
Artificial Intelligence in Pediatric Liver Transplantation: Opportunities and Challenges of a New Era



Abstract
1. Introduction
2. Definitions of Artificial Intelligence, Machine Learning, and Deep Learning
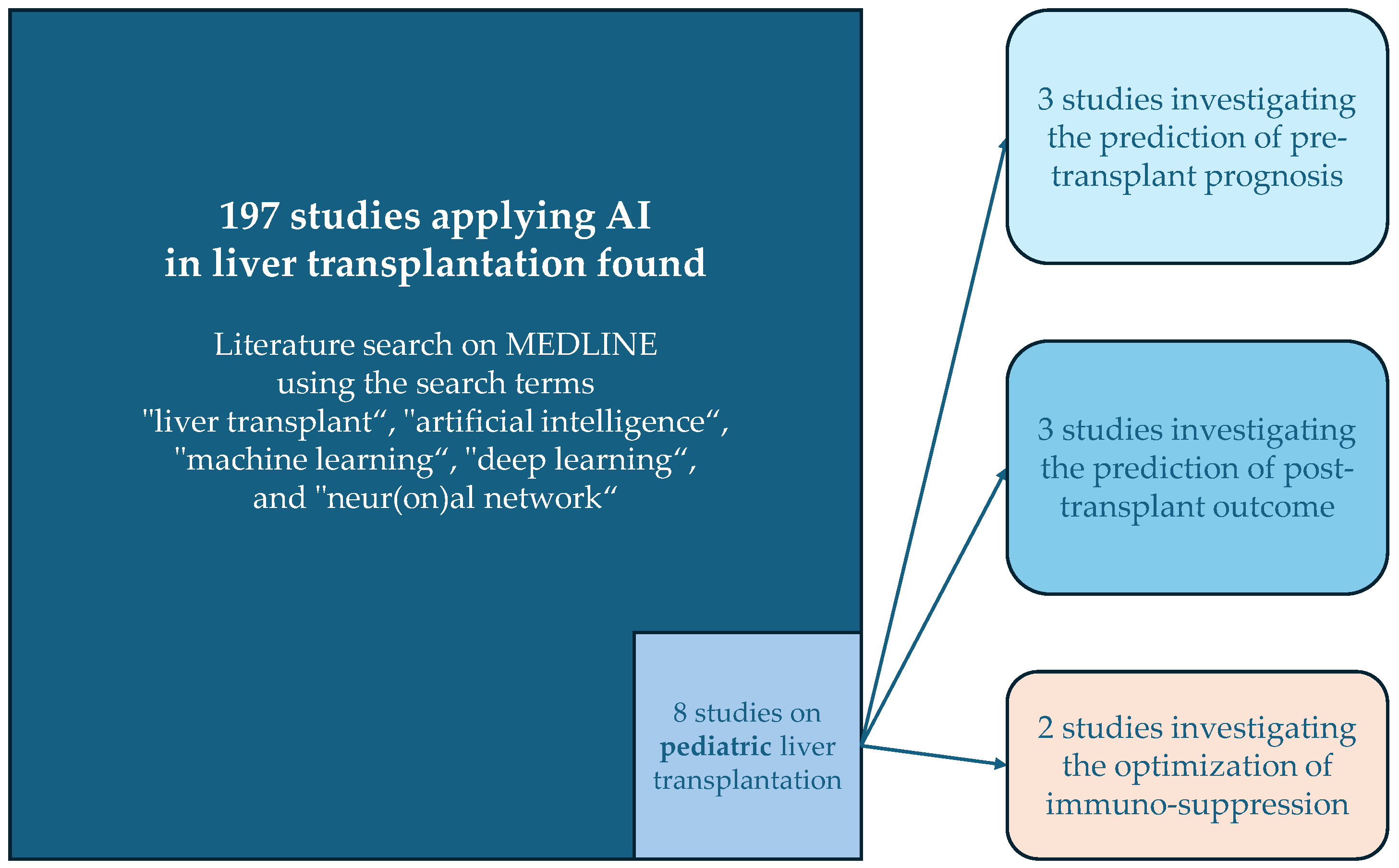
3. AI in Pediatric Liver Transplantation: Overview of the Existing Literature
3.1. Studies Investigating Pre-Transplant Predictors of Outcome
3.2. Studies Investigating Post-Transplant Predictors of Outcome
3.3. Studies on Postoperative Immunosuppressive Therapy
4. Summary of Current AI Applications in Pediatric Liver Transplantation: Research and Clinical Practice
4.1. Pre-Transplant Prediction
4.2. Post-Transplant Outcome Prediction
4.3. Personalized Immunosuppressive Therapy
5. Future Directions and Potential Applications of AI in Pediatric Liver Transplantation
5.1. Improving Donor-Recipient Matching and Organ Allocation
5.2. Managing Long-Term Complications
5.3. Enhanced Data Integration
6. Limitations and Critical Aspects of AI in Pediatric Liver Transplantation
6.1. Trust and Interpretability
6.2. Bias and Data Quality
6.3. Ethical Considerations and Patient Safety
6.4. Clinical Implementation
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Starzl, T.E.; Groth, C.G.; Brettschneider, L.; Penn, I.; Fulginiti, V.A.; Moon, J.B.; Blanchard, H.; Martin, A.J.; Porter, K.A. Orthotopic homotransplantation of the human liver. Ann. Surg. 1968, 168, 392–415. [Google Scholar] [CrossRef] [PubMed]
- Bismuth, H.; Houssin, D. Reduced-sized orthotopic liver graft in hepatic transplantation in children. Surgery 1984, 95, 367–370. [Google Scholar] [PubMed]
- Pichlmayr, R.; Ringe, B.; Gubernatis, G.; Hauss, J.; Bunzendahl, H. Transplantation of a donor liver to 2 recipients (splitting transplantation)—A new method in the further development of segmental liver transplantation. Langenbecks Arch. Chir. 1988, 373, 127–130. [Google Scholar] [CrossRef]
- Strong, R.W.; Lynch, S.V.; Ong, T.H.; Matsunami, H.; Koido, Y.; Balderson, G.A. Successful liver transplantation from a living donor to her son. N. Engl. J. Med. 1990, 322, 1505–1507. [Google Scholar] [CrossRef]
- Sammons, H.; Starkey, E. Ethical issues of clinical trials in children. Paediatr. Child Health 2016, 26, 95–98. [Google Scholar] [CrossRef]
- Khorsandi, S.E.; Hardgrave, H.J.; Osborn, T.; Klutts, G.; Nigh, J.; Spencer-Cole, R.T.; Kakos, C.D.; Anastasiou, I.; Mavros, M.N.; Giorgakis, E. Artificial Intelligence in Liver Transplantation. Transplant. Proc. 2021, 53, 2939–2944. [Google Scholar] [CrossRef] [PubMed]
- Vodovotz, Y.; Barclay, D.; Yin, J.; Squires, R.H.; Zamora, R. Dynamics of Systemic Inflammation as a Function of Developmental Stage in Pediatric Acute Liver Failure. Front. Immunol. 2020, 11, 610861. [Google Scholar] [CrossRef]
- Kulkarni, S.; Chi, L.; Goss, C.; Lian, Q.; Nadler, M.; Stoll, J.; Doyle, M.; Turmelle, Y.; Khan, A. Random forest analysis identifies change in serum creatinine and listing status as the most predictive variables of an outcome for young children on liver transplant waitlist. Pediatr. Transplant. 2021, 25, e13932. [Google Scholar] [CrossRef] [PubMed]
