
Risk Factors of Malnutrition among In-School Children and Adolescents in Developing Countries: A Scoping Review
 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Study Design, Data Source and Search Strategy
2.2. Data Extraction
3. Results
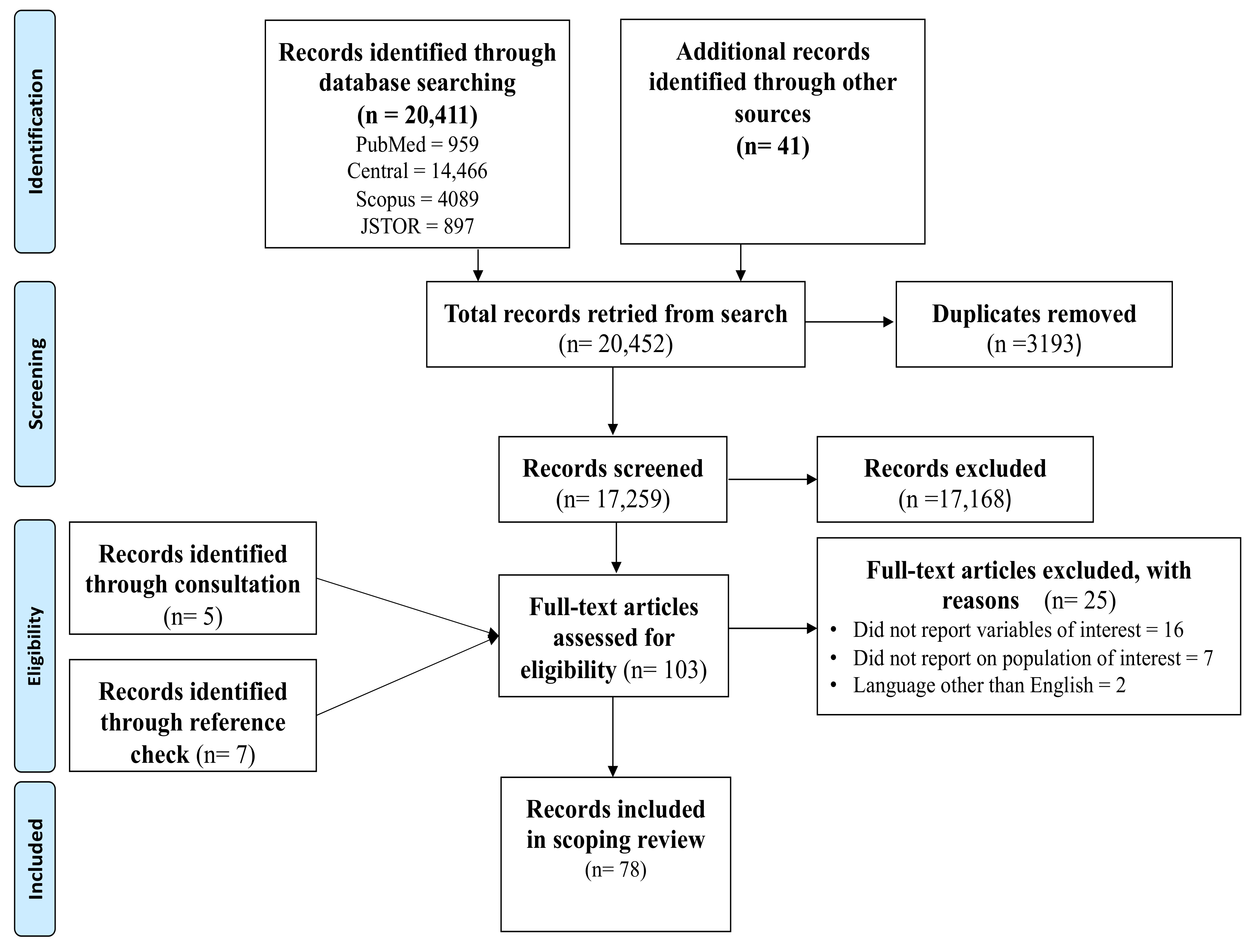
3.1. Search Outcomes
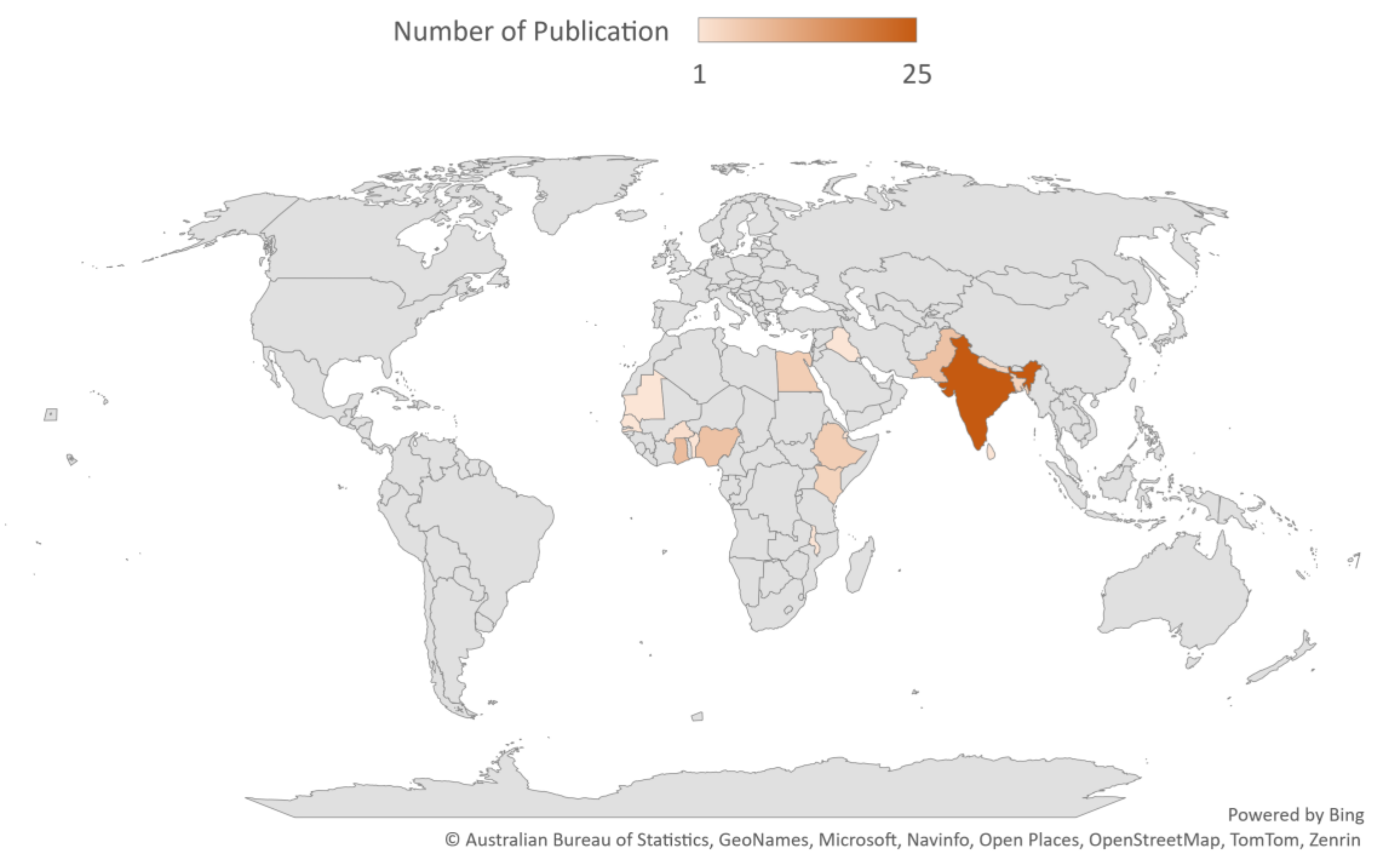
3.2. Characteristics of Included Studies
3.3. Risk Factors of Malnutrition among In-School Children in Developing Countries’ Demographics
3.3.1. Nature of Environment and Sanitation
3.3.2. Knowledge of Practice
3.3.3. Dietary Habits
3.3.4. Nutrient Deficiency and Body Weight
3.3.5. Activity Level
3.3.6. Malaise
3.4. Health Impact of Malnutrition among In-School Children in Developing Countries
3.4.1. General Health Status
3.4.2. Fetal/Maternal Health and Morbidity
3.4.3. Gender Discrimination
3.4.4. Nutritional Deficiency and Specific Body Systems
3.5. Impact of Malnutrition on School Performance and Attendance of In-School Children in Developing Countries
3.5.1. School Performance
3.5.2. School Attendance
4. Discussion
4.1. Summary of Findings
4.2. Risk Factors of Malnutrition among In-School Children in Developing Countries
4.3. Health Impact of Malnutrition on In-School Children in Developing Countries
4.4. Impact of Malnutrition on Educational Outcomes of In-School Children in Developing Countries
4.5. Limitations
4.6. Implications for Policy and Practice
4.7. Recommendations for Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- UNICEF. Global Nutrition Report 2020. 2020. Available online: https://data.unicef.org/resources/global-nutrition-report-2020/ (accessed on 8 January 2024).
- WHO. Fact Sheets—Malnutrition 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 8 January 2024).
- Elia, M. Defining, Recognizing, and Reporting Malnutrition. Int. J. Low. Extremity Wounds 2017, 16, 230–237. [Google Scholar] [CrossRef]
- De, P.; Chattopadhyay, N. Effects of malnutrition on child development: Evidence from a backward district of India. Clin. Epidemiology Glob. Health 2019, 7, 439–445. [Google Scholar] [CrossRef]
- Nugent, R.; Levin, C.; Hale, J.; Hutchinson, B. Economic effects of the double burden of malnutrition. Lancet 2020, 395, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.N.; Kufeldt, J.; Kisser, U.; Hornung, H.-M.; Hoffmann, J.; Andraschko, M.; Werner, J.; Rittler, P. Effects of malnutrition on complication rates, length of hospital stay, and revenue in elective surgical patients in the G-DRG-system. Nutrition 2016, 32, 249–254. [Google Scholar] [CrossRef]
- UNESCO. Universal Access to Education: We Can Do Better 2021. Available online: https://courier.unesco.org/en/articles/universal-access-education-we-can-do-better (accessed on 8 January 2024).
- Ghosh, S.; Chowdhury, S.D.; Chandra, A.M.; Ghosh, T. Grades of undernutrition and socioeconomic status influence cognitive development in school children of Kolkata. Am. J. Phys. Anthr. 2015, 156, 274–285. [Google Scholar] [CrossRef]
- Jumilia, J.; Cleodora, C.; Widyastuti, M. Analysis of the Impact of Stunting on Psychosocial Development in Pre-School Children in the Working Area Seberang Padang Community Health Center. J. Keperawatan Komprehensif (Compr. Nurs. J.) 2023, 9, 298–310. [Google Scholar] [CrossRef]
- Safaei, M.; Sundararajan, E.A.; Driss, M.; Boulila, W.; Shapi’I, A. A systematic literature review on obesity: Understanding the causes & consequences of obesity and reviewing various machine learning approaches used to predict obesity. Comput. Biol. Med. 2021, 136, 104754. [Google Scholar] [CrossRef]
