
Severe Crowding Associated with Lower Canine Premature Resorption: Interceptive Treatment with Clear Aligners—A Pilot Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Treatment Protocol
2.2. Measurements
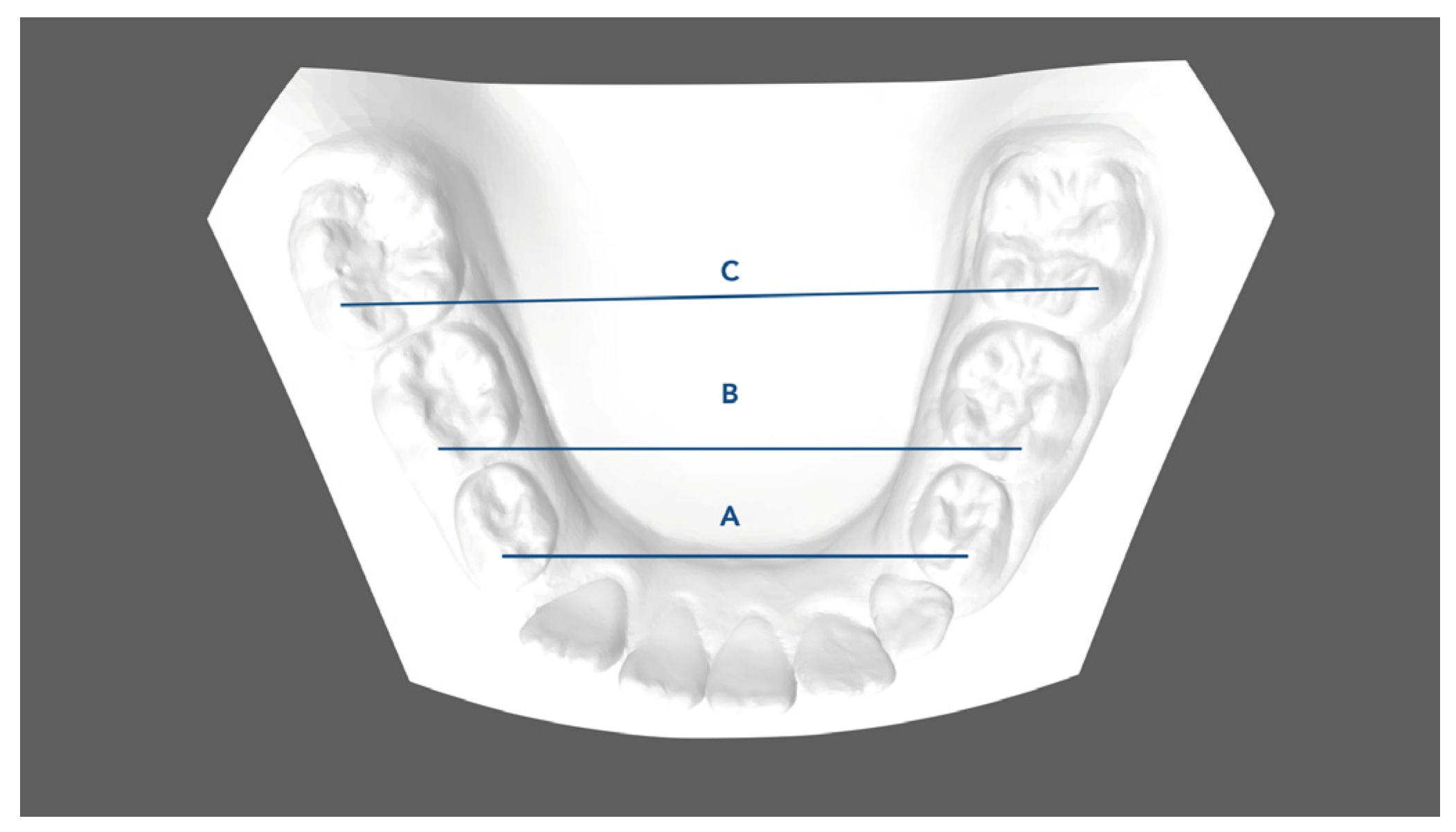
- Mandibular first deciduous inter-molar width (IV–IV): linear distance evaluated between the mesio-buccal cusp tips of the right and left mandibular first deciduous molars;
