1. Introduction
Duchenne muscular dystrophy (DMD), an X-linked disorder due to lack of dystrophin, is characterized by progressive muscle weakness and myocardial dysfunction [
1]. DMD is typically diagnosed between the ages of 3 and 7 years and is characterized by progressive skeletal muscle weakness with loss of ambulation between the ages of 7 and 13 years [
2]. Without treatment, death secondary to cardiac or respiratory failure typically occurs in the second or third decade in DMD. Respiratory care of DMD patients has improved as a result of the development of supportive equipment and techniques [
3]. Advances in the respiratory care of patients with DMD have improved their prognosis. Nocturnal home ventilators and mechanically assisted coughing lead to improved survival of patients with DMD [
4]. The American Thoracic Society has published a statement regarding the respiratory care of patients with DMD, including evaluation and management (i.e., respiratory muscle training, mechanical ventilation, corticosteroids, and end of-life care) [
5]. These improvements in respiratory care make cardiac complications the leading cause of death in patients with DMD [
6,
7,
8,
9,
10]. Consequently, dilated cardiomyopathy and depressed cardiac function are increasing as the major cause of death.
Evidence of myocardial involvement begins with minor electrocardiographic abnormalities [
11]. Then cardiac involvement evolves to cardiomyopathy with dilatation of the cardiac chambers and depression of left ventricular ejection fraction due to widespread fibrosis. Progression of cardiomyopathy is the major cause of mortality. Cardiomyopathy can occur at any age but often occurs around 14–15 years [
12,
13].
Although cardiac dysfunction is treated with standard heart-failure strategies, it remains insufficient in DMD children. The treatment paradigms have been individually based and relied on evidence acquired from other patient populations [
2]. There are some reports that support the efficacy of angiotensin-converting enzyme inhibitors (ACEIs) on left ventricular function and mortality of DMD patients [
11]. In addition to ACEIs, angiotensin receptor blockers, beta-blockers, or aldosterone antagonists are often used for management of Duchenne cardiomyopathy and show improvements in cardiac function. Oral corticosteroid treatment can delay the onset of Duchenne cardiomyopathy [
14]. However, except for ACEIs, there are no reports on the efficacy of other medications.
Baseline assessment of cardiac function is needed for patients with DMD at diagnosis, and annual cardiac assessment is recommended for patients with DMD older than 10 years. Poor treatment outcomes have been noticed in patients with DMD who fail to see a cardiologist after the onset of clinical symptoms of heart failure [
2,
11,
12,
13].
In our hospital, we treated DMD cardiomyopathy patients with cardiac medication and respiratory care. After the start of treatment, we could see the improvement of patients’ early symptoms of heart failure like poor oral intake, night sweat, chest discomfort, fatigue, palpitation or sleep disturbance etc. Based on this, the purpose of this study was to evaluate the efficiency of cardiac medication in DMD cardiomyopathy patients with analyzing echocardiographic data to preserve the cardiac function.