- Mbogori, T.; Kimmel, K.; Zhang, M.; Kandiah, J.; Wang, Y. Nutrition transition and double burden of malnutrition in Africa: A case study of four selected countries with different social economic development. AIMS Public Health 2020, 7, 425–439. [Google Scholar] [CrossRef]
- Bourke, C.D.; Berkley, J.A.; Prendergast, A.J. Immune Dysfunction as a Cause and Consequence of Malnutrition. Trends Immunol. 2016, 37, 386–398. [Google Scholar] [CrossRef]
- Soliman, A.; De Sanctis, V.; Alaaraj, N.; Ahmed, S.; Alyafei, F.; Hamed, N.; Soliman, N. Early and Long-term Consequences of Nutritional Stunting: From Childhood to Adulthood. Acta Biomed. 2021, 92, e2021168. [Google Scholar] [CrossRef]
- Siddiqui, F.; Salam, R.A.; Lassi, Z.S.; Das, J.K. The Intertwined Relationship Between Malnutrition and Poverty. Front. Public Health 2020, 8, 525026. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Khanam, S.J.; Haque, A. Prevalence and determinants of malnutrition among primary school going children in the haor areas of Kishoreganj district of Bangladesh. Heliyon 2021, 7, e08077. [Google Scholar] [CrossRef] [PubMed]
- Damie, T.; Kbebew, M.; Teklehaymanot, A. Nutritional status and associated factors among school adolescent in Chiro Town, West Hararge, Ethiopia. Gaziantep Med. J. 2015, 21, 32. [Google Scholar] [CrossRef]
- Kumari, S. Nutritional Deficiency Disorders Among Primary School Going Children: A Case Study of Rural Darbhanga Village. Int. J. Home Sci. 2021, 7, 238–241. [Google Scholar]
- Aisha, I.A.; Alka, G.; Virginia, P. Prevalence of vitamin A deficiency among school going children aged 6–12 years. Pharma Innov. J. 2018, 7, 412–415. [Google Scholar]
- David, M.D.; Kimiywe, J.; Waudo, J. Nutritional knowledge, attitude and practices and nutritional status of school-going children in Machakos district, Kenya. Int. Conf. Nutr. Food Sci. 2012, 39, 147–152. [Google Scholar]
- Mondal, N.; Basumatary, B.; Kropi, J.; Bose, K. Prevalence of double burden of malnutrition among urban school going bodo children aged 5–11 years of Assam, Northeast India. Epidemiol. Biostat. Public Health 2015, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Daboné, C.; Delisle, H.F.; Receveur, O. Poor nutritional status of schoolchildren in urban and peri-urban areas of Ouagadougou (Burkina Faso). Nutr. J. 2011, 10, 34. [Google Scholar] [CrossRef]
- Aurisinkala-Appadoo, S.; University of Mauritius; Oogarah-Pratap, B.; Ruggoo, A. Mauritius Institute of Education Nutritional status of school children aged 8–12 years in deprived areas of Mauritius. Afr. J. Food, Agric. Nutr. Dev. 2013, 13, 8077–8090. [Google Scholar]
- Opini, R.B.; Kiplangat, J.M.; Muturi, S.K. Nutritional status and associated factors among school going children aged 4–10 years in kisii central sub-county. East Afr. Med. J. 2016, 93, 91–95. [Google Scholar]
- Adegun, J.A.; Ajayi-Vincent, O.B.; Alebiosu, E.O. Differences in the Nutritional Status of Young School Children from Public and Private Owned Primary Schools in Ekiti State, Nigeria. Eur. Sci. J. March 2013, 9, 1857–7881. [Google Scholar]
- Abidoye, R.; Akande, P. Nutritional status of public primary school children: A comparison between an upland and riverine area of Ojo LGA, Lagos State Nigeria. Nutr. Health 2000, 14, 225–240. [Google Scholar] [CrossRef] [PubMed]
- Roba, K.; Abdo, M.; Wakayo, T. Nutritional Status and Its Associated Factors among School Adolescent Girls in Adama City, Central Ethiopia. J. Nutr. Food Sci. 2016, 6, 1000493. [Google Scholar] [CrossRef]
- Bose, A.; Sinha, I.; LataTigga, P.; Nitish, M.; Sen, J. Socio-economic and Demographic Determinants of Double Burden of Malnutrition among Rajbanshi School-going Children aged 9–14 Years from North Bengal, India. Antrocom Online J. Anthropol. 2020, 16, 141–152. [Google Scholar]