- Mandibular second deciduous inter-molar width (V–V): linear distance evaluated between the mesio-buccal cusp tips of the right and left mandibular second deciduous molars;
- Mandibular inter-molar width (6–6): linear distance evaluated between the mesio-buccal cusp tips of the right and left mandibular first permanent molars;
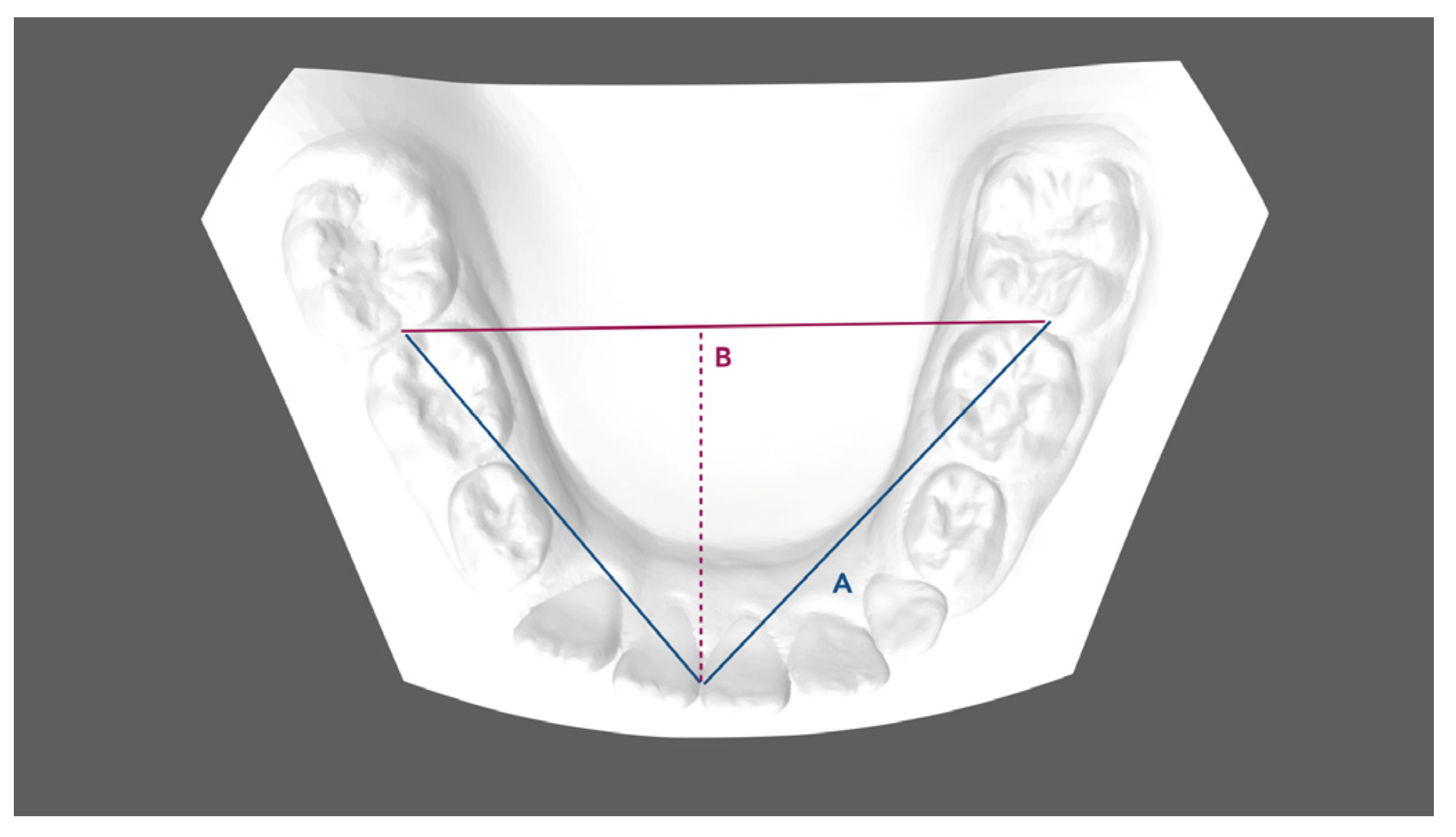
- Arch length: sum of the right and left distances traced from mesial anatomic contact points of the first permanent molars to the contact point of the central incisors;
