Immersive Virtual Reality as Analgesia during Dressing Changes of Hospitalized Children and Adolescents with Burns: A Systematic Review with Meta-Analysis

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Data Collection
2.3.1. Studies Selection
2.3.2. Data Extraction
2.4. Data Analysis
2.4.1. Assessment of Study Quality
Quality of Evidence
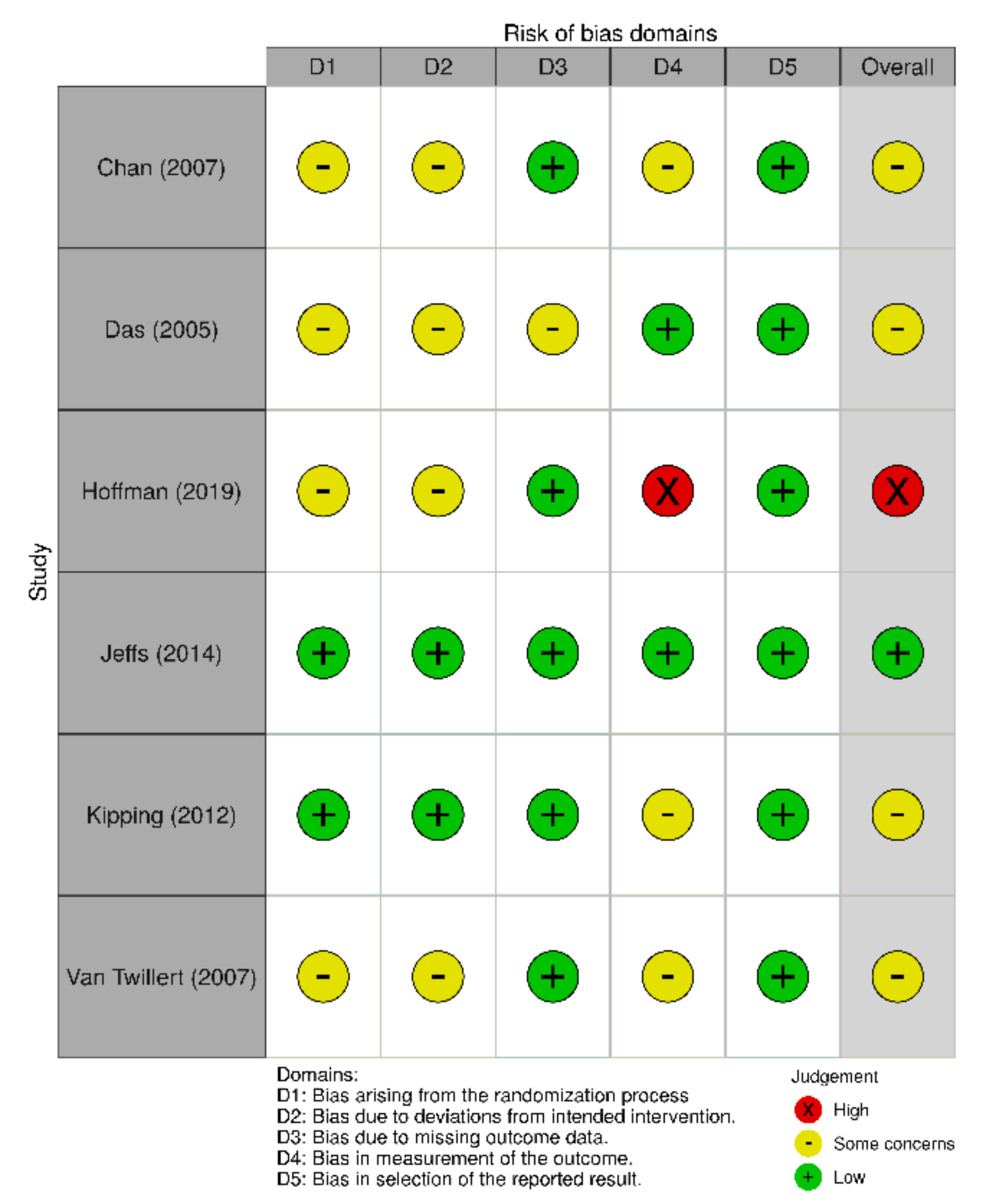
Assessment of Risk of Bias
2.4.2. Synthesis of Results
Measures of Treatment Effect
Dealing with Missing Data
Data Synthesis
3. Results
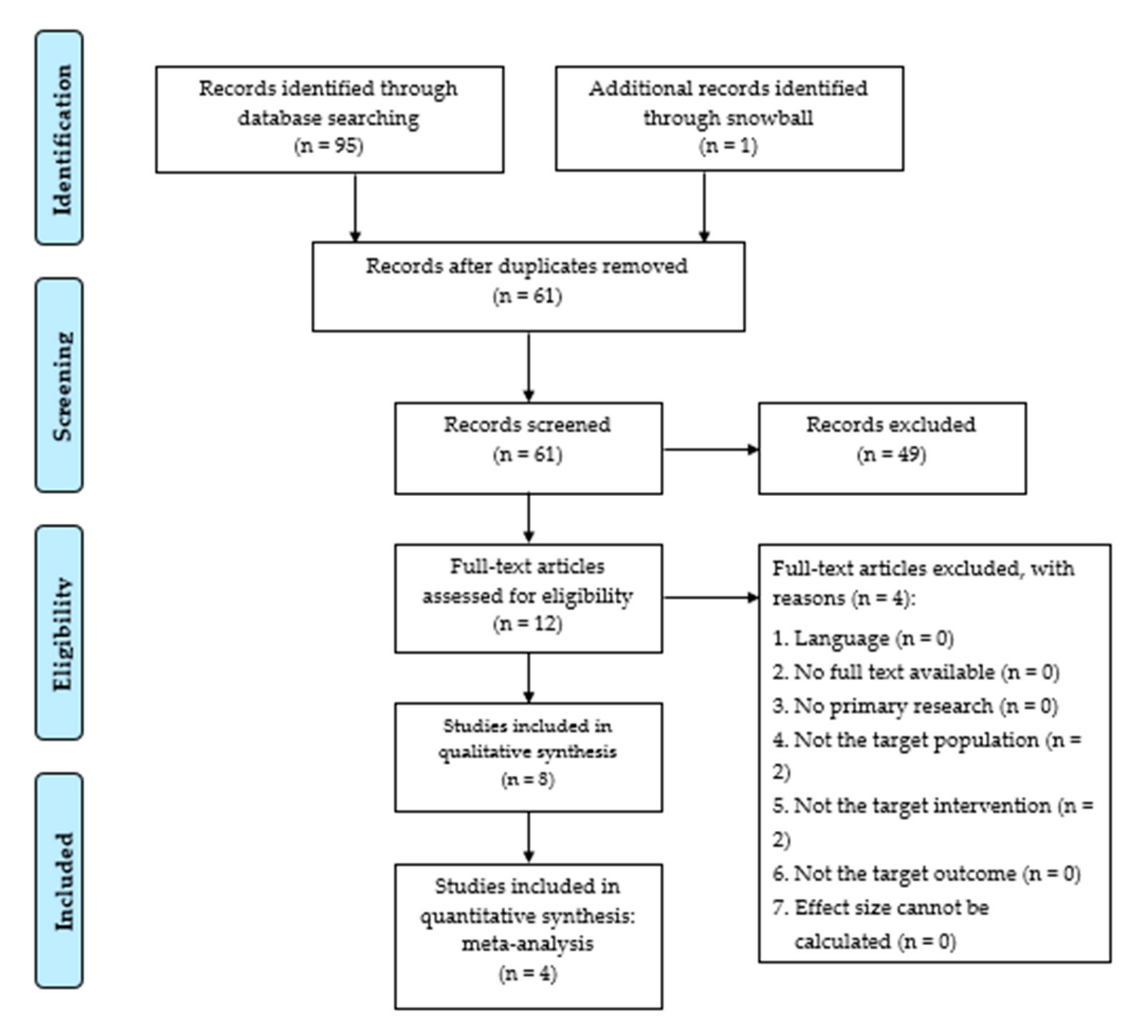
3.1. Description of Studies
3.1.1. Excluded Studies
3.1.2. Included Studies
3.2. Study Quality Assessment
3.2.1. Quality of Evidence
3.2.2. Risk of Bias
Randomized Control Trials
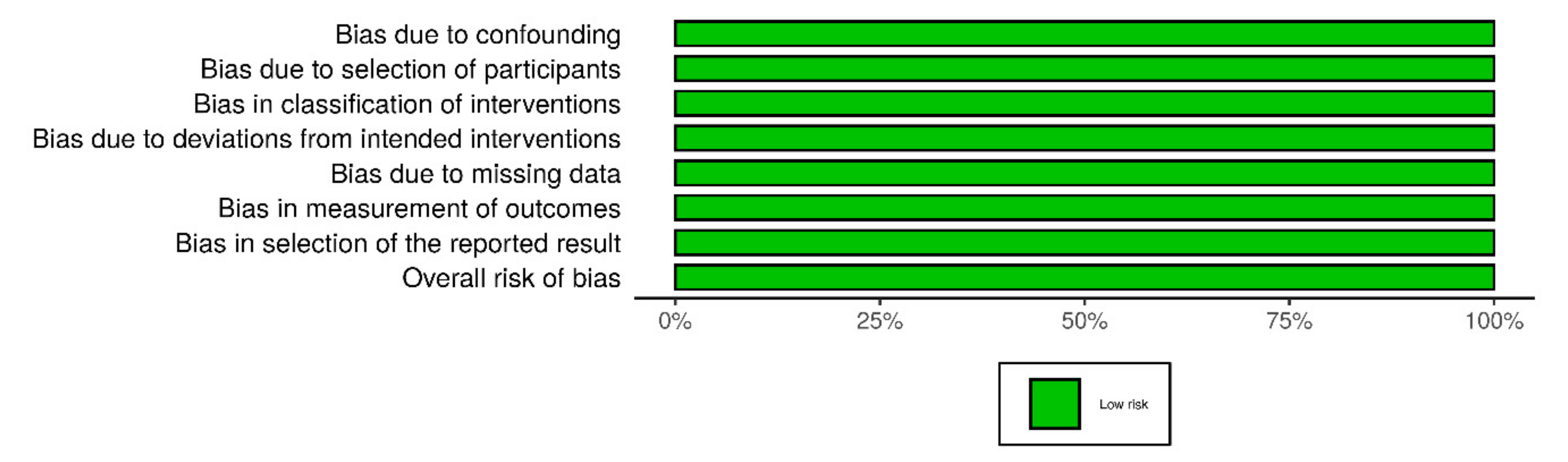
Non-Randomized Studies
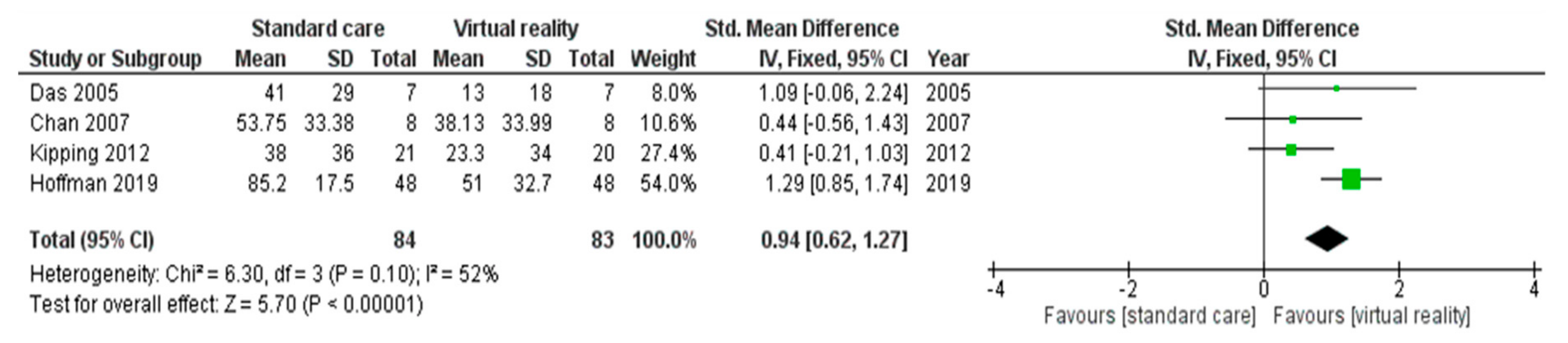
3.2.3. Effect of the Intervention
Summary of Results for Studies Excluded from the Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Title | Study Design | Patients n * (Age) | Study Population | Moment of VR | Duration of VR |
|---|---|---|---|---|---|---|
| Chan (2007) [13] | Application of a virtual reality prototype for pain relief of pediatric burn in Taiwan | RCT: within-subjects, cross-over design | 8 (Mean 6,54 (SD = 2.27)) | Hospitalized pediatric patients with burns | During burn dressing change | 15–35 min |
| Das (2005) [9] | The efficacy of playing a virtual reality game in modulating pain for children with acute burn injuries: a randomized controlled trial [ISRCTN87413556] | RCT: within-subjects design | 7 (5–16) | Hospitalized children with a TBSA >3% and requiring dressing changes | During burn dressing change | 10–45 min |
| Hoffman (2000) [28] | Virtual reality as an adjunctive pain control during burn wound care in adolescent patients | case series | 2 (16 and 17) | Hospitalized pediatric patients with burns | During burn dressing change | 3 min |
| Hoffman (2019) [31] | Immersive Virtual Reality as an Adjunctive Non-opioid Analgesic for Predominantly Latin American Children With Large Severe Burn Wounds During Burn Wound Cleaning in the Intensive Care Unit: A Pilot Study | RCT: within-subjects, cross-over design | 48 (6–17) | Hospitalized children with a TBSA >10% | During burn dressing change | Mean 12.89 min |
| Jeffs (2014) [60] | Effect of virtual reality on adolescent pain during burn wound care | RCT: between-subjects, parallel design | 28 (10–17) | Hospitalized pediatric patients with burns | During burn dressing change | Mean 31.6 (SD = 30.8) min |
| Kipping (2012) [61] | Virtual reality for acute pain reduction in adolescents undergoing burn wound care: a prospective randomized controlled trial | RCT: between-subjects, parallel design | 41 (11–17) | Adolescents with a TBSA >1% | During burn dressing application | 2–62 min |
| Scapin (2017) [8] | Use of virtual reality for treating burned children: case reports | case series | 2 (8 and 9) | Hospitalized pediatric patients with burns | During burn dressing change | 25–35 min |
| Van Twillert (2007) [59] | Computer-generated virtual reality to control pain and anxiety in pediatric and adult burn patients during wound dressing changes | RCT: within-subjects design | 6 (8–18) | Hospitalized pediatric patients with burns without facial burns or other physical limitations | During burn dressing change | Mean 19.2 min |
