Pediatric Solid Tumors in Resource-Constrained Settings: A Review of Available Evidence on Management, Outcomes, and Barriers to Care


 and
and 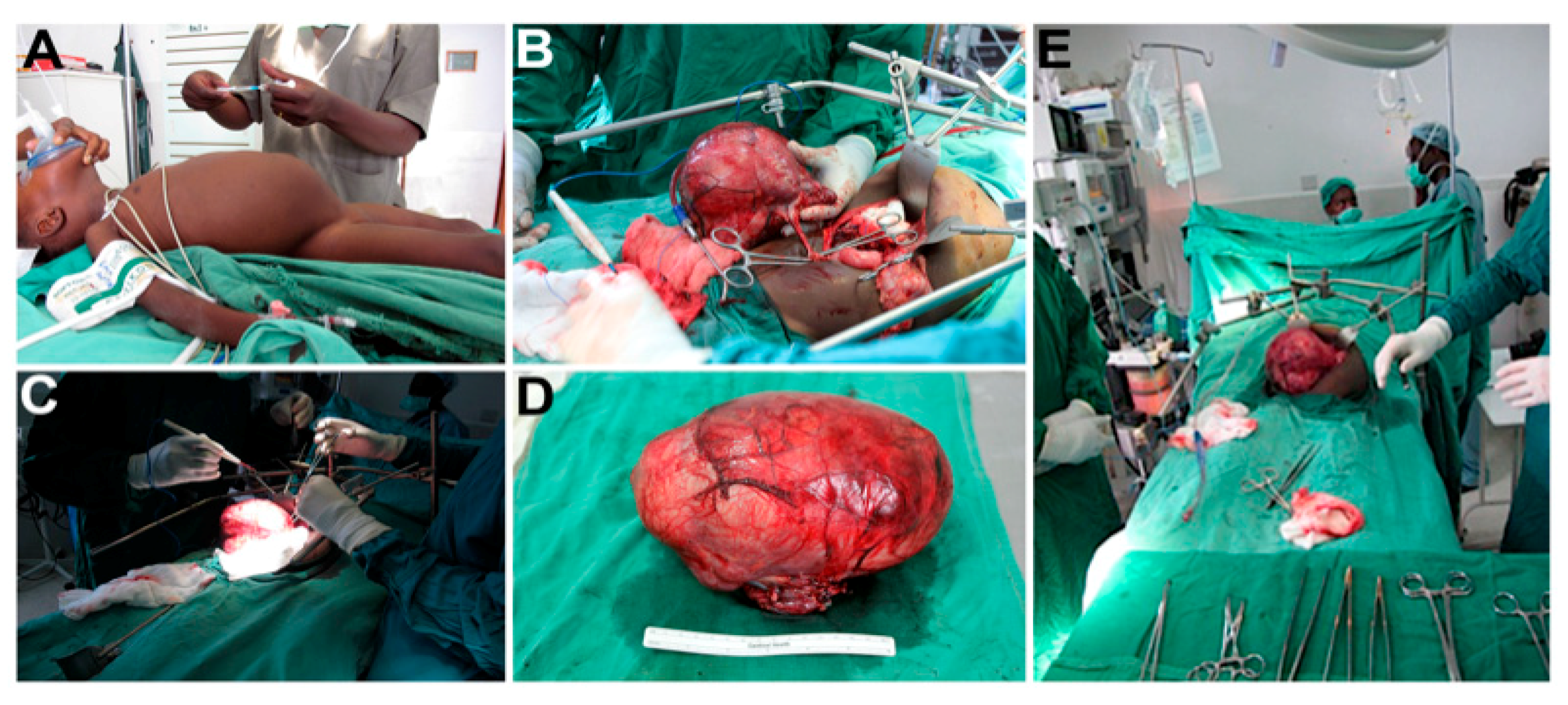{kind=link}
Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
3. Results
3.1. Nephroblastoma (Wilms Tumor)
3.1.1. Burden of Disease and Current Outcomes
3.1.2. Biology
3.1.3. Barriers to Care
3.1.4. Management
3.2. Other Solid Tumors of Childhood
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Appendix A. Images of Pediatric Surgical Oncology Care Performed in Kijabe, Kenya

References
- Spreafico, F.; Pritchard-Jones, K.; Bergeron, C.; de Kraker, J.; Dallorso, S.; Graf, N. Value and difficulties of a common European strategy for recurrent Wilms’ tumor. Expert Rev. Anticancer Ther. 2009, 9, 693–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tournade, M.F.; Com-Nougue, C.; de Kraker, J.; Ludwig, R.; Rey, A.; Burgers, J.M.; Sandstedt, B.; Godzinski, J.; Carli, M.; Potter, R.; et al. Optimal duration of preoperative therapy in unilateral and nonmetastatic Wilms’ tumor in children older than 6 months: Results of the Ninth International Society of Pediatric Oncology Wilms’ Tumor Trial and Study. J. Clin. Oncol. 2001, 19, 488–500. [Google Scholar] [CrossRef] [PubMed]
- de Kraker, J.; Graf, N.; van Tinteren, H.; Pein, F.; Sandstedt, B.; Godzinski, J.; Tournade, M.F. Reduction of postoperative chemotherapy in children with stage I intermediate-risk and anaplastic Wilms’ tumour (SIOP 93-01 trial): A randomised controlled trial. Lancet 2004, 364, 1229–1235. [Google Scholar] [CrossRef]
- Joko-Fru, W.Y.; Parkin, D.M.; Borok, M.; Chokunonga, E.; Korir, A.; Nambooze, S.; Wabinga, H.; Liu, B.; Stefan, C. Survival from Childhood Cancers in Eastern Africa: A Population-based registry study. Int. J. Cancer 2018. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.S.; Challinor, J.M.; Howard, S.C.; Israels, T. Improving Care for Children with Cancer in Low- and Middle-Income Countries—A SIOP PODC Initiative. Pediatr. Blood Cancer 2016, 63, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, F.K.; Macharia, W.M. Clinical presentation and treatment outcome in children with nephroblastoma in Kenya. East Afr. Med. J. 2001, 78, S43–S47. [Google Scholar] [PubMed]
- Axt, J.; Abdallah, F.; Axt, M.; Githanga, J.; Hansen, E.; Lessan, J.; Li, M.; Musimbi, J.; Mwachiro, M.; Newton, M.; et al. Wilms tumor survival in Kenya. J. Pediatr. Surg. 2013, 48, 1254–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Israels, T.; Borgstein, E.; Pidini, D.; Chagaluka, G.; de Kraker, J.; Kamiza, S.; Molyneux, E.M. Management of children with a Wilms tumor in Malawi, sub-Saharan Africa. J. Pediatr. Hematol. Oncol. 2012, 34, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Abuidris, D.O.; Elimam, M.E.; Nugud, F.M.; Elgaili, E.M.; Ahmed, M.E.; Arora, R.S. Wilms tumour in Sudan. Pediatr. Blood Cancer 2008, 50, 1135–1137. [Google Scholar] [CrossRef] [PubMed]