- Arch depth: perpendicular length from the midpoint drawn between the mandibular central incisors to the line drawn between the mesial anatomic contact points of the first molars;
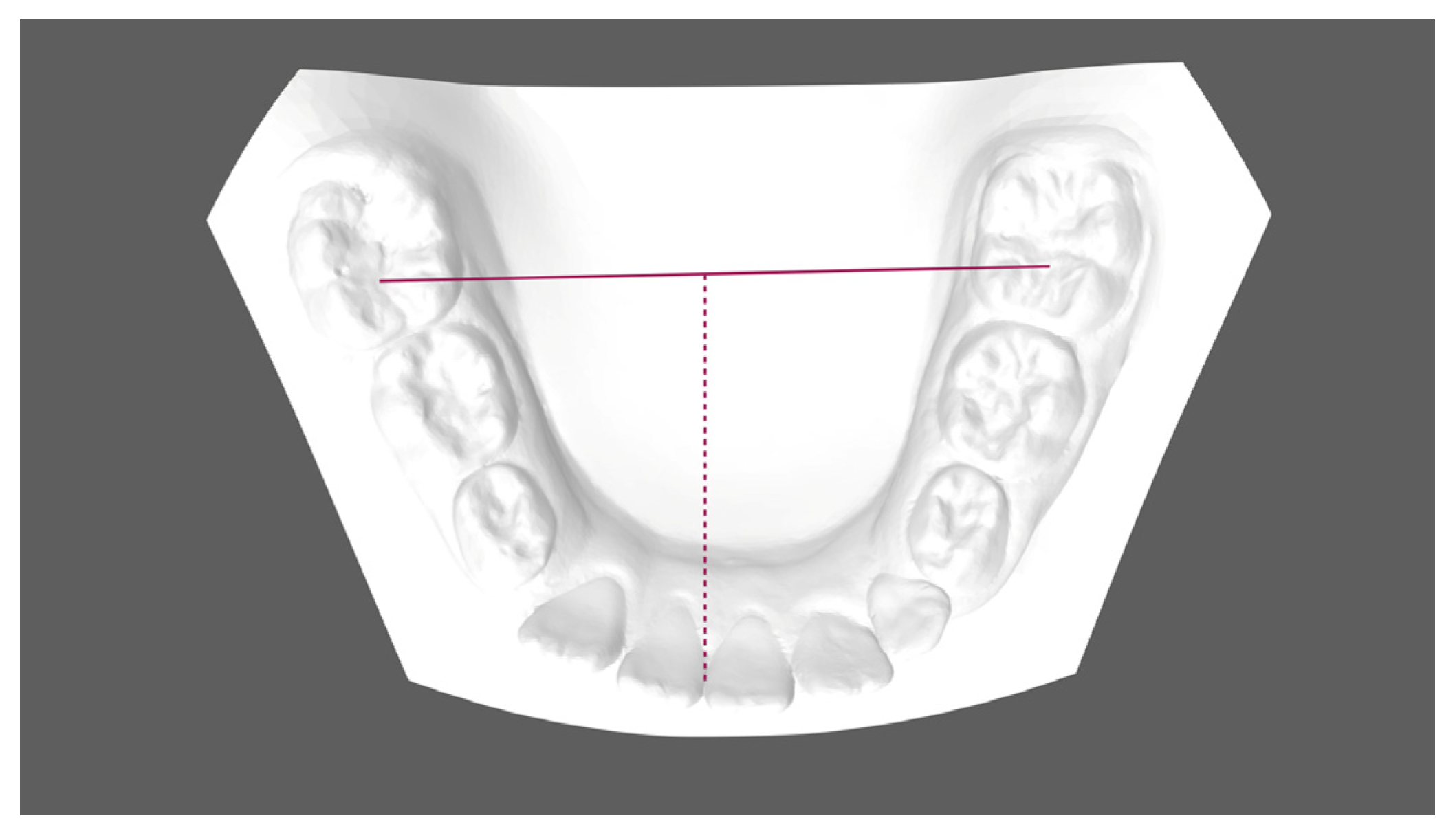
- Midline discrepancy: difference between the initial and final position of the lower midline. The mandibular midline position was determined by measuring the distance between the contact point of the central incisors and the first molar central fossa line.
