1. Introduction
The Center for Disease Control and Prevention (CDC) reports that cardiovascular disease (CVD) is the leading cause of death in the United States. Although the physical manifestation of this disease is less prevalent in adolescents, research shows that the development of CVD starts from childhood [
1,
2]. It is well known that the development of cardiovascular disease is multifactorial, and obesity, a sedentary lifestyle, and low cardiorespiratory fitness (CRF) are important risk factors for the development of CVD. In fact, risk factors such as obesity and physical inactivity in early life correlate with anatomical changes in the coronary arteries and aorta through the increase in atherosclerotic-related hypertension [
3]. Research shows that overweight and obese children with high percentages of fat mass (FM%) and a body mass index (BMI) above the 85
th percentile also report higher arterial stiffness and blood pressure compared to their lean peers, placing them at a higher risk of developing hypertension and CVD later in life [
4,
5]. Specifically, excess adipose tissue has been associated with systemic inflammation [
6], which influences the progression of atherosclerosis leading to CVD [
7]. Yet, regular exercise can increase CRF and delay obesity-related comorbidities by modulating the inflammatory processes at all ages. In fact, CRF in children is negatively associated with low-grade inflammatory markers, which is positively associated with body fat [
8].
Non-invasive assessments of aortic blood pressure have shown to predict cardiovascular events better than brachial assessments [
9]. Carotid-to-femoral pulse wave velocity (cfPWV) is considered the gold standard for the assessment of central arterial stiffness in children [
10], and it is a valid biomarker for the diagnoses and risk stratification of CVD [
11]. Another key CVD risk factor in children is low CRF. Although measurements of maximal aerobic capacity (expressed as peak oxygen consumption (VO
2peak)) are considered the best indicator of CRF in pediatric populations, submaximal measurements of aerobic efficiency such as the oxygen consumption at the aerobic threshold (AerT) are considered an adequate biomarker of fitness in youth [