| Author (Year) | VR Equipment | VR Environment |
|---|---|---|
| Chan (2007) [13] | VR-system with I-glasses and a computer mouse as input | The patient functioned as a patrol person for an ice-cream factory. The purpose was preventing the fox from harming the factory by shooting at it with ice-cream |
| Das (2005) [9] | A laptop (Dell Inspiron 5100, Pentium 4 2.4 Ghz CPU with a Radeon Mobility 7500 Video Card) with a head-mount display (HMD) (IOGlasses Head Mount Display with a SVGA video resolution of 800 × 600 16 million colors), with a tracking system (Intersense IS300 6 degree of freedom Inertia Cube with a USB-Serial converter, required for Inertia Cube) | The patient visualized being on a track, using a pointer to aim and shoot monsters |
| Hoffman (2000) [28] | A Silicon Graphics Octane MXE with Octane Channel Option coupled with a wide field of view head mounted visual display, a stationary Polhemus low energy source detected by movable Polhemus 6df sensors. Information about the sensor’s position relative to the source was fed into the VR computer system | The patient experienced SpiderWorld. Using tactile augmentation patients could ’physically’ touch the furry body of a virtual Guyana bird-eating tarantula with wiggling legs |
| Hoffman (2019) [31] | MX90 VR goggles from Nvis, with 90 degrees field of view diagonal, per eye, and 1280 × 1024 pixels resolution per eye. Held by the ’Magula arm’, a robot-like articulated arm goggle holder | SnowWorld is an iceworld where patients interact with snowmen, igloos, penguins, wooly mammoths, and flying fish by throwing snowballs. During VR, patients heard music and 3D sound effects e.g., ice breaking when a snowball hits a snowman, mammoths trumpeted angrily when pelted, etc. |
| Jeffs (2014) [60] | Kaiser Optics SR80a VR helmet with SXGA resolution (1280–1024) 80-degree field-of-view mounted on a custom-built, articulated-arm tripod device and via a desktop VR analgesia workstation Falcon NW Fragbox, with interactivity using a Kensington orbit trackball and music through Bose Quiet Comfort 3 headphones | SnowWorld is an iceworld where patients interact with snowmen, igloos, penguins, wooly mammoths, and flying fish by throwing snowballs. During VR, patients heard music and 3D sound effects e.g., ice breaking when a snowball hits a snowman, mammoths trumpeted angrily when pelted, etc. |
| Kipping (2012) [61] | Head mounted display (eMagin, Z800 3DVisor with head tracking, joystick hand control (LOGIK PC ATTACK 3), personal computer and off the-shelf software games | Chicken Little™ for the 11–13 years old, and an additional choice of Need for Speed™ for the 14–17 years old |
| Scapin (2017) [8] | Three-dimensional vision goggles and stereo sound from a Samsung Gear VR Innovator Edition for Note 4®. The images were reproduced by a Samsung Note S4® mobile phone | Roller coaster ride and a marine environment |
| Van Twillert (2007) [59] | Cybermind Hi-Res900 3D Head Mounted Display was used with an integrated audio system and controlled by a FasTrak control-box: the Polhemus FasTrak 6 DOF motion tracking system | SnowWorld is an iceworld where patients interact with snowmen, igloos, penguins, wooly mammoths, and flying fish by throwing snowballs. During VR, patients heard music and 3D sound effects e.g., ice breaking when a snowball hits a snowman, mammoths trumpeted angrily when pelted, etc. |