- IMPA (°): angle between the long axis of the lower incisor and the mandibular plane (Go-Me).
- L1-APg (mm): linear distance between the lower crown tip and the A-Pg line.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- -
- Atypical Premature Root Canine Resorption (APRCP) is a clinical sign of primary crowding, which requires accurate space management during early mixed dentition.
- -
- Early treatment with clear aligners represents a valid treatment strategy in early mixed dentition to manage arch and occlusion development.
- -
- The combination of transversal arch development, control of permanent incisor inclination, maintenance of leeway space, and guidance of eruption allows the early recovery of anterior dental crowing and arch length discrepancies.
- -
- Further studies with larger sample sizes and longer observational periods are needed to strengthen the described dentoalveolar changes.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nadelman, P.; Magno, M.B.; Pithon, M.M.; de Castro, A.C.R.; Maia, L.C. Does the premature loss of primary anterior teeth cause morphological, functional and psychosocial consequences? Braz. Oral Res. 2021, 35, e092. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R.; Fields, H.W.; Sarver, D.M.; Ackerman, J.L. Contemporary Orthodontics, 5th ed.; Elsevier: St. Louis, MO, USA, 2013; pp. 137–139, 417–418, 427. [Google Scholar]
- Foley, T.F.; Wright, G.Z.; Weinberger, S.J. Management of lower incisor crowding in the early mixed dentition. ASDC J. Dent. Child. 1996, 63, 169–174. [Google Scholar] [PubMed]
- Christensen, R.T.; Fields, H.W.; Christensen, J.R.; Beck, F.M.; Casamassimo, P.S.; McTigue, D.J. The Effects of Primary Canine Loss on Permanent Lower Dental Midline Stability. Pediatr. Dent. 2018, 40, 279–284. [Google Scholar] [PubMed]
- Moorrees, C.F.; Chadha, J.M. Available space for the incisors during dental development-a growth study based on physiologic age. Angle Orthod. 1965, 35, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Pinkham, J.R.; Casamassimo, P.S.; Fields, H.W.; McTigue, D.J.; Nowak, A.J. Pediatric Dentistry: Infancy through Adolescence, 5th ed.; Elsevier: St. Louis, MO, USA, 2005; pp. 270, 385–392. [Google Scholar]
- Sayin, M.O.; Türkkahraman, H. Effects of lower primary canine extraction on the mandibular dentition. Angle Orthod. 2006, 76, 31–35. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, F.P.G.M. Development of the Human Dentition; Quintessence Pub Co., Inc.: Hanover Park, IL, USA, 2016. [Google Scholar]
- McDonald, R.E.; Avery, D.R.; Dean, J.A. Managing the developing occlusion. In McDonald and Avery’s Dentistry for the Child and Adolescent, 9th ed.; Mosby/Elsevier: Maryland Heights, MO, USA, 2011; pp. 545–609. [Google Scholar]
- Gianelly, A.A. Treatment of crowding in the mixed dentition. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 569–571. [Google Scholar] [CrossRef] [PubMed]
- Gellin, M.E. Conservative treatment for malaligned permanent mandibular incisors in the early mixed dentition. ASDC J. Dent. Child. 1989, 56, 288–292. [Google Scholar] [PubMed]
- Hollander, C.S.; Full, C.A. Midline correction by extraction of the remaining mandibular canine: Myth or reality. ASDC J. Dent. Child. 1992, 59, 207–211. [Google Scholar] [PubMed]
- Lee, K.P. Behavior or erupting crowded lower incisors. J. Clin. Orthod. 1980, 14, 24–33. [Google Scholar]
- Owen, D.G. The incidence and nature of space closure following the premature extraction of deciduous teeth: A literature study. Am. J. Orthod. Dentofac. Orthop. 1971, 59, 37–49. [Google Scholar] [CrossRef]