- Wadhwani, S.I.; Hsu, E.K.; Shaffer, M.L.; Anand, R.; Ng, V.L.; Bucuvalas, J.C. Predicting ideal outcome after pediatric liver transplantation: An exploratory study using machine learning analyses to leverage Studies of Pediatric Liver Transplantation Data. Pediatr. Transplant. 2019, 23, e13554. [Google Scholar] [CrossRef]
- Killian, M.O.; Payrovnaziri, S.N.; Gupta, D.; Desai, D.; He, Z. Machine learning-based prediction of health outcomes in pediatric organ transplantation recipients. JAMIA Open 2021, 4, ooab008. [Google Scholar] [CrossRef]
- Ningappa, M.; Rahman, S.A.; Higgs, B.W.; Ashokkumar, C.S.; Sahni, N.; Sindhi, R.; Das, J. A network-based approach to identify expression modules underlying rejection in pediatric liver transplantation. Cell Rep. Med. 2022, 3, 100605. [Google Scholar] [CrossRef]
- Jung, S.; Park, K.; Ihn, K.; Kim, S.J.; Kim, M.S.; Chae, D.; Koo, B.-N. Predicting graft failure in pediatric liver transplantation based on early biomarkers using machine learning models. Sci. Rep. 2022, 12, 22411. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Liu, F.; Gao, H.; Yan, M.; Zhang, F.; Zhao, J.; Qin, Y.; Li, Y.; Zhang, Y. Compare the performance of multiple machine learning models in predicting tacrolimus concentration for infant patients with living donor liver transplantation. Pediatr. Transplant. 2023, 27, e14379. [Google Scholar] [CrossRef]
- Tan, S.-B.; Kumar, K.S.; Truong, A.T.L.; Tan, L.W.J.; Chong, L.M.; Gan, T.R.X.; Mali, V.P.; Aw, M.M.; Blasiak, A.; Ho, D. Comparing the Performance of Multiple Small-Data Personalized Tacrolimus Dosing Models for Pediatric Liver Transplant: A Retrospective Study. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; pp. 1–4. [Google Scholar]
- Goyet, J.d.V.d.; Baumann, U.; Karam, V.; Verkade, H.J. Letter to the editor: Organ shortage and pediatric liver transplantation: David against Goliath. Hepatology 2022, 75, 1342–1343. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.K.; Lemoine, C.P.; Superina, R.; Sayed, B.; Goldaracena, N.; Soltys, K.A.; Griesemer, A.; Dick, A.; Angelis, M.; Chin, L.T.; et al. State of pediatric liver transplantation in the United States and achieving zero wait list mortality with ideal outcomes: A statement from the Starzl Network for Excellence in Pediatric Transplant Surgeon’s Working Group. Pediatr. Transplant. 2023, 27 (Suppl. S1), e14283. [Google Scholar] [CrossRef] [PubMed]
- Hsu, E.K.; Mazariegos, G.V. Global lessons in graft type and pediatric liver allocation: A path toward improving outcomes and eliminating wait-list mortality. Liver Transplant. 2017, 23, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Ahn, D.J.; Zeng, S.B.; Pelzer, K.M.; Barth, R.N.; Gallo, A.; Parker, W.F. The accuracy of nonstandardized meld/peld score exceptions in the pediatric liver allocation system. Transplantation 2023, 107, e247–e256. [Google Scholar] [CrossRef] [PubMed]
- James, L.P.; Alonso, E.M.; Hynan, L.S.; Hinson, J.A.; Davern, T.J.; Lee, W.M.; Squires, R.H.; the Pediatric acute liver failure study group. detection of acetaminophen protein adducts in children with acute liver failure of indeterminate cause. Pediatrics 2006, 118, e676–e681. [Google Scholar] [CrossRef] [PubMed]
- McDiarmid, S.V.; Anand, R.; Lindblad, A.S. Development of a pediatric end-stage liver disease score to predict poor outcome in children awaiting liver transplantation. Transplantation 2002, 74, 173–181. [Google Scholar] [CrossRef]