| Author (Year) | Treatment Conditions | Comparison Intervention | Key Findings |
|---|---|---|---|
| Chan (2007) [13] | VR distraction with a standard pharmacologic analgesic (Tylenol) | A standard pharmacologic analgesic (Tylenol) | In the VR-group less pain was experienced during dressing change, but this was not statistically significant compared to the non VR-group (df = 7, t = 1.58, p > 0.05) |
| Das (2005) [9] | VR distraction with routine pharmacological analgesia | Routine pharmacological analgesia | The average pain scores for only pharmacological analgesia was 4.1 (SD = 2.9), while VR coupled with pharmacological analgesia, the average pain score was 1.3 (SD = 1.8). The mean pain score difference between administrations was 3.2 (SD 2.1), which was significant using paired t-tests (p < 0.01) |
| Hoffman (2000) [28] | VR distraction with standard pharmacological analgesia | Nintendo 64 with standard pharmacological analgesia | Both patients showed drops in pain during VR treatment compared to the comparison intervention |
| Hoffman (2019) [31] | VR distraction with the usual standard pharmacological analgesia | Traditional pharmacological analgesia | VR significantly reduced children’s pain ratings during dressing change. Worst pain during No VR = 8.52 (SD = 1.75) vs. during Yes VR = 5.10 (SD = 3.27), t(47) = 7.11, p < 0.001, SD = 3.33, CI = 2.45–4.38, Cohen’s d = 1.03 |
| Jeffs (2014) [60] | VR distraction with standard care | Standard care | Participants in the VR group reported less procedural pain compared with the SC group (difference = 9.7 mm, 95% CI: −9.5 to 28.9, p = 32). Pair-wise effect sizes were estimated between treatment groups. The estimated effect size between VR and SC groups was 0.535 |
| Kipping (2012) [61] | VR distraction with standard medication protocols (Entonox) | Standard medication protocols (Entonox) with the possibility of TV, stories, music, caregivers or no distraction | The self-reported pain experienced during dressing application was lower in the VRG than the SDG. However, the difference was not statistically significant |
| Scapin (2017) [8] | VR distraction with standard pharmacological treatment (Morphine) | Standard pharmacological treatment (Morphine) | Case 1: during the standard care the child scored his pain the maximum FACE-scale value (10/10). During VR intervention he scored his pain 4/10. Case 2: during standard care the child rated his pain 6/10. During the VR treatment was the pain rated 0/10 |
| Van Twillert (2007) [59] | VR distraction with standard pharmacological analgesia | Standard pharmacological care and the possibility of alternative distractions (TV, stories, music, caregivers or no distraction) | Mean pain experienced by patients younger than 18: VR: 2.90 vs. SC: 5.85. Mean difference between VR and SC was −2.95 (p: 0.688) |
| Author (Year) | Type of Outcome Measure | Moment of Outcome Measure | Quality Assessment | Risk of Bias | Statistical Significance | Effect Size | 95% CI (Lower Bounds) | 95% CI (Upper Bounds) |
|---|---|---|---|---|---|---|---|---|
| Chan (2007) [13] | Faces scale (0–100) | Before, during and after dressing change | PEDro-scale: 7/11 | RoB 2: some concerns | p > 0.05 | 0.44 | −0.56 | 1.43 |