- Lombardo, E.C.; Paoloni, V.; Fanelli, S.; Pavoni, C.; Gazzani, F.; Cozza, P. Evaluation of the Upper Arch Morphological Changes after Two Different Protocols of Expansion in Early Mixed Dentition: Rapid Maxillary Expansion and Invisalign® First System. Life 2022, 12, 1323. [Google Scholar] [CrossRef] [PubMed]
- Pavoni, C.; Gazzani, F.; Franchi, L.; Loberto, S.; Lione, R.; Cozza, P. Soft tissue facial profile in Class III malocclusion: Long-term post-pubertal effects produced by the Face Mask Protocol. Eur. J. Orthod. 2019, 41, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Kau, C.H.; Durning, P.; Richmond, S.; Miotti, F.A.; Harzer, W. Extractions as a form of interception in the developing dentition: A randomized controlled trial. J. Orthod. 2004, 31, 107–114. [Google Scholar] [CrossRef] [PubMed]
- McDonald, R.E.; Avery, D.R. McDonald and Avery’s Dentistry for the Child and Adolescent, 10th ed.; Elsevier: St. Louis, MO, USA, 2016; p. 425. [Google Scholar]
- Fleming, P.S. Timing orthodontic treatment: Early or Late? Aust. Dent. J. 2017, 62 (Suppl. S1), 11–19. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.; Sonis, A. Space Supervision and Guidance of Eruption in Management of Lower Transitional Crowding: A Non-extraction Approach. Semin. Orthod. 2014, 20, 16–35. [Google Scholar] [CrossRef]
- Pinho, T.; Rocha, D.; Ribeiro, S.; Monteiro, F.; Pascoal, S.; Azevedo, R. Interceptive Treatment with Invisalign® First in Moderate and Severe Cases: A Case Series. Children 2022, 9, 1176. [Google Scholar] [CrossRef] [PubMed]
- Lione, R.; Paoloni, V.; Bartolommei, L.; Gazzani, F.; Meuli, S.; Pavoni, C.; Cozza, P. Maxillary arch development with Invisalign System: Analysis of expansion dental movements on digital dental casts. Angle Orthod. 2021, 91, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the sample size for a pilot randomized trial to minimize the overall sample size for the external pilot and main trial for a continuous variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef] [PubMed]
- Lione, R.; Gazzani, F.; Moretti, S.; Danesi, C.; Cretella Lombardo, E.; Pavoni, C. Gingival Margins’ Modifications during Orthodontic Treatment with Invisalign First®: A Preliminary Study. Children 2022, 9, 1423. [Google Scholar] [CrossRef]
- Van der Linden, F.P.G.M. Desenvolvimento da Dentição, 1st ed.; Santos: São Paulo, Brazil, 1986; pp. 129–153. [Google Scholar]
- Kapala, J.T. Ortodoncia interceptativa y manejo de los problemas de espacio. Odontol. Pediatr. 1984, 18, 378–419. [Google Scholar]
- Ericson, S.; Kurol, J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur. J. Orthod. 1988, 10, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Dugoni, S.A.; Lee, J.S.; Varela, J.; Dugoni, A.A. Early mixed dentition treatment: Post-retention evaluation of stability and relapse. Angle Orthod. 1995, 65, 311–320. [Google Scholar] [PubMed]
- Ngan, P.; Alkire, R.G.; Fields, H. Management of space problems in the primary and mixed dentitions. J. Am. Dent. Assoc. 1999, 130, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Blevins, R. Phase I orthodontic treatment using Invisalign First. J. Clin. Orthod. 2019, 53, 73–83. [Google Scholar] [PubMed]
- Germane, N.; Lindauer, S.J.; Rubenstein, L.K.; Revere, J.H., Jr.; Isaacson, R.J. Increase in arch perimeter due to orthodontic expansion. Am. J. Orthod. Dentofac. Orthop. 1991, 100, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.A. Management of the developing occlusion. In McDonald and Avery’s Dentistry for the Child and Adolescent, 10th ed.; Mosby Elsevier: Maryland Heights, MO, USA, 2015; pp. 415–478. [Google Scholar]
