.190 † |
| Swelling in groin | 1 | 0 | |
| Scrotal edema | 1 | 2 | |
| Scrotal hematoma | 0 | 4 | |
| Wound infection | 0 | 1 | |
| Length of hospital stay (h) | 9 (8, 12) | 24 (12, 24) | <0.001 * |
| Recurrence | 0 (0) | 0 (0) | - |
| Follow-up (months) | 30 (15, 38) | 32 (15, 49) | 0.395 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pogorelić, Z.; Stanić, P.; Bašković, M. Comparison of Percutaneous Internal Ring Suturing (PIRS) versus Open Ligation of the Patent Processus Vaginalis for the Treatment of Communicating Pediatric Hydrocele. Children 2024, 11, 437. https://doi.org/10.3390/children11040437
Pogorelić Z, Stanić P, Bašković M. Comparison of Percutaneous Internal Ring Suturing (PIRS) versus Open Ligation of the Patent Processus Vaginalis for the Treatment of Communicating Pediatric Hydrocele. Children. 2024; 11(4):437. https://doi.org/10.3390/children11040437
Chicago/Turabian StylePogorelić, Zenon, Petar Stanić, and Marko Bašković. 2024. "Comparison of Percutaneous Internal Ring Suturing (PIRS) versus Open Ligation of the Patent Processus Vaginalis for the Treatment of Communicating Pediatric Hydrocele" Children 11, no. 4: 437. https://doi.org/10.3390/children11040437
APA StylePogorelić, Z., Stanić, P., & Bašković, M. (2024). Comparison of Percutaneous Internal Ring Suturing (PIRS) versus Open Ligation of the Patent Processus Vaginalis for the Treatment of Communicating Pediatric Hydrocele. Children, 11(4), 437. https://doi.org/10.3390/children11040437