| Das (2005) [9] | Faces scale (0–10) | After dressing change | PEDro-scale: 7/11 | RoB 2: some concerns | p < 0.01 | 1.09 | −0.06 | 2.24 |
| Hoffman (2000) [28] | Visual analogue scale (0–100) | After dressing change | MD&B: 15/27 | ROBINS-I: low risk | / | / | / | / |
| Hoffman (2019) [31] | Graphic rating scales (0–10) | After dressing change | PEDro-scale: 7/11 | RoB 2: high risk | p < 0.001 | 1.29 | 0.85 | 1.74 |
| Jeffs (2014) [60] | Adolescent pediatric pain tool—Word graphic rating scale (0–100) | After dressing change | PEDro-scale: 7/11 | RoB 2: low risk | p = 0.32 | 0.53 | −9.50 | 28.90 |
| Kipping (2012) [61] | Visual analog scale (0–10) | Before, during and after dressing change | PEDro-scale: 8/11 | RoB 2: some concerns | p = 0.40 | 0.41 | −0.21 | 1.03 |
| Scapin (2017) [8] | Faces scale (0–10) | Before, during and after dressing change | MD&B: 15/27 | ROBINS-I: low risk | / | / | / | / |
| Van Twillert (2007) [59] | Graphic rating scales (0–10) | During dressing change | PEDro-scale: 7/11 | RoB 2: some concerns | p = 0.68 | / | / | / |
| N° | Criteria | Evaluation |
|---|---|---|
| 1. | Eligibility criteria were specified? | Yes (1)/No (0) |
| 2. | Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received)? | Yes (1)/No (0) |
| 3. | Allocation was concealed? | Yes (1)/No (0) |
| 4. | The groups were similar at baseline regarding the most important prognostic indicators? | Yes (1)/No (0) |
| 5. | There was blinding of all subjects? | Yes (1)/No (0) |
| 6. | There was blinding of all therapists who administered the therapy? | Yes (1)/No (0) |
| 7. | There was blinding of all assessors who measured at least one key outcome? | Yes (1)/No (0) |
| 8. | Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups? | Yes (1)/No (0) |
| 9. | All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat”? | Yes (1)/No (0) |
| 10. | The results of between-group statistical comparisons are reported for at least one key outcome? | Yes (1)/No (0) |
| 11. | The study provides both point measures and measures of variability for at least one key outcome? | Yes (1)/No (0) |
| N° | Criteria | Evaluation |
|---|---|---|
| 1. | Is the hypothesis/aim/objective of the study clearly described? | Yes (1)/No (0) |
| 2. | Are the main outcomes to be measured clearly described in the Introduction or Methods section? | Yes (1)/No (0) |
| 3. | Are the characteristics of the patients included in the study clearly described? | Yes (1)/No (0) |
| 4. | Are the interventions of interest clearly described? | Yes (1)/No (0) |
| 5. | Are the distributions of principal confounders in each group of subjects to be compared clearly described? | Yes (2)/Partially (1)/No (0) |
| 6. | Are the main findings of the study clearly described? | Yes (1)/No (0) |
| 7. | Does the study provide estimates of the random variability in the data for the main outcomes? | Yes (1)/No (0) |
| 8. | Have all important adverse events that may be a consequence of the intervention been reported? | Yes (1)/No (0) |
| 9. | Have the characteristics of patients lost to follow-up been described? | Yes (1)/No (0) |
| 10. | Have actual probability values been reported (e.g., 0.035 rather than < 0.05) for the main outcomes except where the probability value is less than 0.001? | Yes (1)/No (0) |