- Axt, J.; Murphy, A.J.; Seeley, E.H.; Martin, C.A.; Taylor, C.; Pierce, J.; Caprioli, R.M.; Whiteside, M.; Lovvorn, H.N., 3rd. Race disparities in Wilms tumor incidence and biology. J. Surg. Res. 2011, 170, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Libes, J.M.; Seeley, E.H.; Li, M.; Axt, J.R.; Pierce, J.; Correa, H.; Newton, M.; Hansen, E.; Judd, A.; McDonald, H.; et al. Race disparities in peptide profiles of North American and Kenyan Wilms tumor specimens. J. Am. Coll. Surg. 2014, 218, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.J.; Axt, J.R.; de Caestecker, C.; Pierce, J.; Correa, H.; Seeley, E.H.; Caprioli, R.M.; Newton, M.W.; de Caestecker, M.P.; Lovvorn, H.N., 3rd. Molecular characterization of Wilms’ tumor from a resource-constrained region of sub-Saharan Africa. Int. J. Cancer 2012, 131, E983–E994. [Google Scholar] [CrossRef] [PubMed]
- Lovvorn, H.N., 3rd; Pierce, J.; Libes, J.; Li, B.; Wei, Q.; Correa, H.; Gouffon, J.; Clark, P.E.; Axt, J.R.; Hansen, E.; et al. Genetic and chromosomal alterations in Kenyan Wilms Tumor. Genes Chromosomes Cancer 2015, 54, 702–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelps, H.M.; Al-Jadiry, M.F.; Corbitt, N.M.; Pierce, J.M.; Li, B.; Wei, Q.; Flores, R.R.; Correa, H.; Uccini, S.; Frangoul, H.; et al. Molecular and epidemiologic characterization of Wilms tumor from Baghdad, Iraq. World J. Pediatr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Nyagetuba, J.K.M.; Hansen, E.N. Pediatric solid tumors in Africa: Different biology? Curr. Opin. Pediatr. 2017, 29, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Meara, J.G.; Leather, A.J.; Hagander, L.; Alkire, B.C.; Alonso, N.; Ameh, E.A.; Bickler, S.W.; Conteh, L.; Dare, A.J.; Davies, J.; et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet 2015, 386, 569–624. [Google Scholar] [CrossRef]
- Aronson, D.C.; Maharaj, A.; Sheik-Gafoor, M.H.; Hadley, G.P. The results of treatment of children with metastatic Wilms tumours (WT) in an African setting: Do liver metastases have a negative impact on survival? Pediatr. Blood Cancer 2012, 59, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Rogers, T.; Bowley, D.M.; Poole, J.; Swanepoel, P.; Wainwright, J.; Beale, P.; Pitcher, G. Experience and outcomes of nephroblastoma in Johannesburg, 1998–2003. Eur. J. Pediatr. Surg. 2007, 17, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Israels, T.; Moreira, C.; Scanlan, T.; Molyneux, L.; Kampondeni, S.; Hesseling, P.; Heij, H.; Borgstein, E.; Vujanic, G.; Pritchard-Jones, K.; et al. SIOP PODC: Clinical guidelines for the management of children with Wilms tumour in a low income setting. Pediatr. Blood Cancer 2013, 60, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Paintsil, V.; David, H.; Kambugu, J.; Renner, L.; Kouya, F.; Eden, T.; Hesseling, P.; Molyneux, E.; Israels, T. The