- Goyet, J.d.V.d. Tailoring allocation policies and improving access to pediatric liver transplantation in Italy: Outframing and concluding. J. Hepatol. 2024. [Google Scholar] [CrossRef]
- Miloh, T.; Barton, A.; Wheeler, J.; Pham, Y.; Hewitt, W.; Keegan, T.; Sanchez, C.; Bulut, P.; Goss, J. Immunosuppression in pediatric liver transplant recipients: Unique aspects. Liver Transplant. 2017, 23, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Blondet, N.M.; Healey, P.J.; Hsu, E. Immunosuppression in the pediatric transplant recipient. Semin. Pediatr. Surg. 2017, 26, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Ayllón, M.D.; Ciria, R.; Cruz-Ramírez, M.; Pérez-Ortiz, M.; Gómez, I.; Valente, R.; O’Grady, J.; de la Mata, M.; Hervás-Martínez, C.; Heaton, N.D.; et al. Validation of artificial neural networks as a methodology for donor-recipient matching for liver transplantation. Liver Transplant. 2018, 24, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Cesaretti, M.; Brustia, R.; Goumard, C.; Cauchy, F.; Poté, N.; Dondero, F.; Paugam-Burtz, C.; Durand, F.; Paradis, V.; Diaspro, A.; et al. Use of artificial intelligence as an innovative method for liver graft macrosteatosis assessment. Liver Transplant. 2020, 26, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Bhat, M.; Rabindranath, M.; Chara, B.S.; Simonetto, D.A. Artificial intelligence, machine learning, and deep learning in liver transplantation. J. Hepatol. 2023, 78, 1216–1233. [Google Scholar] [CrossRef]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Machry, M.; Ferreira, L.F.; Lucchese, A.M.; Kalil, A.N.; Feier, F.H. Liver volumetric and anatomic assessment in living donor liver transplantation: The role of modern imaging and artificial intelligence. World J. Transplant. 2023, 13, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, A.; Langs, G.; Denk, H.; Zatloukal, K.; Müller, H. Causability and explainability of artificial intelligence in medicine. WIREs Data Min. Knowl. Discov. 2019, 9, 1312. [Google Scholar] [CrossRef] [PubMed]
- Ratti, E.; Graves, M. Explainable machine learning practices: Opening another black box for reliable medical AI. AI Ethics 2022, 2, 801–814. [Google Scholar] [CrossRef]
- Hee, K. Is data quality enough for a clinical decision?: Apply machine learning and avoid bias. In Proceedings of the 2017 IEEE International Conference on Big Data (Big Data), Boston, MA, USA, 11–14 December 2017; IEEE: New York, NY, USA, 2017. [Google Scholar]
- Gianfrancesco, M.A.; Tamang, S.; Yazdany, J.; Schmajuk, G. Potential biases in machine learning algorithms using electronic health record data. JAMA Intern. Med. 2018, 178, 1544–1547. [Google Scholar] [CrossRef]
- Azencott, C.-A. Machine learning and genomics: Precision medicine versus patient privacy. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2018, 376, 20170350. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, H.H.; Tran, N.K.; Betts, E.V.; Howell, L.P.; Green, R. Artificial intelligence and machine learning in pathology: The present landscape of supervised methods. Acad. Pathol. 2019, 6, 2374289519873088. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, M.J.; Javed, Z.; Sadia, H.; Qureshi, I.A.; Irshad, A.; Ahmed, R.; Malik, K.; Raza, S.; Abbas, A.; Pezzani, R.; et al. Clinical applications of artificial intelligence and machine learning in cancer diagnosis: Looking into the future. Cancer Cell Int. 2021, 21, 270. [Google Scholar] [CrossRef]