| 11. | Were the subjects asked to participate in the study representative of the entire population from which they were recruited? | Yes (1)/No (0)/Unable to determine (0) |
| 12. | Were those subjects who were prepared to participate representative of the entire population from which they were recruited? | Yes (1)/No (0)/Unable to determine (0) |
| 13. | Were the staff, places, and facilities where the patients were treated, representative of the treatment the majority of patients receive? | Yes (1)/No (0)/Unable to determine (0) |
| 14. | Was an attempt made to blind study subjects to the intervention they have received? | Yes (1)/No (0)/Unable to determine (0) |
| 15. | Was an attempt made to blind those measuring the main outcomes of the intervention? | Yes (1)/No (0)/Unable to determine (0) |
| 16. | If any of the results of the study were based on “data dredging”, was this made clear? | Yes (1)/No (0)/Unable to determine (0) |
| 17. | In trials and cohort studies, do the analyses adjust for different lengths of follow-up of patients, or in case-control studies, is the time period between the intervention and outcome the same for cases and controls? | Yes (1)/No (0)/Unable to determine (0) |
| 18. | Were the statistical tests used to assess the main outcomes appropriate? | Yes (1)/No (0)/Unable to determine (0) |
| 19. | Was compliance with the intervention/s reliable? | Yes (1)/No (0)/Unable to determine (0) |
| 20. | Were the main outcome measures used accurate (valid and reliable)? | Yes (1)/No (0)/Unable to determine (0) |
| 21. | Were the patients in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited from the same population? | Yes (1)/No (0)/Unable to determine (0) |
| 22. | Were study subjects in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited over the same period of time? | Yes (1)/No (0)/Unable to determine (0) |
| 23. | Were study subjects randomized to intervention groups? | Yes (1)/No (0)/Unable to determine (0) |
| 24. | Was the randomized intervention assignment concealed from both patients and health care staff until recruitment was complete and irrevocable? | Yes (1)/No (0)/Unable to determine (0) |
| 25. | Was there adequate adjustment for confounding in the analyses from which the main findings were drawn? | Yes (1)/No (0)/Unable to determine (0) |
| 26. | Were losses of patients to follow-up taken into account? | Yes (1)/No (0)/Unable to determine (0) |
| 27. | Did the study have sufficient power to detect a clinically important effect where the probability value for a difference being due to chance is less than 5%? | <n1 (0)/n1 - n2 (1)/n3 - n4 (2)/n5 - n6 (3)/n7 - n8 (4)/>n8 (5) |



References
- Elrod, J.; Schiestl, C.M.; Mohr, C.; Landolt, M.A. Incidence, severity and pattern of burns in children and adolescents: An epidemiological study among immigrant and Swiss patients in Switzerland. Burns 2019, 45, 1231–1241. [Google Scholar] [CrossRef] [PubMed]
- Bayat, A.; Ramaiah, R.; Bhananker, S.M. Analgesia and sedation for children undergoing burn wound care. Expert Rev. Neurother. 2010, 10, 1747–1759. [Google Scholar] [CrossRef] [PubMed]
- Stichting Brandwonden Epidemologie. Available online: www.brandwonden.be/nl/brandwondenzorg/eerste-hulp/epidemologie (accessed on 5 April 2020).