12]. Submaximal indicators of CRF are commonly used in children since young individuals may lack motivation to exercise at severe intensities and/or fail to deliver maximal effort [
12]. Research shows that values of oxygen consumption at AerT lower than 11 ml/kg/min are associated with an increased risk of death in the clinical population [
13]. Moreover, CRF is inversely associated with arterial stiffness, independently of fat mass [
14], and high levels of CRF have been shown to decrease the incidence of all-cause cardiovascular disease [
15]. Furthermore, it has been suggested that sufficiently high CRF may attenuate the deleterious cardiovascular effects of obesity in adults, providing a stepping stone for the “fit but fat” paradigm [
16]. However, evidence in support of such a paradigm, or observations made in children and adolescents, is inconsistent, in part due to limited access to obese yet healthy adolescents.
Therefore, this study aimed to investigate the association between non-invasive, gold-standard indicators of CRF and the body fat percentage with cfPWV and the central arterial pressure in healthy adolescents.
3. Results
Participants’ descriptive characteristics are reported in
Table 1. The Kolmogorov–Smirnov test for normality conducted on cfPWV data from 60 participants did not reject the null hypothesis of normality (
p = 0.09), suggesting that the data were consistent with a normal distribution. The sample for this study was comprised of individuals representing a diverse range of ethnicities including white (
n = 35, 58.3%), Indian (
n = 12, 20.0%), Asian (
n = 9, 15.0%), and Black (
n =4, 6.7%). Eighteen subjects were considered overweight or obese (8 overweight and 10 obese) as per US Centers for Disease Control and Prevention BMI-for-age growth charts (58.5 ± 30.9 BMI percentile). Males in this sample had a higher height (
p < 0.01, F = 13.7), body mass (
p < 0.01, F = 8.3), FFM% (
p < 0.01, F = 21.2), ASBP (
p = 0.01, F = 7.1), and VO
2peak (
p = 0.03, F = 4.8) than the females. Females had a higher HR at AerT (HR
AerT) (
p < 0.01, F = 11.1) and HR at AnT (HR
AnT) (
p < 0.01, F = 7.3) compared to males. Differences in cardiovascular measures between VO
2AerT, VO
2peak, BMI, and BF% tertiles are reported in
Table 2,
Table 3,
Table 4 and
Table 5 and in
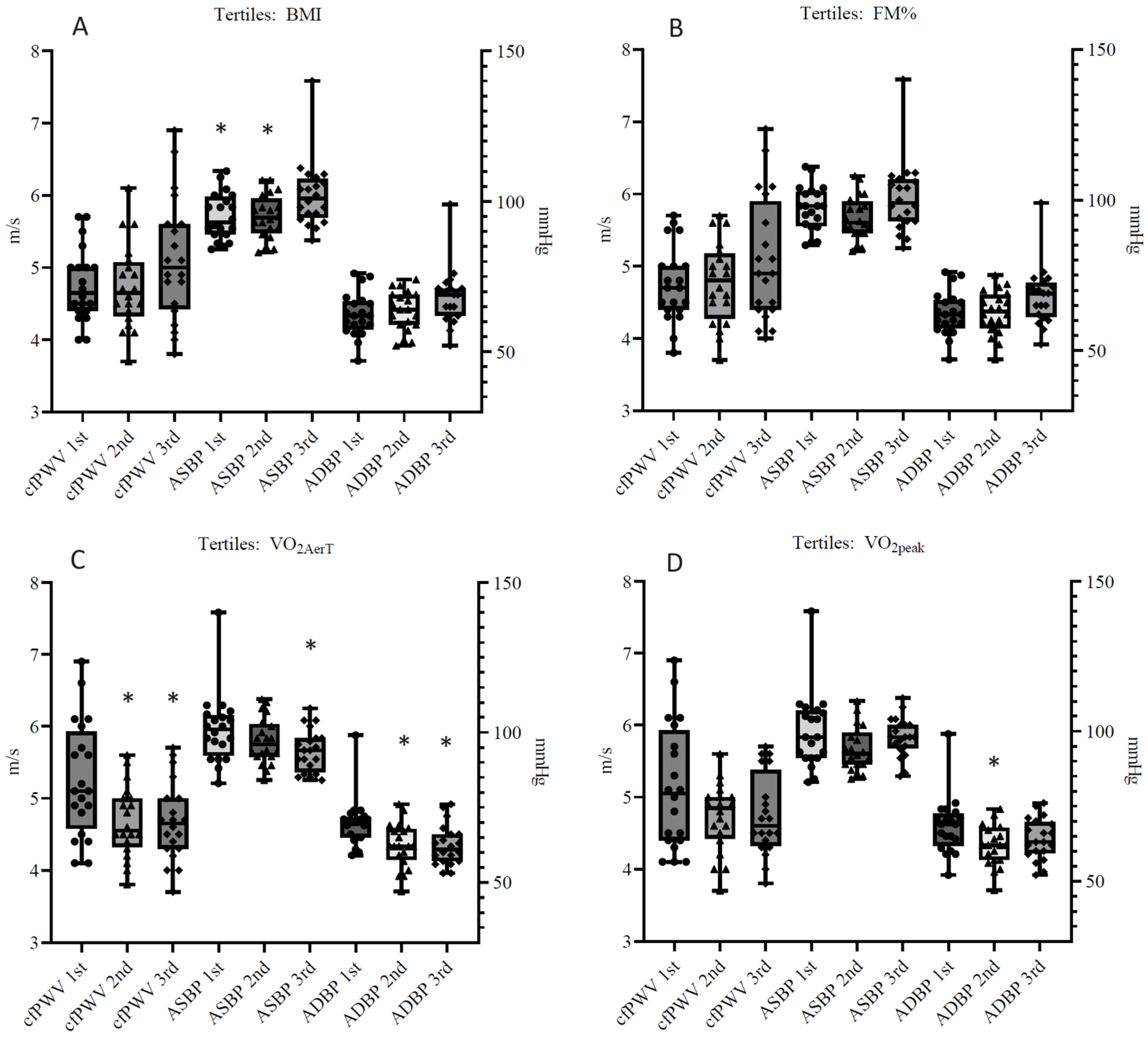
Figure 1, respectively.