- Keane, P.A.; Topol, E.J. AI-facilitated health care requires education of clinicians. Lancet 2021, 397, 1254. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Authors | Title | Type of Study and Topic | AI Methods | Results/Conclusion | Area |
|---|---|---|---|---|---|
| Vodovotz et al., 2020 [7] | Dynamics of Systemic Inflammation as a Function of Developmental Stage in Pediatric Acute Liver Failure | Retrospective multi-center study. Prognostic clinical characteristics and PALF-associated systemic inflammatory mediators in daily serum samples on the outcome of children with acute liver failure. | Dynamic Bayesian network inference, dynamic network analysis | HMGB1 was the sole central node in both INF and NS, aiding in the prediction of pre-transplant prognosis. | Prediction of pre-transplant prognosis |
| Kulkarni et al., 2021 [8] | Random forest analysis identifies change in serum creatinine and listing status as the most predictive variables of an outcome for young children on liver transplant waitlist | Registry retrospective analysis. Demographic, clinical, listing history, and laboratory variables at the time of listing (baseline variables) and changes in variables between listing and prior to outcome (trajectory variables) were analyzed to predict the outcome of children listed for LT. | Random forest analysis | Change in creatinine, listing status, need for RRT, time spent on the LT waitlist, and type of diagnosis were the most predictive variables. | Prediction of pre-transplant prognosis |
| Wadhwani et al., 2019 [9] | Predicting ideal outcome after pediatric liver transplantation: An exploratory study using machine learning analyses to leverage Studies of Pediatric Liver Transplantation Data | Registry analysis. Prognostic value of baseline demographic factors and clinical/biochemical factors in the first year post-transplant for prediction of the ideal outcome at 3 years after pLT. | Random forest analyses using ensembles of conditional inference trees | Factors associated with an ideal outcome: white race, shorter duration of operation, absence of vascular and biliary complications within 30 days, absence of pretransplant supplemental feedings, and use of Roux limb biliary anastomosis. | Prediction of post-transplant outcome |
| Killian et al., 2021 [10] | Machine learning-based prediction of health outcomes in pediatric organ transplantation recipients | Predict 1-, 3-, and 5-year post-transplant hospitalizations using patient and administrative data from a large pediatric organ transplant center. | Naive Bayes, support vector ML, and DL | DL models did not yield superior performance compared to models using ML methods. | Prediction of post-transplant outcome |
| Ningappa et al., 2022 [11] | A network-based approach to identify expression modules underlying rejection in pediatric liver transplantation | Cohort study. Identification and validation of separate pre- and post-LT transcriptomic signatures of rejection. | Integrative ML approach, combining transcriptomics data with the reference high-quality human protein interactome to identify network module signatures | ML identified high-risk patients for rejection after pLT and also found targets for individualized antirejection treatment. | Prediction of post-transplant outcome |