- Louw, Q.; Grimmer-Somers, K.; Schrikk, A. Measuring children’s distress during burns dressing changes: Literature search for measures appropriate for indigenous children in South Africa. J. Pain Res. 2011, 4, 263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herndon, D.N. Total Burn Care, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2012; ISBN 9781437727869. [Google Scholar]
- Godambe, S.A.; Elliot, V.; Matheny, D.; Pershad, J. Comparison of Propofol/Fentanyl Versus Ketamine/Midazolam for Brief Orthopedic Procedural Sedation in a Pediatric Emergency Department. Pediatrics 2003, 112, 116–123. [Google Scholar] [CrossRef]
- Mather, L.; Mackie, J. The incidence of postoperative pain in children. Pain 1983, 15, 271–282. [Google Scholar] [CrossRef]
- Scapin, S.Q.; Echevarría-Guanilo, M.E.; Fuculo, P.R.B.; Martins, J.C.; Barbosa, M.d.V.; Pereima, M.J.L. Use of virtual reality for treating burned children: Case reports. Rev. Bras. Enferm. 2017, 70, 1291–1295. [Google Scholar] [CrossRef] [Green Version]
- Das, D.A.; Grimmer, K.A.; Sparnon, A.L.; McRae, S.E.; Thomas, B.H. The efficacy of playing a virtual reality game in modulating pain for children with acute burn injuries: A randomized controlled trial [ISRCTN87413556]. BMC Pediatr. 2005, 5, 1. [Google Scholar] [CrossRef]
- Christian, L.M.; Graham, J.E.; Padgett, D.A.; Glaser, R.; Kiecolt-Glaser, J.K. Stress and Wound Healing. Neuroimmunomodulation 2006, 13, 337–346. [Google Scholar] [CrossRef] [Green Version]
- Widgerow, A.D.; Kalaria, S. Pain mediators and wound healing—Establishing the connection. Burns 2012, 38, 951–959. [Google Scholar] [CrossRef]
- Palos, G.R.; Mendoza, T.R.; Cantor, S.B.; Aday, L.A.; Cleeland, C.S. Perceptions of analgesic use and side effects: What the public values in pain management. J. Pain Symptom Manag. 2004, 28, 460–473. [Google Scholar] [CrossRef]
- Chan, E.A.; Chung, J.W.Y.; Wong, T.K.S.; Lien, A.S.Y.; Yang, J.Y. Application of a virtual reality prototype for pain relief of pediatric burn in Taiwan. J. Clin. Nurs. 2007, 16, 786–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benyamin, R.; Trescot, A.M.; Datta, S.; Buenaventura, R.; Adlaka, R.; Sehgal, N.; Glaser, S.E.; Vallejo, R. Opioid complications and side effects. Pain Physician 2008, 11, S105–S120. [Google Scholar] [CrossRef] [PubMed]
- Byers, J.F.; Bridges, S.; Kijek, J.; LaBorde, P. Burn Patients’ Pain and Anxiety Experiences. J. Burn Care Res. 2001, 22, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Chonière, M.; Melzack, R.; Rondeau, J.; Girard, N.; Paquin, M.-J. The Pain of Burns. J. Trauma 1989, 29, 1531–1539. [Google Scholar] [CrossRef]
- Perry, S.; Heidrich, G.; Ramos, E. Assessment of Pain by Burn Patients. J. Burn Care Res. 1981, 2, 322–326. [Google Scholar] [CrossRef]
- Koller, D.; Goldman, R.D. Distraction Techniques for Children Undergoing Procedures: A Critical Review of Pediatric Research. J. Pediatr. Nurs. 2012, 27, 652–681. [Google Scholar] [CrossRef]
- McDonnell, N. Immersive Technology and Medical Visualisation: A Users Guide. In Biomedical Visualisation. Advances in Experimental Medicine and Biology; Springer: Cham, Switzerland, 2019; Volume 1156, pp. 123–134. [Google Scholar]
- Poetker, B. What Is Virtual Reality? Available online: https://learn.g2.com/virtual-reality (accessed on 14 May 2020).
- Marr, B. The Important Difference between Virtual Reality, Augmented Reality and Mixed Reality. Available online: www.forbes.com/sites/bernardmarr/2019/07/19/the-important-difference-between-virtual-reality-augmented-reality-and-mixed-reality/ (accessed on 29 April 2020).