3. Results
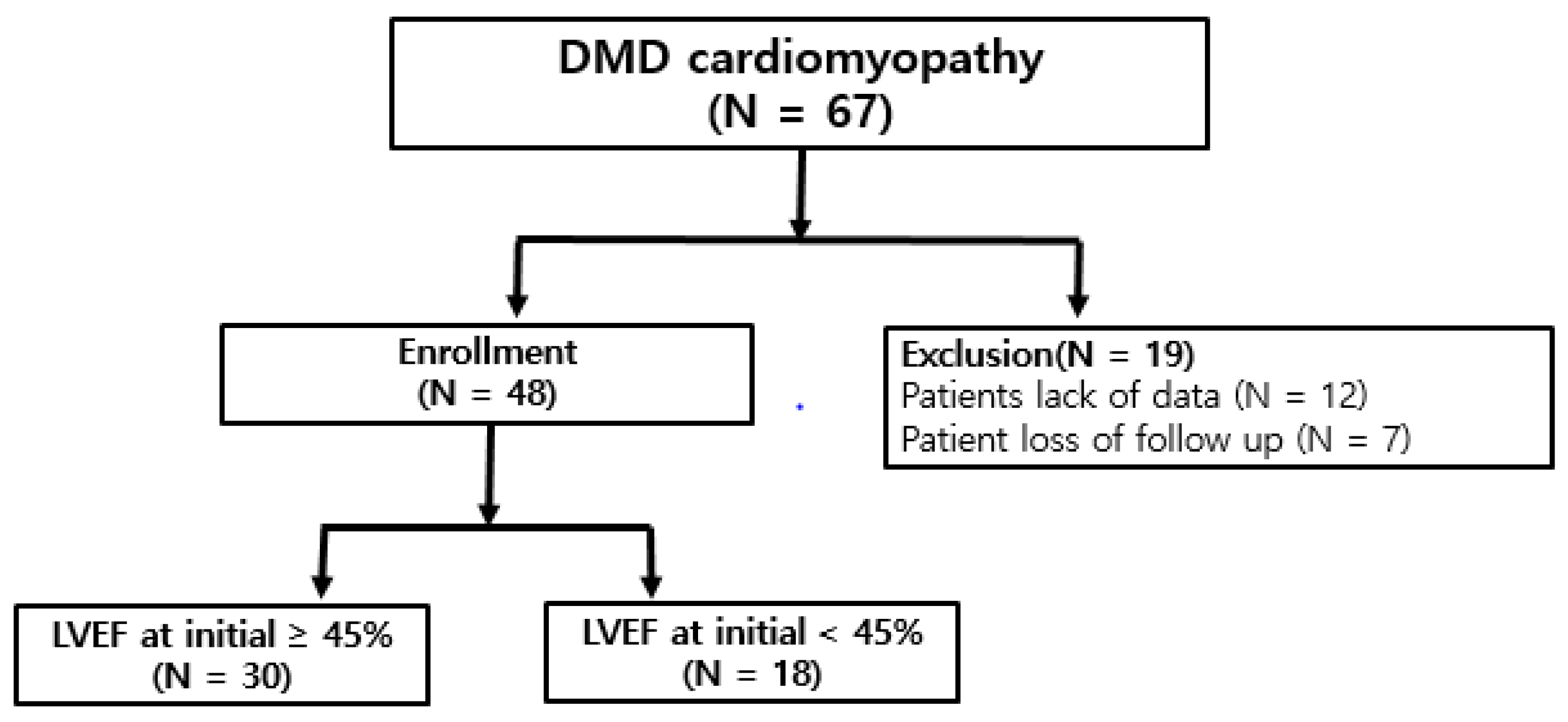
We reviewed 48 DMD patients and divided into two groups based on their ejection fraction at initial treatment. The demographic characteristics of patients with DMD are shown in
Table 1. All patients were male. Age at first medication in Group 2 (17.11 ± 2.30 years) was older than in Group 1 (14.3 ± 5.77 years) (
p < 0.05). For medications, Group 2 (4.6 ± 1.58) presented to take more kinds of medications than Group 1 (3.07 ± 1.26) (
p < 0.05). But onset age of ACE inhibitor was similar between two groups. For height and weight of the patients, Group 1 (143.663 ± 4.606 cm) was smaller than Group 2 (158.556 ± 1.7827 cm) (
p < 0.05) and Group 2 (45.7167 ± 2.822 kg) weighed more than Group 1 (34.7067± 2.5223 kg) (
p < 0.05). Ventilator apply time per day and initial end-tidal CO
2 (EtCO
2) was not significantly different between the two groups. Initial EtCO
2 was not statistically different between patients treated with ventilator and patients without ventilator. The follow-up duration was similar between two groups from 6 months to 4 years. They have been in treatment at least two years, and at most 6 years. As the time of their first clinic visit is individually different, the start of treatment is various for each patient.
The change values of systolic and diastolic echocardiographic data and the mean values of echocardiography which were taken before and after treatment are shown in
Table 2. The change values were significantly different in IVSd, IVSs, LVIDs, LVPWd, EF, FS, DT, DT slope, Lat A’ and Lat E/E’ (
p < 0.05). For the detail, IVSd became thinner by 0.07 cm and IVSs by 0.06 cm per year. LVPWd became thinner by 0.05 cm per year. LVIDs enlarged 0.13 cm per year. LV EF decreased 2.68%, FS 1.72% per year. With the Doppler data, DT decreased 7.3 ms, DT slope increased 0.6 m/s
2 per year. Lat A’ became shorter by 0.41 cm/s, Lateral E/E’ changed by 0.57 per year (
Table 2).