ASBP was higher in the third BMI tertile compared to the first two (
p = 0.02, F = 4.4), and no differences were found between BMI and FM% tertiles in any cardiovascular measure. The second and third VO
2AerT tertiles had lower cfPWV (
p < 0.01, F = 5.6) and ADBP (
p < 0.01, F = 6.5) compared to the first tertile. The third VO
2AerT tertile had lower ASBP (
p = 0.05, F = 3.1) compared to the first tertile. The second VO
2peak tertile had lower ADBP (
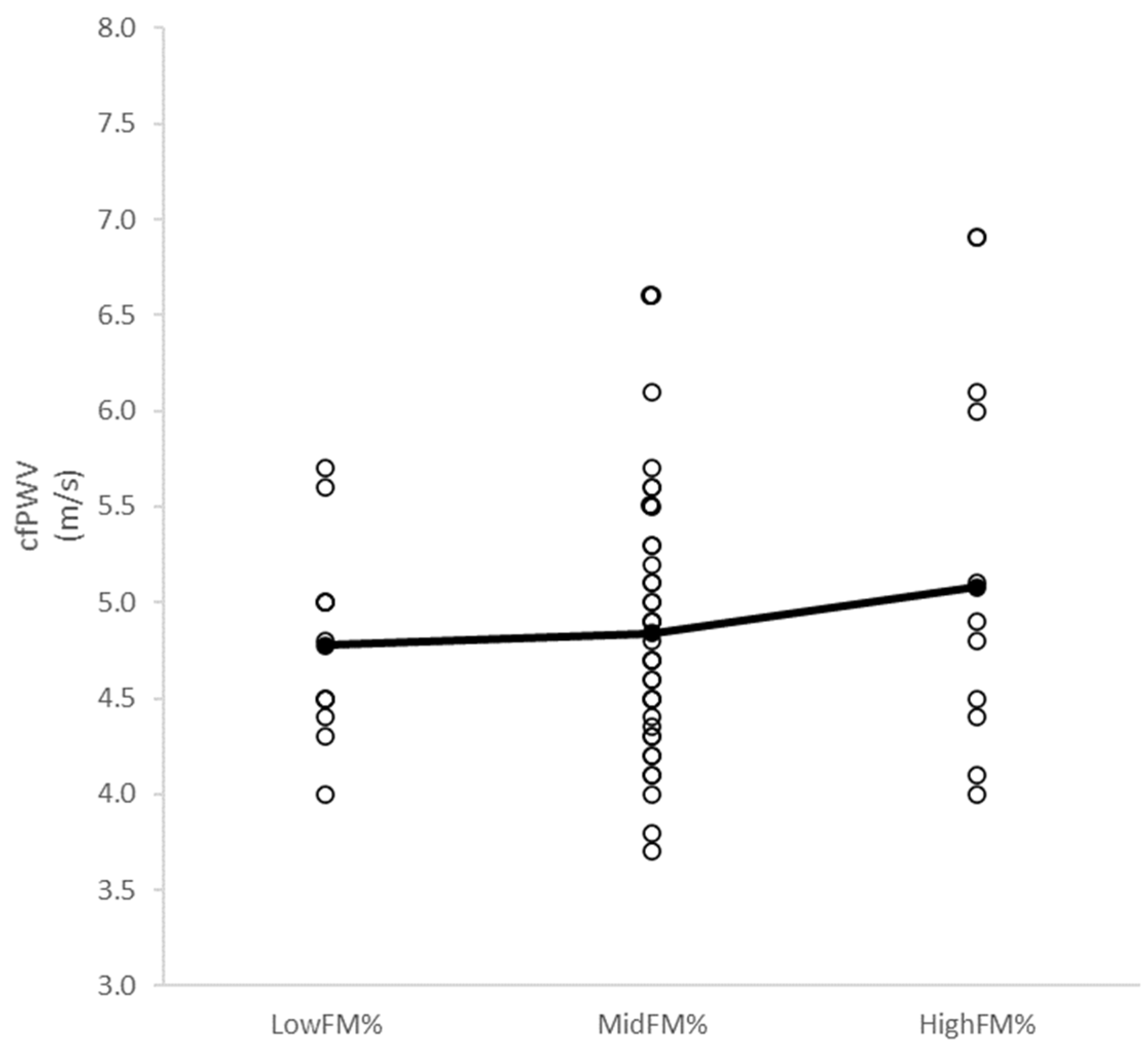
p = 0.03, F = 3.6) compared to the first tertile. No differences in cfPWV (
p = 0.53, F = 0.6) were observed between LowFM%, MidFM%, and HighFM% (4.8 ± 0.5 m/s, 4.8 ± 0.6 m/s, and 5.1 ± 1.0 m/s, respectively) (
Figure 2).