- Garrett, B.; Taverner, T.; Masinde, W.; Gromala, D.; Shaw, C.; Negraeff, M. A Rapid Evidence Assessment of Immersive Virtual Reality as an Adjunct Therapy in Acute Pain Management in Clinical Practice. Clin. J. Pain 2014, 30, 1089–1098. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Seibel, E.J.; Richards, T.L.; Furness, T.A.; Patterson, D.R.; Sharar, S.R. Virtual Reality Helmet Display Quality Influences the Magnitude of Virtual Reality Analgesia. J. Pain 2006, 7, 843–850. [Google Scholar] [CrossRef]
- Macedonio, M.F.; Parsons, T.D.; Digiuseppe, R.A.; Weiderhold, B.A.; Rizzo, A.A. Immersiveness and Physiological Arousal within Panoramic Video-Based Virtual Reality. Cyberpsychol. Behav. 2007, 10, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Malloy, K.M.; Milling, L.S. The effectiveness of virtual reality distraction for pain reduction: A systematic review. Clin. Psychol. Rev. 2010, 30, 1011–1018. [Google Scholar] [CrossRef]
- Shahrbanian, S.; Xiaoli, M.A.; Korner-Bitensky, N.; Simmonds, M.J. Scientific evidence for the effectiveness of virtual reality for pain reduction in adults with acute or chronic pain. In Proceedings of the Studies in Health Technology and Informatics; IOS Press: Amsterdam, The Netherlands, 2009; Volume 144, pp. 40–43. [Google Scholar]
- Wender, R.; Hoffman, H.G.; Hunner, H.H.; Seibel, E.J.; Patterson, D.R.; Sharar, S.R. Interactivity influences the magnitude of virtual reality analgesia. J. Cyber. Ther. Rehabil. 2009, 2, 27–33. [Google Scholar] [PubMed]
- Hoffman, H.G.; Doctor, J.N.; Patterson, D.R.; Carrougher, G.J.; Furness, T.A. Virtual reality as an adjunctive pain control during burn wound care in adolescent patients. Pain 2000, 85, 305–309. [Google Scholar] [CrossRef]
- Geisser, M.E.; Bingham, H.G.; Robinson, M.E. Pain and anxiety during burn dressing changes: Concordance between patients’ and nurses’ ratings and relation to medication administration and patient variables. J. Burn Care Rehabil. 1995, 16, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.-Y. Cognitive and cognitive-behavioral methods for pain control: A selective review. Pain 1982, 12, 201–228. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Rodriguez, R.A.; Gonzalez, M.; Bernardy, M.; Peña, R.; Beck, W.; Patterson, D.R.; Meyer, W.J. Immersive Virtual Reality as an Adjunctive Non-opioid Analgesic for Pre-dominantly Latin American Children with Large Severe Burn Wounds During Burn Wound Cleaning in the Intensive Care Unit: A Pilot Study. Front. Hum. Neurosci. 2019, 13, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallari, B.; Spaeth, E.K.; Goh, H.; Boyd, B.S. Virtual reality as an analgesic for acute and chronic pain in adults: A systematic review and meta-analysis. J. Pain Res. 2019, 12, 2053–2085. [Google Scholar] [CrossRef] [Green Version]
- Kahneman, D. Attention and Effort; Prentice-Hall: Englewood Cliffs, NJ, USA, 1973; ISBN 0130505188. [Google Scholar]
- Melzack, R.; Wall, P.D. Pain Mechanisms: A New Theory. Science 1965, 150, 971–978. [Google Scholar] [CrossRef]
- Hoffman, H. Virtual Reality: A New Tool for Interdisciplinary Psychology Research. Cyberpsychol. Behav. 1998, 1, 195–200. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Chambers, G.T.; Meyer, W.J.; Arceneaux, L.L.; Russell, W.J.; Seibel, E.J.; Richards, T.L.; Sharar, S.R.; Patterson, D.R. Virtual Reality as an Adjunctive Non-pharmacologic Analgesic for Acute Burn Pain During Medical Procedures. Ann. Behav. Med. 2011, 41, 183–191. [Google Scholar] [CrossRef] [Green Version]
- Arane, K.; Behboudi, A.; Goldman, R.D. Virtual reality for pain and anxiety management in children. Can. Fam. Physician 2017, 63, 932–934. [Google Scholar]
- Pourmand, A.; Davis, S.; Marchak, A.; Whiteside, T.; Sikka, N. Virtual Reality as a Clinical Tool for Pain Management. Curr. Pain Headache Rep. 2018, 22, 53. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M. Virtual Reality May Help Children Undergoing Chemotherapy. J. Natl. Cancer Inst. 2001, 93, 675–676. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.; Rodger, S.; Bucolo, S.; Greer, R.; Kimble, R.M. Multi-modal distraction. Using technology to combat pain in young children with burn injuries. Burns 2010, 36, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Morris, L.D.; Louw, Q.A.; Grimmer-Somers, K. The Effectiveness of Virtual Reality on Reducing Pain and Anxiety in Burn Injury Patients. Clin. J. Pain 2009, 25, 815–826. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Patterson, D.R.; Magula, J.; Carrougher, G.J.; Zeltzer, K.; Dagadakis, S.; Sharar, S.R. Water-friendly virtual reality pain control during wound care. J. Clin. Psychol. 2004, 60, 189–195. [Google Scholar] [CrossRef]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, i4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, L.A. Robvis: An R Package and Web Application for Visualising Risk-of-Bias Assessments. Available online: https://github.com/mcguinlu/robvis (accessed on 9 April 2020).