We assessed the impact of cardiac medication on these echocardiographic data with linear regression analysis (
Table 3). Most of the parameters are not statistically associated with the medications, except the relevance between IVSd and diuretics. The use of diuretics accelerated the thinning of IVSd by 0.06 cm per year (
p < 0.05).
The change values of the EF between Group 1 and Group 2 are shown in
Table 4. In Group 1, EF decreased with 3.62% per year of statistical significance, while in Group 2, EF became decreased with 0.58% per year (
p < 0.05). With the result in
Table 1, we compared medications in two groups to evaluate which medication related LV EF most. Obviously, inotropic agents were more taken in Group 2 patients (
Table 5).
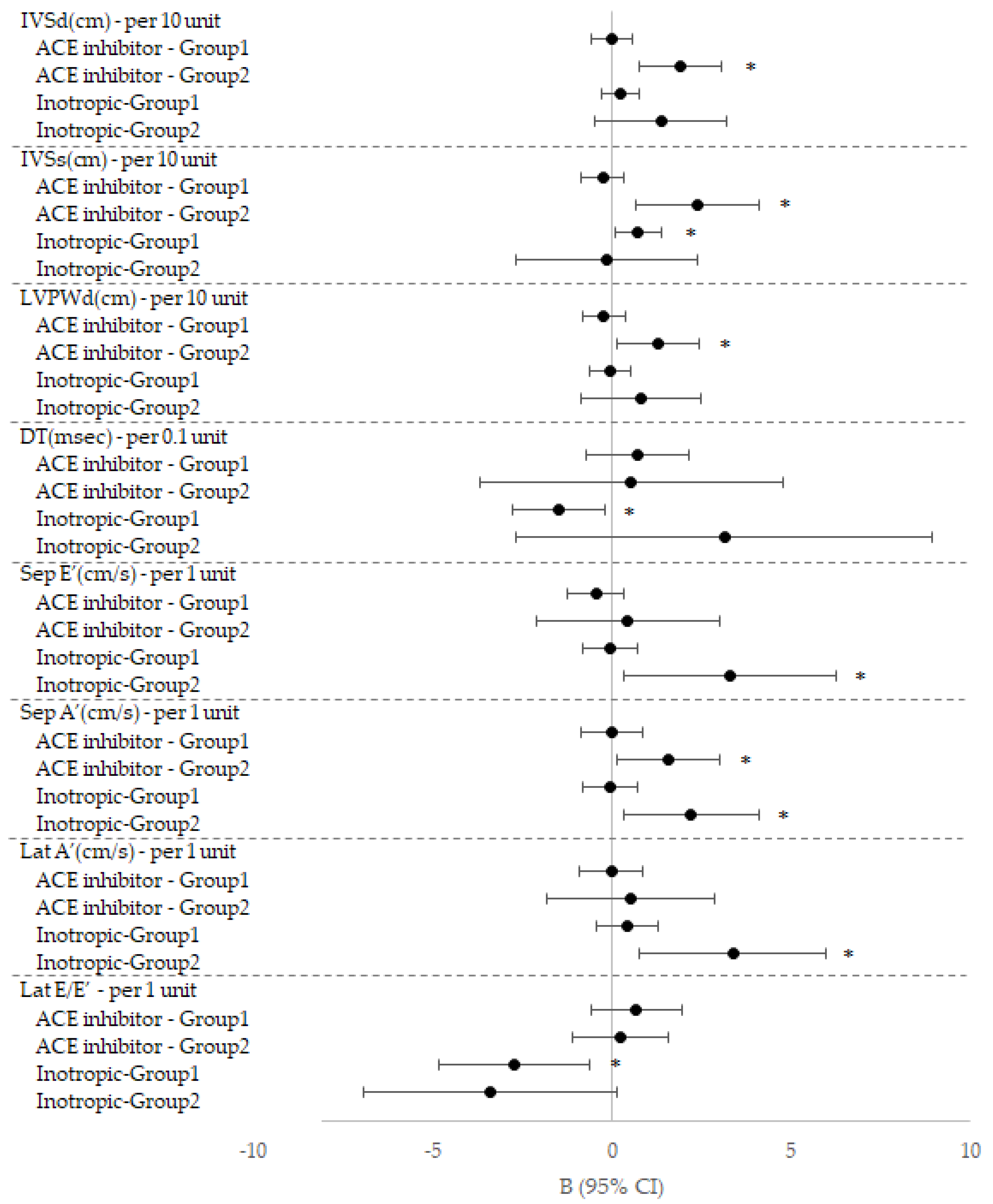
To compare the effect of treatment, we analyzed relationship between the change values of echocardiographic data and cardiac medication & respiratory care in each group (
Table 6). Taking ACE inhibitor in Group 2 was related to increase in IVSd, IVSs and LVPWd (
p < 0.05), and also related to decrease in Sep S’ and Lat E/E’ and increase in Sep A’ (
p < 0.05). Taking inotropic in Group 2 was related to increase in Sep E’ and Lat A’ (
p < 0.05). Taking inotropic agents in Group 1 was related to increase in IVSs and decrease in DT (
p < 0.05). The effect of these two medications, ACE inhibitor and inotropic agent in each group was demonstrated as a graph by Forest plot (
Figure 2). Taking beta-blocker in Group 2 was related to decrease in EDV, EF, SV and FS (
p < 0.05). Taking aspirin in Group 1 related to increase in IVSs and taking aspirin in Group 2 was related to decrease in SV (
p < 0.05). Taking diuretics in Group 2 was related to decrease in Sep E/E’ (
p < 0.05). Ventilator use in Group 2 was related to increase in mitral E (
p < 0.05) (
Table 6).
4. Discussion
DMD is an inherited X-linked disease with a 1/3000 male birth incidence. The disease follows a predictable clinical course marked by progressive skeletal muscle weakness. Death occurs in early adulthood secondary to respiratory or cardiac failure [
16]. Cardiac involvement begins as minor electrocardiographic abnormalities and evolves toward cardiomyopathy with dilatation of the cardiac chambers and depressed LV EF due to widespread fibrosis; it accounts for up to 40% of deaths [