- Subramanian, P.; Dasari, S.; Devulapalli, S.; Chitgupiker, S.R. Correlation of Nutrition with Parental Literacy Status among School Going Adolescent Children in Telangana: A Cross-sectional Study. J. Clin. Diagn. Res. 2021, 15, SC13–SC16. [Google Scholar] [CrossRef]
- Hassan, S.K.; Abdelwahed, W.Y.; Eldessouki, R. Nutritional Status and Some Sociodemographic and Lifestyle Characteristics among A Group of Rural School Children in Fayoum Governorate, Egypt. Egypt J. Community Med. 2018, 36, 1–11. [Google Scholar] [CrossRef]
- Twara, T.; Upasna, S.; Agrawal, A.; Dubey, G.P.; Fellow, J.R. Evaluation of Nutritional Status of School Going Tribal Children by Using Anthropometric Measurement in Selected Areas of Eastern Uttar Pradesh. Int. J. Health Sci. Res. 2015, 5, 347. [Google Scholar]
- El-Sabely, A.A.; Tork, H.M.; Hussien, Y.E. Comparative study of nutritional status and dietary habits of children from public and private primary schools in Zagazig City, Egypt. IOSR J. Nurs. Health Sci. 2013, 3, 47–52. [Google Scholar] [CrossRef]
- Sharma, A.; Katoch, O.R. Socioeconomic Factors, Living Conditions and Child Undernutrition among School going Children in Rural Areas of district Doda, Jammu & Kashmir, India: A Preliminary Study. Indian J. Nutr. 2016, 3, 1–7. [Google Scholar]
- Malpani, A.K.; Sarat, S.; Hunchannavar, S.V.; Ade, A. Prevalence of Malnutrition among School Children in Rural Area of North Karnataka Region. Indian J. Pharm. Pract. 2014, 7, 33–36. [Google Scholar] [CrossRef]
- Kadu, K.P.; Kadu, S.K.; Ingle, S.Y. Prevalence of Vitamin A Deficiency in School Going Children in Rural Area. Int. J. Res. Rev. 2021, 8, 1–4. [Google Scholar] [CrossRef]
- Ahsan, S.; Saleh, Z.; Sheikh, S.A.; Fahim, M.F.; Memon, M.S.; Shakil, S. Nutritional Status of School Going Children of 5–15 Years of Age: Urban Slums Scenario in Karachi, Pakistan. Biostat. Biom. Open Access J. 2020, 10, 22–26. [Google Scholar]
- Babar, N.F.; Muzaffar, R.; Khan, M.A.; Imdad, S. Impact of socioeconomic factors on nutritional status in primary school children. J. Ayub Med. Coll. Abbottabad 2010, 22, 15–18. [Google Scholar]
- Bhattarai, S.; Bhusal, C.K. Prevalence and associated factors of malnutrition among school going adolescents of Dang district, Nepal. AIMS Public Health 2019, 6, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Galgamuwa, L.S.; Iddawela, D.; Dharmaratne, S.D.; Galgamuwa, G. Nutritional status and correlated socio-economic factors among preschool and school children in plantation communities, Sri Lanka. BMC Public Health 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ayogu, R.N.; Nnam, N.M.; Ibemesi, O.; Okechukwu, F. Prevalence and factors associated with anthropometric failure, vitamin A and iron deficiency among adolescents in a Nigerian urban community. Afr. Health Sci. 2016, 16, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Ayogu, R.N.B.; Afiaenyi, I.C.; Madukwe, E.U.; Udenta, E.A. Prevalence and predictors of under-nutrition among school children in a rural South-eastern Nigerian community: A cross sectional study. BMC Public Health 2018, 18, 587. [Google Scholar] [CrossRef] [PubMed]
- Agbozo, F.; Atito, P.; Abubakari, A. Malnutrition and associated factors in children: A comparative study between public and private schools in Hohoe Municipality, Ghana. BMC Nutr. 2016, 2, 32. [Google Scholar] [CrossRef]
- Singh, A.; Sharma, A.K.; Kumar, A.; Singh, A.; Khan, S.; Chauhan, N.S. Socio-economic Predisposing Factors of Malnutrition among School Going Children in Bareilly District of North India: A Cross-sectional Study. J. Soc. Behav. Community Health 2022, 6, 786–793. [Google Scholar] [CrossRef]