Collaborative Wilms Tumour Africa Project; baseline evaluation of Wilms tumour treatment and outcome in eight institutes in sub-Saharan Africa. Eur. J. Cancer 2015, 51, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, P.; Lam, C.G.; Kaur, G.; Itriago, E.; Ribeiro, R.C.; Arora, R.S. Determinants of Treatment Abandonment in Childhood Cancer: Results from a Global Survey. PLoS ONE 2016, 11, e0163090. [Google Scholar] [CrossRef] [PubMed]
- Libes, J.; Oruko, O.; Abdallah, F.; Githanga, J.; Ndung’u, J.; Musimbi, J.; Njuguna, F.; Patel, K.; White, J.; Axt, J.R.; et al. Risk factors for abandonment of Wilms tumor therapy in Kenya. Pediatr. Blood Cancer 2015, 62, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Hadley, G.P.; Govender, D.; Landers, G. Wilms tumour with unfavourable histology: Implications for clinicians in the Third World. Med. Pediatr. Oncol. 2001, 36, 652–653. [Google Scholar] [CrossRef] [PubMed]
- Mostert, S.; Lam, C.G.; Njuguna, F.; Patenaude, A.F.; Kulkarni, K.; Salaverria, C. Hospital detention practices: Statement of a global taskforce. Lancet 2015, 386, 649. [Google Scholar] [CrossRef]
- Mehta, P.S.; Wiernikowski, J.T.; Petrilli, J.A.; Barr, R.D. Essential medicines for pediatric oncology in developing countries. Pediatr. Blood Cancer 2013, 60, 889–891. [Google Scholar] [CrossRef] [PubMed]
- Hadley, G.P.; Mars, M.; Ramdial, P.K. Bilateral Wilms’ tumour in a developing country: A descriptive study. Pediatr. Surg. Int. 2013, 29, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Magrath, I.; Steliarova-Foucher, E.; Epelman, S.; Ribeiro, R.C.; Harif, M.; Li, C.K.; Kebudi, R.; Macfarlane, S.D.; Howard, S.C. Paediatric cancer in low-income and middle-income countries. Lancet. Oncol. 2013, 14, e104–e116. [Google Scholar] [CrossRef]
- Graf, N.; Tournade, M.F.; de Kraker, J. The role of preoperative chemotherapy in the management of Wilms’ tumor. The SIOP studies. International Society of Pediatric Oncology. Urol. Clin. N. Am. 2000, 27, 443–454. [Google Scholar] [CrossRef]
- Gupta, S.; Howard, S.; Hunger, S. Treating Childhood Cancer in Low- and Middle-Income Countries. In Cancer: Disease Control Priorities, 3rd ed.; Gelband, H., Jha, P., Sankaranarayanan, R., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2015; Volume 3. [Google Scholar]
- Mitchell, C.; Pritchard-Jones, K.; Shannon, R.; Hutton, C.; Stevens, S.; Machin, D.; Imeson, J.; Kelsey, A.; Vujanic, G.M.; Gornall, P.; et al. Immediate nephrectomy versus preoperative chemotherapy in the management of non-metastatic Wilms’ tumour: Results of a randomised trial (UKW3) by the UK Children’s Cancer Study Group. Eur. J. Cancer 2006, 42, 2554–2562. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel-Eibrink, M.M.; Hol, J.A.; Pritchard-Jones, K.; van Tinteren, H.; Furtwangler, R.; Verschuur, A.C.; Vujanic, G.M.; Leuschner, I.; Brok, J.; Rube, C.; et al. Position paper: Rationale for the treatment of Wilms tumour in the UMBRELLA SIOP-RTSG 2016 protocol. Nat. Rev. Urol. 2017, 14, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Israels, T.; Renner, L.; Hendricks, M.; Hesseling, P.; Howard, S.; Molyneux, E. SIOP PODC: Recommendations for supportive care of children with cancer in a low-income setting. Pediatr. Blood Cancer 2013, 60, 899–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Israels, T.; Paintsil, V.; Nyirenda, D.; Kouya, F.; Mbah Afungchwi, G.; Hesseling, P.; Tump, C.; Kaspers, G.; Burns, L.; Singh Arora, R.; et al. Improved outcome at end of treatment in the collaborative Wilms tumour Africa project. Pediatr. Blood Cancer 2018, 65, e26945. [Google Scholar] [CrossRef] [PubMed]
- Parikh, N.S.; Howard, S.C.; Chantada, G.; Israels, T.; Khattab, M.; Alcasabas, P.; Lam, C.G.; Faulkner, L.; Park, J.R.; London, W.B.; et al. SIOP-PODC adapted risk stratification and treatment guidelines: Recommendations for neuroblastoma in low- and middle-income settings. Pediatr. Blood Cancer 2015, 62, 1305–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chantada, G.; Luna-Fineman, S.; Sitorus, R.S.; Kruger, M.; Israels, T.; Leal-Leal, C.; Bakhshi, S.; Qaddoumi, I.; Abramson, D.H.; Doz, F. SIOP-PODC recommendations for graduated-intensity treatment of retinoblastoma in developing countries. Pediatr. Blood Cancer 2013, 60, 719–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadley, G.P.; van Heerden, J. High-risk neuroblastoma in a sub-Saharan African country: Telling it like it is. Trop. Dr. 2017, 47, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Kamihara, J.; Ma, C.; Fuentes Alabi, S.L.; Garrido, C.; Frazier, A.L.; Rodriguez-Galindo, C.; Orjuela, M.A. Socioeconomic status and global variations in the incidence of neuroblastoma: Call for support of population-based cancer registries in low-middle-income countries. Pediatr. Blood Cancer 2017, 64, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Dimaras, H.; Corson, T.W.; Cobrinik, D.; White, A.; Zhao, J.; Munier, F.L.; Abramson, D.H.; Shields, C.L.; Chantada, G.L.; Njuguna, F.; et al. Retinoblastoma. Nat. Rev. Dis. Primers 2015, 1, 15021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, S.W.; Millar, A.J.; Hadley, G.P.; Ionescu, G.; Kruger, M.; Poole, J.; Stones, D.; Wainwright, L.; Chitnis, M.; Wessels, G. Hepatocellular carcinoma and liver tumors in South African children: A case for increased prevalence. Cancer 2004, 101, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.W.; Davidson, A.; Hadley, G.P.; Kruger, M.; Poole, J.; Stones, D.; Wainwright, L.; Wessels, G. Malignant liver tumors in South African children: A national audit. World J. Surg. 2008, 32, 1389–1395. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, P.; Ortiz, R.; Fuentes, S.; Gamboa, Y.; Ah Chu-Sanchez, M.S.; Arambu, I.C.; Montero, M.; Baez, F.; Rodriguez-Galindo, C.; Antillon-Klussmann, F. Barriers to effective treatment of pediatric solid tumors in middle-income countries: Can we make sense of the spectrum of nonbiologic factors that influence outcomes? Cancer 2014, 120, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Soerjomataram, I.; Lortet-Tieulent, J.; Parkin, D.M.; Ferlay, J.; Mathers, C.; Forman, D.; Bray, F. Global burden of cancer in 2008: A systematic analysis of disability-adjusted life-years in 12 world regions. Lancet 2012, 380, 1840–1850. [Google Scholar] [CrossRef]
- Aminkeng, F.; Ross, C.J.; Rassekh, S.R.; Brunham, L.R.; Sistonen, J.; Dube, M.P.; Ibrahim, M.; Nyambo, T.B.; Omar, S.A.; Froment, A.; et al. Higher frequency of genetic variants conferring increased risk for ADRs for commonly used drugs treating cancer, AIDS and tuberculosis in persons of African descent. Pharm. J. 2014, 14, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Israels, T.; Ribeiro, R.C.; Molyneux, E.M. Strategies to improve care for children with cancer in Sub-Saharan Africa. Eur. J. Cancer 2010, 46, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Israels, T.; Bailey, S.; Verschoor, R.; Kaspers, G.J.; Kennedy, N.; Molyneux, E.M. Management of children with Wilms tumor in Africa and Europe; thoughts about costs, priorities and collaboration. Pediatr. Hematol. Oncol. 2014, 31, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Hadley, L.G.; Rouma, B.S.; Saad-Eldin, Y. Challenge of pediatric oncology in Africa. Semin. Pediatr. Surg. 2012, 21, 136–141. [Google Scholar] [CrossRef] [PubMed]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carter, N.H.; Avery, A.H.; Libes, J.; Lovvorn, H.N., III; Hansen, E.N. Pediatric Solid Tumors in Resource-Constrained Settings: A Review of Available Evidence on Management, Outcomes, and Barriers to Care. Children 2018, 5, 143. https://doi.org/10.3390/children5110143
Carter NH, Avery AH, Libes J, Lovvorn HN III, Hansen EN. Pediatric Solid Tumors in Resource-Constrained Settings: A Review of Available Evidence on Management, Outcomes, and Barriers to Care. Children. 2018; 5(11):143. https://doi.org/10.3390/children5110143
Chicago/Turabian StyleCarter, Nicholas H., Andrew H. Avery, Jaime Libes, Harold N. Lovvorn, III, and Erik N. Hansen. 2018. "Pediatric Solid Tumors in Resource-Constrained Settings: A Review of Available Evidence on Management, Outcomes, and Barriers to Care" Children 5, no. 11: 143. https://doi.org/10.3390/children5110143
APA StyleCarter, N. H., Avery, A. H., Libes, J., Lovvorn, H. N., III, & Hansen, E. N. (2018). Pediatric Solid Tumors in Resource-Constrained Settings: A Review of Available Evidence on Management, Outcomes, and Barriers to Care. Children, 5(11), 143. https://doi.org/10.3390/children5110143