Results of the multivariable analysis are reported in
Table 6. The analysis showed that the eight-variable model significantly contributed to the variance of cfPWV (F(8, 51) = 7.450,
p < 0.01), accounting for 47% of the variance. Individually, two out of the eight variables significantly predicted cfPWV. Participants more likely had a higher cfPWV with a higher ADBP (adjusted
B = 0.389, t = 2.321,
p < 0.01) and if they were older (adjusted
B = 0.420, t = 3.053,
p < 0.05). VO
2AerT, VO
2peak, BMI, and BF% were not independently associated with cfPWV.
4. Discussion
In our cohort of adolescents, we observed that age and ADBP were the best predictors of higher arterial stiffness independently of sex and that children with higher levels of CRF had lower cfPWV and reduced central blood pressure. Interestingly, our findings indicated that elevated FM% did not uniformly correspond to increased cfPWV, and there was a tendency toward an association between BMI and cfPWV, with the correlation approaching statistical significance. This suggests that CRF might serve as a more robust indicator of cardiovascular health in healthy adolescents compared to BMI and FM%. Also, our data suggest that VO2AerT could be a better indicator of cardiovascular health compared to VO2peak in apparently healthy, recreationally active adolescents. Therefore, we postulate that VO2AerT, an index of aerobic efficiency, may play an important role in the association between overweight and cardiovascular health in adolescents.
Previous research has shown the association between high CRF and lower central arterial stiffness and systolic blood pressure in children [
14,
23], and that overweight and obese children tend to display high levels of arterial stiffness and elevated blood pressure [
24]. These findings align with our results, which indicate that adolescents with higher CRF have lower cfPWV and aortic blood pressure. In contrast, adolescents with a high BMI exhibit elevated ASBP, but not cfPWV, compared to their leaner peers. Surprisingly, aortic blood pressure and cfPWV did not differ among adolescents with varying FM%. Although obesity is an independent predictor of cardiovascular risk, the direct association between excess adiposity and arterial stiffness has previously been debated, especially in healthy children and adolescents [
25]. Previous studies have shown that obese children often suffer from elevated blood pressure and hypertension, which may alter arterial functions and increase arterial stiffness [
26]. Although increased adiposity is linked to attenuated adiponectin signaling [
27] and increased inflammatory cytokines concerning endothelial dysfunction and arterial stiffness in children [
28,
29], this process does not always manifest phenotypically, especially in adolescents with high levels of CRF. In fact, overweight and obese adolescents can show low arterial stiffness due to the cardioprotective effect of exercise, since CRF is inversely and independently associated with arterial stiffness [
14,
30]. Research conducted in adult populations shows CRF may be a stronger modulator of cardiovascular risk than body composition [
31], yet the benefits of high fitness levels may be compromised by obesity. Although this finding is promising, obese children may respond to higher fitness levels differently than adults. Recently, a systematic review confirmed the inverse association between CRF and central PWV. Also, there were inconsistencies between adolescents and adults since a positive association between fitness and central PWV in adolescents was only observed in the adolescents [
32]. Additionally, a study conducted on 252 male children and adolescents reported that body weight determines central systolic blood pressure, a surrogate for arterial stiffness, rather than CRF [
33]. The divergent findings could be caused by the method used to determine CRF (estimations vs. direct measurements) and/or too wide an age range, including children in different developmental stages, and/or the inclusion of participants with a relatively low body weight and high level of CRF. Therefore, it is essential to include participants with a wide range of body weights and CRFs, and to use direct assessment of CRF in the evaluation of cardiovascular risk factors in healthy, young individuals [
34]. VO
2peak is considered the gold standard for CRF. However, it may not be the best way to assess the aerobic capacity in children as psychological and physiological factors can limit the achievement of VO
2peak in this population. Research shows that a lack of motivation to reach the maximal effort [
12,
35] and an undeveloped anaerobic metabolism [
36] may increase the margin of error while assessing VO
2peak, thus calling into question its utility in children and adolescents for preventing the achievement of maximal effort. Moreover, the achievement of VO
2peak and VO
2AerT have shown to be independent in children and do not occur at the same rate. While VO
2peak mainly relies on both a maximal cardiac output and oxygen extraction, VO
2AerT depends on the muscle oxidative capacity [
12] and the ability to produce and remove lactate, which is impaired in young children [
37,
38]. This indicates that VO
2AerT may be more appropriate than VO
2peak for assessing CRF, and it can be identified even if individuals prematurely end the graded exercise test. When considering strategies to improve CRF, research shows that moderate exercise intensities can provide enough of a stimulus to improve both indices of fitness and health [
39]. However, voluntary physical activity may lack the duration and intensity associated with adequate stimuli for chronic aerobic exercise adaptations in children [
40]. In contrast, research conducted by our laboratory shows that when play-based physical activity is supervised, improvements in CRF and cardiovascular health in overweight children can occur, independently of changes in body weight and body composition [
41].