- Shukla, M.; Ahmad, S.; Shukla, N.K.; Singh, J.V.; Shukla, R. Double burden of malnutrition among school-going adolescent girls in North India: A cross-sectional study. J. Fam. Med. Prim. Care 2018, 7, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, S.B.; Youssef, M.R.L.; Sedrak, A.S.; Labib, J.R. Nutritional Status and Dietary Habits of School Children in Beni-Suef Governorate, Egypt. Food Nutr. Sci. 2015, 6, 54–63. [Google Scholar] [CrossRef]
- Pal, D.; Kanungo, S.; Bal, B.; Bhowmik, K.; Sarkar, T.M.A.K. Malnutrition Scenario among School Children in Eastern-India-an Epidemiological Study. J. Sleep Disord. Ther. 2016, 6, 1000228. [Google Scholar] [CrossRef]
- Degarege, D.; Degarege, A.; Animut, A. Undernutrition and associated risk factors among school age children in Addis Ababa, Ethiopia. BMC Public Health 2015, 15, 375. [Google Scholar] [CrossRef]
- Joshi, H.S.; Katyal, R.; Singh, A.; Khan, S.; Upadhayay, D. An Epidemiological Study on Malnutrition among Primary School-going Children of Rural Area of Bareilly District, Uttar Pradesh, India. Int. J. Adv. Integr. Med. Sci. 2018, 3, 8–11. [Google Scholar] [CrossRef]
- Shashank, K.J.; Chethan, T.K. Nutritional status of schol going children between the age group of 6–12 yrs in rural area of Bijpaur district. Natl. J. Community Med. 2016, 7, 409–412. [Google Scholar] [CrossRef]
- Sherpa, A.T.; Singh, N.; Basnet, P.B.; Sherpa, M.C. Nutritional Status Assessment of Adolescent School Going Children in Solukhumbu, Nepal. Nepal. Med. J. 2019, 2, 155–159. [Google Scholar] [CrossRef]
- Bhattacharyya, M.; Roy, S.; Sarkar, A.; Sinha, R.N.; Mallick, A.K.; Bandyopadhyay, S. Burden of malnutrition among school-going children in a slum area of Kolkata: A matter of concern. J. Family Med. Prim. Care 2017, 10, 2940–2946. [Google Scholar]
- Tiwar, D.; Tiwari, M.; Kumari, R.; Agrawal, A.; Dubey, G.P. Learning disabilities among school going children with Protein Energy Malnutrition in relation to psychosomatic constitution. Int. J. Adv. Res. 2015, 3, 1211–1218. [Google Scholar] [CrossRef]
- Marwat, Z.I.; Nawaz, S.; Wazir, A.K.; Afzal, E.; Gul, C.; Khan, M.J.; Ahmad, A. Nutritional assessment of school going children in district Abbottabad, K.P. Pakistan. Int. J. Sci. Rep. 2019, 5, 59–65. [Google Scholar] [CrossRef]
- Aboagye, R.G.; Kugbey, N.; Ahinkorah, B.O.; Seidu, A.-A.; Cadri, A.; Bosoka, S.A.; Akonor, P.Y.; Takase, M. Nutritional status of school children in the South Tongu District, Ghana. PLoS ONE 2022, 17, e0269718. [Google Scholar] [CrossRef] [PubMed]
- Erismann, S.; Knoblauch, A.M.; Diagbouga, S.; Odermatt, P.; Gerold, J.; Shrestha, A.; Tarnagda, G.; Savadogo, B.; Schindler, C.; Utzinger, J.; et al. Prevalence and risk factors of undernutrition among schoolchildren in the Plateau Central and Centre-Ouest regions of Burkina Faso. Infect. Dis. Poverty 2017, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Wahed, W.Y.A.; Hassan, S.K.; Eldessouki, R. Malnutrition and Its Associated Factors among Rural School Children in Fayoum Governorate, Egypt. J. Environ. Public Health 2017, 2017, 4783791. [Google Scholar] [CrossRef] [PubMed]
- Tani, I.A.; Hassan, N.; Poly, I.; A New Approach for Solving Nutritional Deficiency of Primary School Going Children from Comparative Analysis of Slum and Urban Children of Bangladesh. ResearchgateNet 2018. Available online: https://www.researchgate.net/profile/Nazia_Hassan9/publication/322926519_A_New_Approach_for_Solving_Nutritional_Deficiency_of_Primary_School_Going_Children_from_Comparative_Analysis_of_Slum_and_Urban_Children_of_Bangladesh/links/5a772cf0a6fdccbb3c098061/A (accessed on 31 December 2023).