17]. Cardiac management has been challenging because the New York Heart Association classification of heart failure relies on reduced exercise tolerance, a feature that in DMD arises from skeletal muscle and cardiac disease combined. In DMD children, the signs and symptoms of heart failure in the non-ambulatory individual are frequently subtle and overlooked. The patients with lower LV EF did not always demonstrate definite symptoms or signs of heart failure with chronic adjustment. Relatively, they had been in subtle difficulty with chest tightness, discomfort, or tachypnea. As DMD children might have been adjusted to their gradual progress of cardiac dysfunction, their clinical presentation of heart failure is probably masked or unusual compared with other patients with heart failure. Once or twice per year, they were regularly hospitalized for checking the spontaneous respiration or assisted ventilation with CO
2 status, in addition to cardiac functional evaluation by echocardiography. For the patients with EF < 50%, we added low dosage of oral inotropic agents by combination of dopamine with dobutamine for stabilizing the vital sign of blood pressure and heart rate for optimal circulation. Among the enrolled patients, nobody was related implantable cardioverter defibrillator (ICD) or pacemaker implantation. Perhaps a proactive strategy of early diagnosis and treatment for cardiomyopathy in DMD is essential to maximize duration and quality of life [
18].
In this study, we can notice that all the echocardiographic measurements demonstrated alteration over time even with or without statistical significances (
Table 2). Myocardial wall thickness of IVSd, IVSs and LVPWd became thinner, systolic functional measurement of EF and FS decreased with ongoing cardiac dysfunction in DMD patients with aging (
Table 2). We investigated to find the relation between cardiac medications and all the change values of echocardiographic parameters, and revealed the relationship (
Table 3). Interventricular septal thickness at diastole implies the relaxation status of the radial direction of myofibril from both left ventricle (LV) and right ventricle (RV). While heart failure proceeds in DMD cardiomyopathy, myocardial thinning might develop at the interventricular septum, then each free wall of LV and RV in order. As diuretic is one of the medical treatment regimens for heart failure, for ongoing heart failure status in DMD children, the initial treatment protocol should include diuretics, ACE inhibitor, and inotropic agents, which helped the myocardial protection. However, beta-blocker was not contributed to maintain cardiac function.