Another important finding of this study is that cardiovascular measures showed a decreasing trend across both VO
2peak and VO
2AerT tertiles. However, mean differences were significant only in VO
2AerT tertiles. This result suggests that VO
2peak may not be the best indicator of CRF in adolescents, as young individuals may reach volitional exhaustion before the maximal oxygen consumption is attained [
42]. On the contrary, submaximal indicators of CRF such as VO
2AerT may be preferred, as they have been shown to be effective indicators of cardiovascular health [
11]. This result is highly relevant in the pediatric field as the prognosis of cardiovascular disease in adolescents can be acquired using submaximal indicators of CRF. Moreover, it is possible to increase VO
2AerT in children with just a moderate exercise intensity [
43], while a vigorous exercise intensity is necessary to improve VO
2max [
44]. It may be more important to consider clinical relevance between tertiles even if mean differences are not statistically significant. For example, children and adolescents are considered hypertensive when their blood pressure readings are ≥95
th percentile for sex, age, and height with 4 mmHg difference between the 90
th and 95
th percentiles in both systolic and diastolic blood pressure [
45]. Although not statistically significant, the first and second tertiles of BMI and FM% showed a mean difference in aortic pressures equal or greater than 4 mmHg against the third tertile. Similarly, the second and third tertiles of VO
2peak and VO
2AerT, when not statistically different, showed similar mean differences in aortic blood pressure when compared to the first tertile. These results are relevant as they suggest that adolescent children with VO
2AerT and VO
2peak above 14.5 ml/kg/min and 30 ml/kg/min, and BMI and FM% below 23kg/m
2 and 30%, respectively, may be at a lower risk of developing high blood pressure and consequently arterial stiffness.
This research study included participants from different ethnic backgrounds, with the ethnic distribution closely mirroring the demographic composition of North Carolina and of the general United States population (≈60% white, 6–20% Indian, Asian, and African American). Although the percentage distributions of the sample did not perfectly match those of this state and country, it is important to consider how the sample’s diversity supports the generalizability of the results. We recognize the limitations of our methods, including the heterogeneous sample of males and females, the limited number of overweight/obese participants, and the potential selection bias. Although our sample had an equal number of male and female participants, the two sexes were not equally distributed between tertiles and we recognize that sex differences were not analyzed in this study. Moreover, only one-third of our sample (18 out of 60 participants) was overweight/obese. A larger representation of overweight and especially obese individuals may help in investigating differences in cardiovascular measures in individuals with high BMI and FM%. Finally, this study’s potential selection bias, due to the exclusion of participants with certain medical conditions, may have skewed the results by not fully representing the diverse range of health profiles, thereby limiting the generalizability and applicability of the findings. Our findings are limited to cross-sectional data and do not provide further evidence of the mechanisms by which CRF may attenuate the deleterious cardiovascular effects of overweight or excess adiposity beyond the healthy normative values in adolescents. Future studies should address these limitations by recruiting more overweight and obese individuals and monitoring CRF before and after specific physical exercise programs in this population. Specifically, investigating the effect of different types of physical activity on CRF and their impact on CV health may help us to further understand the dose–response relationship between aerobic fitness and arterial health in overweight adolescents.


 ,
, 

{kind=link}
{kind=link}