- Farhin, S.; Jaffry, T.; Zafar, S.; Rashid, F. Frequency and assessment of Nutritional Status of school going children in rural areas of Islamabad. Pak. J. Med. Sci. 2021, 37, 1475–1479. [Google Scholar] [CrossRef] [PubMed]
- Abraham, S.; Chauhan, R.; Rajesh, M.; Purty, A.; Singh, Z. Nutritional status and various morbidities among school children of a coastal area in South India. Int. J. Res. Med. Sci. 2015, 3, 718–722. [Google Scholar] [CrossRef]
- Kundu, S.; Khan, S.I.; Bakchi, J.; Sayeed, A.; Al Banna, H.; Begum, M.R.; Hassan, N. Sources of nutrition information and nutritional knowledge among school-going adolescents in Bangladesh. Public Health Pract. 2020, 1, 100030. [Google Scholar] [CrossRef] [PubMed]
- Joshi, H.; Gupta, R.; Joshi, M.; Vipul, M. Determinants of Nutritional Status of School Children Determinants of Nutritional Status of School Children—A Cross Sectional Study in the Western Region of Nepal. Njirm 2011, 2, 2230–9969. [Google Scholar]
- Manyanga, T.; El-Sayed, H.; Doku, D.T.; Randall, J. The prevalence of underweight, overweight, obesity and associated risk factors among school-going adolescents in seven African countries. BMC Public Health 2014, 14, 887. [Google Scholar] [CrossRef]
- Anwaar, S.; Manzoor, M.S.; Nadeem, S.; Saleem, A.; Saeed, M.A.; Mustafa, F.; Raza, A. Assessment of nutritional status among school-going children through their dietary intake. Asian J. Allied Health Sci. 2022, 7, 1–12. [Google Scholar]
- Tukei, J.; Masinde Muliro University of Science and Technology; Situma, J.; Konyole, S. Relationship between household characteristics and food security among households with school going children 6-14 years in Turkana county, Kenya. Afr. J. Food Agric. Nutr. Dev. 2022, 22, 20246–20258. [Google Scholar] [CrossRef]
- Eluya, M. Dietary Intake and Nutritional Status of Primary School Children Participating in the Botswana School Feeding Programme, South-East District, Botswana. Ph.D. Thesis, University of Kwazulu-Natal, Durban, South Africa, 2019. [Google Scholar]
- Owusu, J.S.; Colecraft, E.K.; Aryeetey, R.N.; Vaccaro, J.A.; Huffman, F.G. Nutrition Intakes and Nutritional Status of School Age Children in Ghana. J. Food Res. 2017, 6, 11. [Google Scholar] [CrossRef]
- Danquah, A.O.; Amoah, A.N.; Steiner-Asiedu, M.; Opare-Obisaw, C. Nutritional Status of Participating and Non-participating Pupils in the Ghana School Feeding Programme. J. Food Res. 2012, 1, 263. [Google Scholar] [CrossRef]
- Mwaniki, E.W.; Makokha, A.N.; Muttunga, J.N. Nutrition status and associated morbidity risk factors among orphanage and non-orphanage children in selected public primary schools within dagoretti, nairobi, kenya. East Afr. Med. J. 2014, 91, 289–297. [Google Scholar]
- Rawat, R.; Garg, S.K.; Chopra, H.; Bajpai, S.K.; Bano, T.; Jain, S.; Kumar, A. Prevalence of malnutrition among school children with reference to overweight and obesity and its associated factors. Indian J. Community Health 2012, 24, 97–102. [Google Scholar]
- Gha, H.F.; Isa, Z.M.; Aljunid, S.; Tami, A.M.; Abdalqa, M.A. Nutritional Status, Nutritional Habit and Breakfast Intake in Relation to IQ among Primary School Children in Baghdad City, Iraq. Pak. J. Nutr. 2012, 11, 379–382. [Google Scholar] [CrossRef][Green Version]
- Gebremariam, H.; Seid, O.; Assefa, H. Assessment of Nutritional Status and Associated Factors among School Going Adolescents of Mekelle City, Northern Ethiopia. Int. J. Nutr. Food Sci. 2015, 4, 118. [Google Scholar] [CrossRef]
- Fiorentino, M.; Bastard, G.; Sembène, M.; Fortin, S.; Traissac, P.; Landais, E.; Icard-Vernière, C.; Wieringa, F.T.; Berger, J. Anthropometric and Micronutrient Status of School-Children in an Urban West Africa Setting: A Cross-Sectional Study in Dakar (Senegal). PLoS ONE 2013, 8, e84328. [Google Scholar] [CrossRef] [PubMed]
- Freda, D.I.; Ogyiri, L.; Asante, M.; Mensah, A.A.; Steele-Dadzie1, R.K.; Boateng, L. Nutritional Status of Boarding and Non-Boarding Children in Selected Schools in the Accra Metropolis. J. Biol. Agric. Healthc. 2013, 3, 156–163. [Google Scholar]
- Eze, J.; Oguonu, T.; Ojinnaka, N.; Ibe, B. Physical growth and nutritional status assessment of school children in Enugu, Nigeria. Niger. J. Clin. Pract. 2017, 20, 64–70. [Google Scholar] [CrossRef]
- Kaushik, B.; Bisai, S.; Chakraborty, J.; Datta, N.; Banerjee, P. Extreme levels of underweight and stunting among pre-adolescent children of low socioeconomic class from Madhyamgram and Barasat, West Bengal, India. Coll. Antropol. 2008, 32, 73–77. [Google Scholar]
- Patel, N.; Gunjana, G.; Patel, S.; Thanvi, R.; Sathvara, P.; Joshi, R. Nutrition and health status of school children in urban area of Ahmedabad, India: Comparison with Indian Council of Medical Research and body mass index standards. J. Nat. Sci. Biol. Med. 2015, 6, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Ullah, W.; Khan, S.J. Nutrtional Status and its Correlation with Academic Performance of School Going Children. Pak. J. Med. Health Sci. 2022, 16, 784–787. [Google Scholar] [CrossRef]
- Naik, S.; Itagi, S.; Patil, M. Relationship between nutritional status and academic performance of Lambani school children. Int. J. Appl. Home Sci. 2015, 6, 3235–3238. [Google Scholar]
- Agarwal, A.; Jain, S.; Garg, S.; Chopra, H.; Bano, T. Prevalence of malnutrition and its impact on scholastic performance among 8–12 year children from 2 private schools of urban Meerut. J. Med. Allied Sci. 2018, 8, 3–6. [Google Scholar] [CrossRef]