- Review Manager (RevMan 5.3). Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman (accessed on 9 April 2020).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 2013; ISBN 9780203771587. [Google Scholar]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Version 6; Wiley: Hoboken, NJ, USA, 2019; ISBN 9781119536628. [Google Scholar]
- Higgins, J.P.T. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faber, A.W.; Patterson, D.R.; Bremer, M. Repeated Use of Immersive Virtual Reality Therapy to Control Pain During Wound Dressing Changes in Pediatric and Adult Burn Patients. J. Burn Care Res. 2013, 34, 563–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, Y.; Qiu, R.; Yao, W.; Zhang, Q.; Chen, X. The Effect of Virtual Reality Distraction on Pain Relief During Dressing Changes in Children with Chronic Wounds on Lower Limbs. Pain Manag. Nurs. 2015, 16, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H.G.; Patterson, D.R.; Carrougher, G.J.; Sharar, S.R. Effectiveness of virtual reality-based pain control with multiple treatments. Clin. J. Pain 2001, 17, 229–235. [Google Scholar] [CrossRef]
- Mott, J.; Bucolo, S.; Cuttle, L.; Mill, J.; Hilder, M.; Miller, K.; Kimble, R.M. The efficacy of an augmented virtual reality system to alleviate pain in children undergoing burns dressing changes: A randomised controlled trial. Burns 2008, 34, 803–808. [Google Scholar] [CrossRef]
- Phelan, I.; Furness, P.J.; Fehily, O.; Thompson, A.R.; Babiker, N.T.; Lamb, M.A.; Lindley, S.A. A Mixed-Methods Investigation Into the Acceptability, Usability, and Perceived Effectiveness of Active and Passive Virtual Reality Scenarios in Managing Pain Under Experimental Conditions. J. Burn Care Res. 2019, 40, 85–90. [Google Scholar] [CrossRef]
- Schmitt, Y.S.; Hoffman, H.G.; Blough, D.K.; Patterson, D.R.; Jensen, M.P.; Soltani, M.; Carrougher, G.J.; Nakamura, D.; Sharar, S.R. A randomized, controlled trial of immersive virtual reality analgesia, during physical therapy for pediatric burns. Burns 2011, 37, 61–68. [Google Scholar] [CrossRef] [Green Version]
- van Twillert, B.; Bremer, M.; Faber, A.W. Computer-Generated Virtual Reality to Control Pain and Anxiety in Pediatric and Adult Burn Patients During Wound Dressing Changes. J. Burn Care Res. 2007, 28, 694–702. [Google Scholar] [CrossRef]
- Jeffs, D.; Dorman, D.; Brown, S.; Files, A.; Graves, T.; Kirk, E.; Meredith-Neve, S.; Sanders, J.; White, B.; Swearingen, C.J. Effect of Virtual Reality on Adolescent Pain During Burn Wound Care. J. Burn Care Res. 2014, 35, 395–408. [Google Scholar] [CrossRef] [Green Version]
- Kipping, B.; Rodger, S.; Miller, K.; Kimble, R.M. Virtual reality for acute pain reduction in adolescents undergoing burn wound care: A prospective randomized controlled trial. Burns 2012, 38, 650–657. [Google Scholar] [CrossRef]
- Choinière, M.; Auger, F.A.; Latarjet, J. Visual analogue thermometer: A valid and useful instrument for measuring pain in burned patients. Burns 1994, 20, 229–235. [Google Scholar] [CrossRef]
- Tesler, M.D.; Savedra, M.C.; Holzemer, W.L.; Wilkie, D.J.; Ward, J.A.; Paul, S.M. The word-graphic rating scale as a measure of children’s and adolescents’ pain intensity. Res. Nurs. Health 1991, 14, 361–371. [Google Scholar] [CrossRef]
- Scheffler, M.; Koranyi, S.; Meissner, W.; Strauß, B.; Rosendahl, J. Efficacy of non-pharmacological interventions for procedural pain relief in adults undergoing burn wound care: A systematic review and meta-analysis of randomized controlled trials. Burns 2018, 44, 1709–1720. [Google Scholar] [CrossRef] [PubMed]
- Birnie, K.A.; Noel, M.; Chambers, C.T.; Uman, L.S.; Parker, J.A. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Dahlquist, L.M.; Weiss, K.E.; Law, E.F.; Sil, S.; Herbert, L.J.; Horn, S.B.; Wohlheiter, K.; Ackerman, C.S. Effects of Videogame Distraction and a Virtual Reality Type Head-Mounted Display Helmet on Cold Pressor Pain in Young Elementary School-Aged Children. J. Pediatr. Psychol. 2010, 35, 617–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witmer, B.G.; Singer, M.J. Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence 1998, 7, 225–240. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauwens, Y.; Rafaatpoor, F.; Corbeel, K.; Broekmans, S.; Toelen, J.; Allegaert, K. Immersive Virtual Reality as Analgesia during Dressing Changes of Hospitalized Children and Adolescents with Burns: A Systematic Review with Meta-Analysis. Children 2020, 7, 194. https://doi.org/10.3390/children7110194
Lauwens Y, Rafaatpoor F, Corbeel K, Broekmans S, Toelen J, Allegaert K. Immersive Virtual Reality as Analgesia during Dressing Changes of Hospitalized Children and Adolescents with Burns: A Systematic Review with Meta-Analysis. Children. 2020; 7(11):194. https://doi.org/10.3390/children7110194
Chicago/Turabian StyleLauwens, Yannick, Fatemeh Rafaatpoor, Kobe Corbeel, Susan Broekmans, Jaan Toelen, and Karel Allegaert. 2020. "Immersive Virtual Reality as Analgesia during Dressing Changes of Hospitalized Children and Adolescents with Burns: A Systematic Review with Meta-Analysis" Children 7, no. 11: 194. https://doi.org/10.3390/children7110194