Moreover, we divided patients into two group based on EF which represents systolic function (
Table 4) [
19]. In Group 1, EF decreased by 3.615% annually, while in Group 2, EF decreased by 0.582% in similar respiratory assist situation (
p < 0.05). The difference should be elucidated why the lower LV EF group demonstrated better preservation of cardiac function. In
Table 5, it is noticeable that Group 2 patients take more numbers of medications (
p = 0.001), especially including inotropic agents for stabilizing their blood pressure and heart rate at 88.9% in Group 2 (
p = 0.0009).
It is well known that ACE inhibitor and beta-blocker are helpful for the treatment of heart failure. Furthermore, ACE inhibitor is recognized to decrease mortality in 10-year follow-up [
20]. Similarly, in our study, there was significant positive correlation between ACE inhibitor and the echocardiographic parameters (
Table 6). As
Figure 2 demonstrated, especially in Group 2, by taking ACE inhibitor, IVSs, IVSd and LVPWd were more preserved and improved systolic and diastolic myocardial function of the measurement of Sep S’, Lat E/E’. In addition, taking inotropic agents showed statistical significance within similar reasonable ranges of Sep E’, Lat A’, DT, Lat S’, which implied diastolic and systolic functional preservation. While ACE inhibitor helped to protect myocardial wall thickness from thinning, but, diminished myocardial wall movement, inotropic agents effected to enhance systolic myocardial wall velocities by tissue Doppler measurements (
Figure 1). Accordingly, ACE inhibitor with inotropic agents would benefit for cardiac functional preservation, especially in patients with lower LV EF.
In contrast, taking beta-blocker in Group 2 seemed to be associated deterioration of systolic function (EF, SV, EDV and FS). Based on this result, we could not expect favorable outcome with taking beta-blocker in patients with low EF. Despite, it is opposite result of conventional treatment, further research on this aspect should be necessary in the future.
LV EF is the most popular cardiac functional prognostic measurement in DMD; however, recent studies pointed out its low sensitivity to detect early cardiac involvement [
11]. In addition, it is not common to use inotropic agents in DMD children whose EF is maintained within normal range. Goudot et al. reported that DMD patients without the presence of inotropic reserve (defined as an increase in LV EF >10% during dobutamine infusion) showed more significant decline of LV EF than DMD patients with the presence of inotropic reserve (
p = 0.031 for difference in trend between groups). Moreover, they also reported an assessment of inotropic reserve may offer a sensitive approach for progression of cardiovascular disease in DMD children patients [
17]. Based on inotropic reserve, to investigate the effect of inotropics on cardiac function in DMD cardiomyopathy, would be helpful to provide a better guideline for the treatment of DMD children. In this study, various medical treatment including inotropic agents revealed to benefit, not only for the stable blood pressure and heart rate, but also for preservation of myocardial function with ongoing heart failure in DMD children’s cardiomyopathy. Inotropic agents demonstrated to help to augmentation of Sep E’, Sep A’ and Lat S’ velocities in patients with LV EF < 45% (
Table 5), which implied to sustain myocardial velocities.
The limitation of this study is that this is a single-center retrospective study and the numbers of patients was relatively small due to DMD disease’s rarity. We did not investigate the steroid treatment in this study [
21]. The eplerenone, a new medication which is reported mineralocorticoid receptor antagonists in heart failure with preserved ejection fraction (HFpEF), we should investigate the effect for the DMD cardiomyopathy in the future [
8].
Observation for the relationship between medications and echocardiographic parameters in this study was relatively short-term follow up for complete explanation. Further long-term research should be preceded for the fruitful results.





{kind=link}
{kind=link}