- Aiga, H.; Abe, K.; Randriamampionona, E.; Razafinombana, A.R. Possible causalities between malnutrition and academic performances among primary schoolchildren: A cross-sectional study in rural Madagascar. BMJ Nutr. Prev. Health 2021, 4, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Aiga, H.; Abe, K.; Andrianome, V.N.; Randriamampionona, E.; Razafinombana, A.R.; Murai, T.; Hara, M. Risk factors for malnutrition among school-aged children: A cross-sectional study in rural Madagascar. BMC Public Health 2019, 19, 773. [Google Scholar] [CrossRef] [PubMed]
- Akeredolu, I.A.; Oguntona, B.E.; Okafor, C.; Osisanya, O.J. Iron, Zinc, and Copper Malnutrition among Primary School Children in Lagos, Niagara. Food Nutr. Sci. 2011, 2, 1063–1070. [Google Scholar] [CrossRef]
- Kumar Ahirwar, A.; Ahirwar, A.K.; Gautam, R.K.; Ahirwar, A.K. Nutritional status among school going boys and girls (5–17 years) of Bharia Tribe (PVTG) of Patalkot-District Chhindwara (M. P.) India Nutritional status among school going boys and girls (5-17 years) of Bharia Tribe (PVTG) of Patalkot-District Chhindwara. Hum. Biol. Rev. 2017, 6, 346. [Google Scholar]
- Mansur, D.; Sharma, K.; Kumar Mehta, D.; Shakya, R.; Islam Mansur, D. A Study on Nutritional Status of Rural School going Children in Kavre District Prevalence of Underweight, Stunting and Thinness Among Adolescent Girls in Kavre District View project A Study on Nutritional Status of Rural School going Children in Kavre Dis. Child. Kavre Dist. Kathmandu Univ. Med. J. 2015, 50, 146–151. [Google Scholar]
- Lardner, D.; Giordano, J.; Jung, M.; Passafaro, M.D.; Small, A.; Haar, M.; Beria, J. Evaluation of nutritional status among school-aged children in rural Kwahu-eastern region, Ghana; anthropometric measures and environmental influences. Afr. J. Food, Agric. Nutr. Dev. 2015, 15, 9996–10012. [Google Scholar] [CrossRef]
- Jubayer, A.; Islam, H.; Nayan, M.; Khan, N.I. Prevalence and Factors Associated with Nutritional Status and Individual Level Double Burden of Malnutrition among School Going Adolescents of Bangladesh: Findings from Global School-based Student Health Survey-2014. Int. J. Sci. Res. Biol. Sci. 2020, 7, 51057. [Google Scholar]
- Weres, Z.G.; Yebyo, H.G.; Gesesew, H.A.; Miruts, K.B.; Woldehymanot, T.E. Assessment of Adolescents’ Under Nutrition Level among School Students in Eastern Tigray, Ethiopia: A Cross-Sectional Study. J. Nutr. Food Sci. 2015, 5, 1000402. [Google Scholar] [CrossRef]
- Falade, O.S.; Otemuyiwa, I.; Oluwasola, O.; Oladipo, W.; Adewusi, S.A. School Feeding Programme in Nigeria: The Nutritional Status of Pupils in a Public Primary School in Ile-Ife, Osun State, Nigeria. Food Nutr. Sci. 2012, 3, 596–605. [Google Scholar] [CrossRef][Green Version]
- Manjunath, R.; Jagadish Kumar, K.; Kulkarni, P.; Begum, K.; Gangadhar, M.R. Malnutrition among under-five children of Kadukuruba tribe: Need to reach the unreached. J. Clin. Diagn. Res. 2014, 8, JC01–JC04. [Google Scholar] [CrossRef]
- Khan, D.S.A.; Das, J.K.; Zareen, S.; Lassi, Z.S.; Salman, A.; Raashid, M.; Dero, A.A.; Khanzada, A.; Bhutta, Z.A. Nutritional Status and Dietary Intake of School-Age Children and Early Adolescents: Systematic Review in a Developing Country and Lessons for the Global Perspective. Front. Nutr. 2022, 8, 739447. [Google Scholar] [CrossRef] [PubMed]
- Veereshwar Rao, K.; Pandi, M.; Das, K.; Mukherjee, K. Assessment of the Nutritional Status among the School-going Children aged 6-8 Years from Port Blair, South Andaman, India: A Cross-sectional Study. Antrocom Online J. Anthropol. 2021, 17, 177–184. [Google Scholar]
- Kwabla, M.P.; Gyan, C.; Zotor, F. Nutritional status of in-school children and its associated factors in Denkyembour District, eastern region, Ghana: Comparing schools with feeding and non-school feeding policies. Nutr. J. 2018, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Katoch, O.R.; Sharma, A.; Nawaz, A.; Shrikant. Nutritional assessment using composite index of anthropometric failure (CIAF) among school-going children in J&K, India. J. Tianjin Univ. Sci. Technol. 2021, 3, 6. [Google Scholar] [CrossRef]
- ShahidI, S.; Mohyuddin, A. Malnutrition among school going children in Varanasi. Food Sci. Res. J. 2015, 4, 1654–1659. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Item | Search Strategy |
|---|---|
| #1 Search to identify malnutrition | Malnutrition [Meshi Term] OR Undernutrition OR Overnutrition OR Undernourishment OR Overnourishment OR Nutritional Deficiency OR Nutrient Deficiency OR Protein-Energy Malnutrition OR PEM OR Micronutrient Deficiency OR Vitamin Deficiency OR Mineral Deficiency OR Macronutrient Deficiency OR Energy Deficiency OR Caloric Deficiency OR Dietary Insufficiency OR Inadequate Nutrition OR Poor Nutrition OR Inadequate Intake OR Inadequate Diet OR Dietary Deficiency OR Food Insufficiency OR Food Scarcity OR Food Shortage OR Starvation OR Hunger OR Famine OR Wasting OR Stunting OR Underweight OR Overweight OR Obesity OR Body Mass Index OR BMI OR Kwashiorkor OR Marasmus OR Growth Failure OR Growth Stunting OR Growth Retardation OR Iodine Deficiency OR Iron Deficiency OR Vitamin A Deficiency OR Zinc Deficiency OR Calcium Deficiency OR Anemia |
| #2 Search to identify risk factors | Risk factors [MeSH Term] OR Determinants OR Causes OR Contributors OR Influences OR Precursors OR Triggers OR Antecedents OR Exposures OR Vulnerabilities OR Predictors OR Indicators OR Correlates |