- Brennan, M.M.; Giannelly, A.A. The use of lingual arch in the mixed dentition to resolve incisor crowding. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 81–85. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Management of the Developing Dentition and Occlusion in Pediatric Dentistry. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2017. [Google Scholar]
- Golovcencu, L.; Romanec, C.; Martu, M.A.; Anistoroaiei, D.; Pacurar, M. Particularities of Orthodontic Treatment in Patients with Dental Anomalies That Need Orthodontic—Restorative Therapeutic Approach. Rev. Chim. 2019, 70, 3046–3049. [Google Scholar] [CrossRef]
- Gonçalves, A.; Ayache, S.; Monteiro, F.; Silva, F.S.; Pinho, T. Efficiency of Invisalign First® to promote expansion movement in mixed dentition: A retrospective study and systematic review. Eur. J. Paediatr. Dent. 2023, 24, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Nevant, C.T.; Buschang, P.H.; Alexander, R.G.; Steffen, J.M. Lip bumper therapy for gaining arch length. Am. J. Orthod. Dentofac. Orthop. 1991, 100, 330–336. [Google Scholar] [CrossRef]
- Lione, R.; Pavoni, C.; Laganà, G.; Fanucci, E.; Ottria, L.; Cozza, P. Rapid maxillary expansion: Effects on palatal area investigated by computed tomography in growing subjects. Eur. J. Paediatr. Dent. 2012, 13, 215–218. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Pre-Treatment (T0) | Post-Treatment (T1) | T1–T0 | ||||
| Arch Dimension Measurements (mm) | Mean | SD | Mean | SD | Diff | SD | p Value |
| First inter-deciduous molar width (IV–IV) | 38.2 | 1.4 | 39.8 | 1.8 | 1.6 | 1.5 | 0.01 |
| Second inter-deciduous molar width (V–V) | 29.6 | 0.9 | 31.7 | 2.2 | 2.1 | 1.4 | 0.001 * |
| Mandibular inter-molar width (6–6) | 43.7 | 2.2 | 46.1 | 2.1 | 2.4 | 1.4 | 0.001 * |
| Arch Length | 63.4 | 3.0 | 65.7 | 0.9 | 2.3 | 0.6 | 0.001 * |
| Arch Depth | 27.5 | 2.1 | 32 | 2.2 | 4.5 | 1.6 | 0.05 * |
| Midline Discrepancy | 2.2 | 0.9 | 0.3 | 1.8 | −1.9 | 0.7 | 0.01 * |
| Incisors’ Inclination Changes | Pre-Treatment (T0) | Post-Treatment (T1) | T1–T0 | ||||
| IMPA (°) | 90.6 | 2.5 | 91.8 | 1.2 | 1.2 | 1.3 | 0.5 |
| L1-APg (mm) | 2.3 | 1.9 | 3.9 | 1.9 | 1.6 | 0.5 | 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazzani, F.; Pavoni, C.; Loberto, S.; Caruso, S.; Cozza, P. Severe Crowding Associated with Lower Canine Premature Resorption: Interceptive Treatment with Clear Aligners—A Pilot Study. Children 2024, 11, 451. https://doi.org/10.3390/children11040451
Gazzani F, Pavoni C, Loberto S, Caruso S, Cozza P. Severe Crowding Associated with Lower Canine Premature Resorption: Interceptive Treatment with Clear Aligners—A Pilot Study. Children. 2024; 11(4):451. https://doi.org/10.3390/children11040451
Chicago/Turabian StyleGazzani, Francesca, Chiara Pavoni, Saveria Loberto, Silvia Caruso, and Paola Cozza. 2024. "Severe Crowding Associated with Lower Canine Premature Resorption: Interceptive Treatment with Clear Aligners—A Pilot Study" Children 11, no. 4: 451. https://doi.org/10.3390/children11040451
APA StyleGazzani, F., Pavoni, C., Loberto, S., Caruso, S., & Cozza, P. (2024). Severe Crowding Associated with Lower Canine Premature Resorption: Interceptive Treatment with Clear Aligners—A Pilot Study. Children, 11(4), 451. https://doi.org/10.3390/children11040451