| Jung et al., 2022 [12] | Predicting graft failure in pediatric liver transplantation based on early biomarkers using machine learning models | Retrospective single-center cohort study. Identification of predictors of graft failure by ML-based methods. | Least absolute shrinkage and selection operator (LASSO)-based method | The most predictive features were preoperative hepatic encephalopathy, Natrium level at the end of surgery, hepatic artery thrombosis, and POD7 total bilirubin. | Prediction of post-transplant outcome |
| Song et al., 2022 [13] | Compare the performance of multiple machine learning models in predicting tacrolimus concentration for infant patients with living donor liver transplantation | Retrospective single-center cohort study. Factors influencing tacrolimus concentration in pLT patients. | Thirteen ML algorithms were applied for the development of prediction models. APE, the ratio of APE ≤ 3 ng/mL, and the ideal rate were used to evaluate the predictive performance of the model. | The Ridge regression model (GRWR, donors’ and recipients’ CYP3A5 genotypes, urea, hemoglobin, albumin, and BMI) yielded good predictive performance and provided potential clinical application. | Optimization of immunosuppression |
| Tan et al., 2022 [14] | Comparing the Performance of Multiple Small-Data Personalized Tacrolimus Dosing Models for Pediatric Liver Transplant: A Retrospective Study | Retrospective single-center study. A small-data, artificial intelligence-derived platform, single-center study using AI to model the dose-response relationship of tacrolimus and identify suitable doses dynamically. | CURATE.AI, a small-data AI-driven platform, uses data from individual patients obtained once daily. | This study established and compared the predictive performance of 6 personalized tacrolimus dosing models for pediatric liver transplant patients and identified a suitable model with consistently good predictive performance based on data from pediatric liver transplant patients. | Optimization of immunosuppression |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuchs, J.; Rabaux-Eygasier, L.; Guerin, F. Artificial Intelligence in Pediatric Liver Transplantation: Opportunities and Challenges of a New Era. Children 2024, 11, 996. https://doi.org/10.3390/children11080996
Fuchs J, Rabaux-Eygasier L, Guerin F. Artificial Intelligence in Pediatric Liver Transplantation: Opportunities and Challenges of a New Era. Children. 2024; 11(8):996. https://doi.org/10.3390/children11080996
Chicago/Turabian StyleFuchs, Juri, Lucas Rabaux-Eygasier, and Florent Guerin. 2024. "Artificial Intelligence in Pediatric Liver Transplantation: Opportunities and Challenges of a New Era" Children 11, no. 8: 996. https://doi.org/10.3390/children11080996
APA StyleFuchs, J., Rabaux-Eygasier, L., & Guerin, F. (2024). Artificial Intelligence in Pediatric Liver Transplantation: Opportunities and Challenges of a New Era. Children, 11(8), 996. https://doi.org/10.3390/children11080996