| #3 Search to identify health outcomes | Health Outcomes [MeSH Term] OR Health Status OR Health Conditions OR Health Results OR Health Effects OR Health Impact OR Health Consequences OR Health Indicators OR Immune System Diseases OR Immune System Abnormalities OR Immune System Disorders OR Immune System Diseases OR Growth Disorders OR Growth Retardation OR Growth Impairment OR Growth Failure OR Anemia OR Iron-Deficiency Anemia OR Iron Deficiency Anemias OR Osteoporosis OR Bone Diseases, Metabolic OR Bone Demineralization, Pathologic OR Bone Loss OR Night Blindness OR Vision Disorders OR Cardiovascular Diseases OR Heart Diseases OR Hypertension OR Mental Disorders OR Mental Health OR Depression OR Anxiety Disorders OR Cognitive Dysfunction OR Mortality OR Mortality Risk |
| #4 Search to identify school outcomes | Education Outcomes [MeSH Term] OR School Outcomes [MeSH Term] OR Drop-out OR Truancy OR Skipping class OR Violence OR Poor academic performance OR Inattentiveness OR Educational Failure OR Academic Failure OR School Disengagement OR School Problems OR Poor school performance OR Poor educational attainment |
| #5 Search to identify in-school children | School Children [MeSH Term] OR Child OR Childhood OR Infants OR Toddlers OR Adolescents OR Adolescence OR Junior High School Students OR Senior High School Students OR Elementary School Students OR Preschoolers OR Preteens OR Pre-adolescents OR Middle School Students OR High School Students OR Primary School Students OR Nursery School Children OR Kindergarteners OR Grade School Children OR Teenagers OR Teenage Years OR Puberty OR Pre-schoolers OR Early Childhood OR Middle Childhood OR Late Childhood OR Youth |
| #6 Search to identify developing countries | Developing countries [MeSH Term] Africa OR Asia OR south America OR Afghanistan OR Albania OR Algeria OR Angola OR Antigua and Barbuda OR Argentina OR Armenia OR Azerbaijan OR Bahamas OR Bahrain OR Bangladesh OR Barbados OR Belarus OR Belize OR Benin OR Bhutan OR Bolivia OR Bosnia and Herzegovina OR Botswana OR Brazil OR Brunei OR Bulgaria OR Burkina Faso OR Burundi OR Cambodia OR Cameroon OR Cape Verde OR Central African Republic OR Chad OR Chile OR China OR Colombia OR Comoros OR Congo OR Costa Rica OR Côte d’Ivoire OR Croatia OR Cuba OR Cyprus OR Czech Republic OR Djibouti OR Dominica OR Dominican Republic OR Ecuador OR Egypt OR El Salvador OR Equatorial Guinea OR Eritrea OR Eswatini OR Ethiopia OR Fiji OR Gabon OR Gambia OR Georgia OR Ghana OR Grenada OR Guatemala OR Guinea OR Guinea-Bissau OR Guyana OR Haiti OR Honduras OR Hungary OR India OR Indonesia OR Iran OR Iraq OR Jamaica OR Jordan OR Kazakhstan OR Kenya OR Kiribati OR Kosovo OR Kuwait OR Kyrgyzstan OR Laos OR Latvia OR Lebanon OR Lesotho OR Liberia OR Libya OR Lithuania OR Macedonia OR Madagascar OR Malawi OR Malaysia OR Maldives OR Mali OR Malta OR Marshall Islands OR Mauritania OR Mauritius OR Mexico OR Micronesia OR Moldova OR Mongolia OR Montenegro OR Morocco OR Mozambique OR Myanmar OR Namibia OR Nauru OR Nepal OR Nicaragua OR Niger OR Nigeria OR Oman OR Pakistan OR Palau OR Palestine OR Panama OR Papua New Guinea OR Paraguay OR Peru OR Philippines OR Poland OR Portugal OR Qatar OR Romania OR Russia OR Rwanda OR Saint Kitts and Nevis OR Saint Lucia OR Saint Vincent and the Grenadines OR Samoa OR Sao Tome and Principe OR Saudi Arabia OR Senegal OR Serbia OR Seychelles OR Sierra Leone OR Solomon Islands OR Somalia OR South Africa OR South Sudan OR Sri Lanka OR Sudan OR Suriname OR Syria OR Tajikistan OR Tanzania OR Thailand OR Timor-Leste OR Togo OR Tonga OR Trinidad and Tobago OR Tunisia OR Turkey OR Turkmenistan OR Tuvalu OR Uganda OR Ukraine OR United Arab Emirates OR Uruguay OR Uzbekistan OR Vanuatu OR Venezuela OR Vietnam OR Yemen OR Zambia OR Zimbabwe |
| Overall search strategy | #2 AND #1 AND #5 AND #6 Not animal * #3 AND #1 AND 5 AND #6 Not animal * #4 AND #1 AND 5 AND #6 Not animal * |
| Filters activated | Language: English language Date: From 1 January 2000 |
| Inclusion criteria | The paper should be:
|
| Exclusion criteria | The paper should be:
|
| Main Theme | Subtheme | Authors |
|---|---|---|
| Socio-demographics | Low total family income | [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,41,42,43,44,52,75] |
| Higher socio-economic status | [28] | |
| Large family size | [16,21,24,30,32,33,36,37,38,39,41,45,46,47] | |
| Nuclear family | [44] | |
| Depend on agricultural land | [16] | |
| Irregular work of father | [56] | |
| Unemployed father | [46] | |
| Maternal employment | [39] | |
| Those who have lost their mother | [46] | |
| The age at which the child starts complementary foods | [16] | |
| Children whose parents were laborers | [20] | |
| Being younger | [17,41,47] | |
| Older age group | [55,56] | |
| Adolescent who come from male-headed household | [17] | |
| Low educational status of parents | [17,21,23,26,29,32,33,34,36,37,43,44,45,46,48,49,50,51,52,53] | |
| Formal education | [54] | |
| Type of school attended | [42] | |
| Being female | [39,48] | |
| Being male | [38,47] | |
| Malaise | Those who suffered diarrhea | [68] |
| Those who suffered cold/coughs | [68] | |
| Anorexia | [52] | |
| Nature of environment | Children who live in flood areas | [18] |
| Poor environment | [26] | |
| Living slum | [36,57] | |
| Rural environment | [28] | |
| Urban environment | [28,44,58] | |
| Living in small houses | [39] | |
| Sanitation | Unsafe drinking water | [16,54] |
| Children with poor personal hygiene | [59] | |
| Knowledge of practice | Source of information | [60] |
| Low information on nutritional panel | [20,23,24,60,61] | |
| Poor breastfeeding practices | [16] | |
| Dietary Habit | Adolescent who consume regular carbonated soft drinks | [13,62] |
| Poor eating habits | [36] | |
| Adolescents who consume regular fast food | [13,62] | |
| Households without food security | [13,37,48,50,62] | |
| Inadequate dietary intake of adolescent | [17,27,31,42,47,52,63,65,67,68] | |
| Adolescents who consumed diet of low diversity | [17,25,68] | |
| Adolescents who consume foods such as plus, legumes, and lentils | [71] | |
| Children with low consumption of high-quality protein | [20,30,41,56,63,64,65,66] | |
| Poor dietary quality | [67] | |
| Children who have the habit of eating in between meals | [69] | |
| Children who are having dinner as the heaviest meal of the day | [69] | |
| Children who consume more than three meals in a day | [69] | |
| Micronutrient deficiency | [73] | |
| Skipping breakfast | [30,56,70] | |
| Children who consumed beverages between meals per day | [54] | |
| Early cessation of breast feeding | [52] | |
| Nutrient Deficiency | Vitamin A | [41,65,66,72] |
| Calcium deficiency | [65,66] | |
| Zinc deficiency | [66,72] | |
| Iodine deficiency | [72] | |
| Iron deficiency | [66,72] | |
| Micro-nutrient deficiency | [52] | |
| Maternal malnutrition | [52] | |
| Body Weight | Obesity | [74] |
| Overweight | [74] | |
| Means of transport | Children who use vehicular transport to school | [69] |
| Household activities | Depending on family members | [60] |
| Not participating in household activities | [69] | |
| Children who watch TV more than 3 hours per day | [69] | |
| Sedentary lifestyle | Children who have the habit of not playing outdoor games | [69] |
| Adolescents who do not do any physical activities | [69] |
| Main Theme | Subtheme | Authors |
|---|---|---|
| General health status | Malaria | [20] |
| Headaches | [20] | |
| Nose bleeding | [20] | |
| Abdominal pains | [20,76] | |
| Fainting | [20] | |
| Pallor | [59] | |
| Myopia | [59] | |
| Diarrhea | [68] | |
| Colds/coughs | [68] | |
| Vomiting | [68] | |
| Fever | [68] | |
| Fetal/Maternal health | Poor maternal health | [13] |
| Preterm birth | [13] | |
| Risk of Small for Gestational Age (SGA) | [13] | |
| Morbidity | Increased morbidity in children | [67] |
| Social issue | Gender discrimination | [16] |
| Eye (Ophthalmologic) Complications | Conjunctival xerosis | [35] |
| Bitot’s spot | [35] | |
| Dental caries | [59,63,76] | |
| Physiological and developmental delays | [28] | |
| Cognitive function | Reduced cognitive functions | [28,50,52,64,70,72,74] |
| Metabolic Risk factors | Obesity | [21,64,74] |
| Overweight | [21,74] | |
| Risk of nutrition-related chronic diseases | [33] | |
| Immunity/Infection | Lowered resistance to infection | [52,61] |
| Recurring illness | [13] | |
| Upper Respiratory Infections (URI) | [20,76] | |
| Lower Respiratory Tract infection | [76] | |
| Skin infection | [20,68] | |
| Risk of developing non-communicable diseases | [21,69] | |
| Parasitic infections | [40,76] | |
| Impaired immune function | [28] | |
| Nutritional deficiency | Vitamin A deficiency | [18,19,22,35,40] |
| Vitamin B complex deficiency | [18] | |
| Iron deficiency | [18,22,40,66,73] | |
| Calcium deficiency | [63] | |
| Inadequate dietary intake | [40] | |
| Growth Retardation | Faltering growth | [61,64] |
| Long-term relative physical growth retardation | [28] |
| Main Theme | Subtheme | Authors |
|---|---|---|
| School Performance | Diminished learning ability | [18,61] |
| Work efficiency | [18] | |
| Poor academic performance | [27,32,42,52,53,67,70,77,78,79] | |
| Lack of concentration | [32] | |
| Poor memory | [52] | |
| Attendance | High levels of school dropout | [20,32,42,74] |
| Low-class attendance | [32,42,64,72,74,80] | |
| Delayed school entry | [27,32,42] | |
| Decreased graduation rates from primary and secondary school | [27] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amoadu, M.; Abraham, S.A.; Adams, A.K.; Akoto-Buabeng, W.; Obeng, P.; Hagan, J.E., Jr. Risk Factors of Malnutrition among In-School Children and Adolescents in Developing Countries: A Scoping Review. Children 2024, 11, 476. https://doi.org/10.3390/children11040476
Amoadu M, Abraham SA, Adams AK, Akoto-Buabeng W, Obeng P, Hagan JE Jr. Risk Factors of Malnutrition among In-School Children and Adolescents in Developing Countries: A Scoping Review. Children. 2024; 11(4):476. https://doi.org/10.3390/children11040476
Chicago/Turabian StyleAmoadu, Mustapha, Susanna Aba Abraham, Abdul Karim Adams, William Akoto-Buabeng, Paul Obeng, and John Elvis Hagan, Jr. 2024. "Risk Factors of Malnutrition among In-School Children and Adolescents in Developing Countries: A Scoping Review" Children 11, no. 4: 476. https://doi.org/10.3390/children11040476
APA StyleAmoadu, M., Abraham, S. A., Adams, A. K., Akoto-Buabeng, W., Obeng, P., & Hagan, J. E., Jr. (2024). Risk Factors of Malnutrition among In-School Children and Adolescents in Developing Countries: A Scoping Review. Children, 11(4), 476. https://doi.org/10.3390/children11040476