Time-Dependent Anti-Demineralization Effect of Silver Diamine Fluoride

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
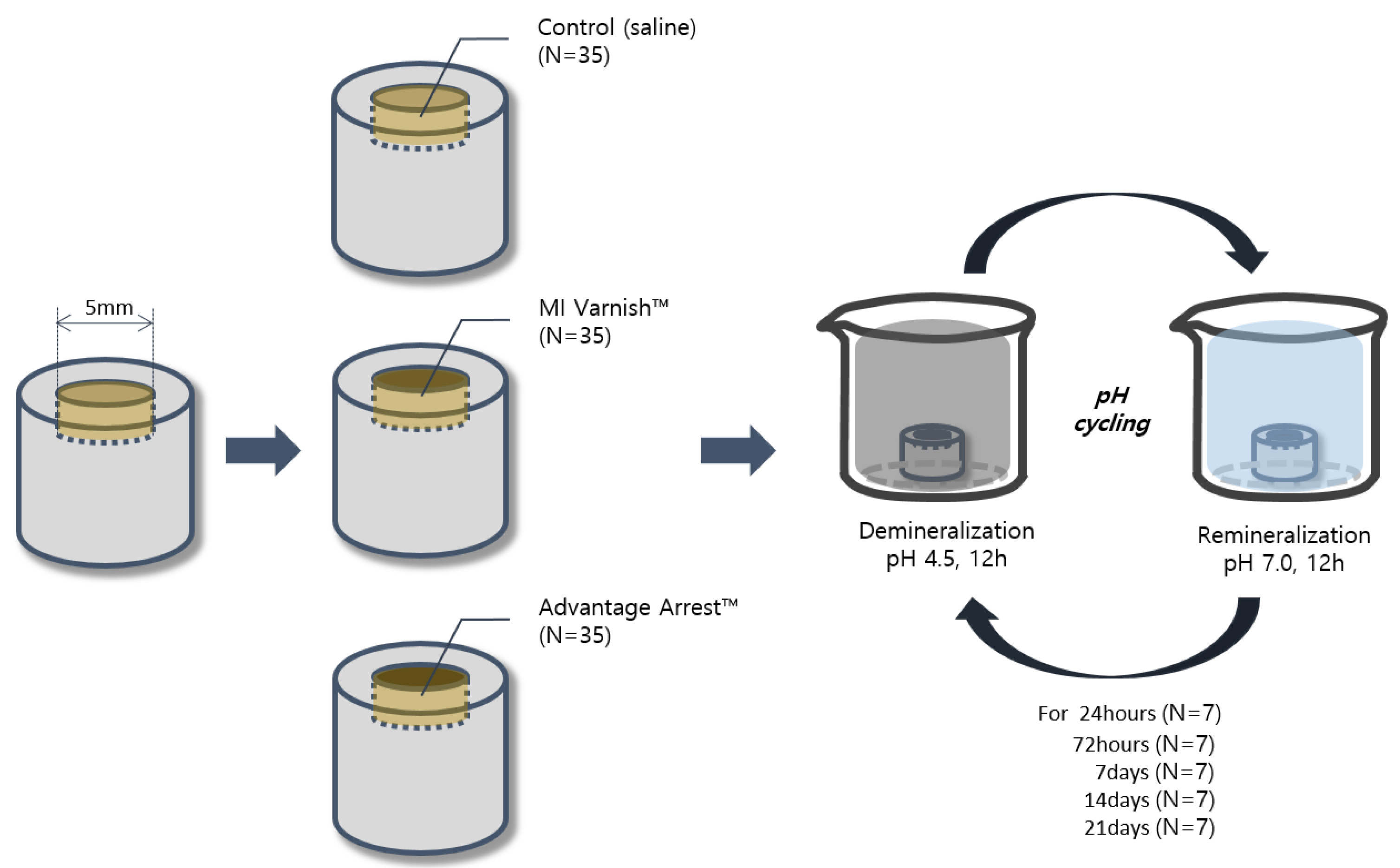
2.1. Specimen Preparation and Classification
2.2. Agent Application and PH Cycling
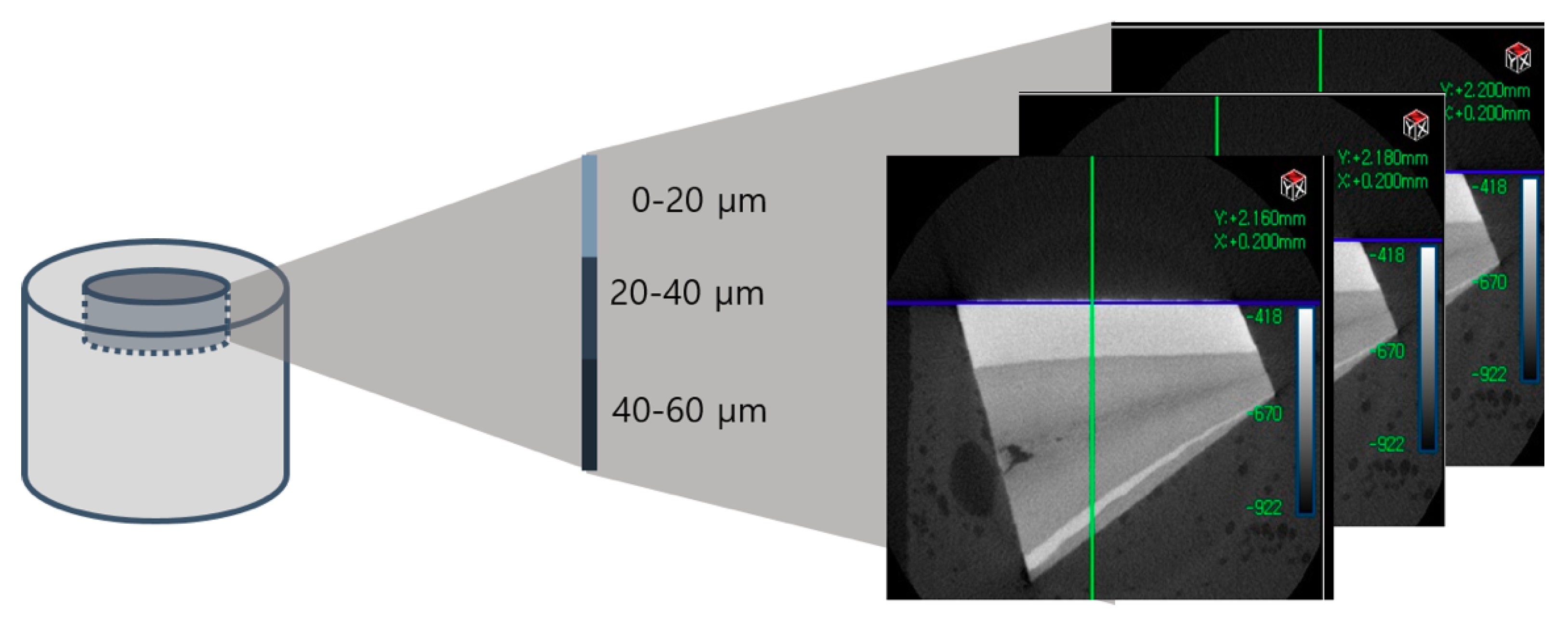
2.3. Micro-Computed Tomography Analysis
2.3.1. Changes in Surface Density
2.3.2. Changes in Density by Enamel Depth
2.3.3. Changes in Enamel Volume
2.4. Enamel Surface Analysis Using Scanning Electron Microscopy
2.5. Statistical Analysis
3. Results
3.1. Density and Volume Analysis with Micro-CT
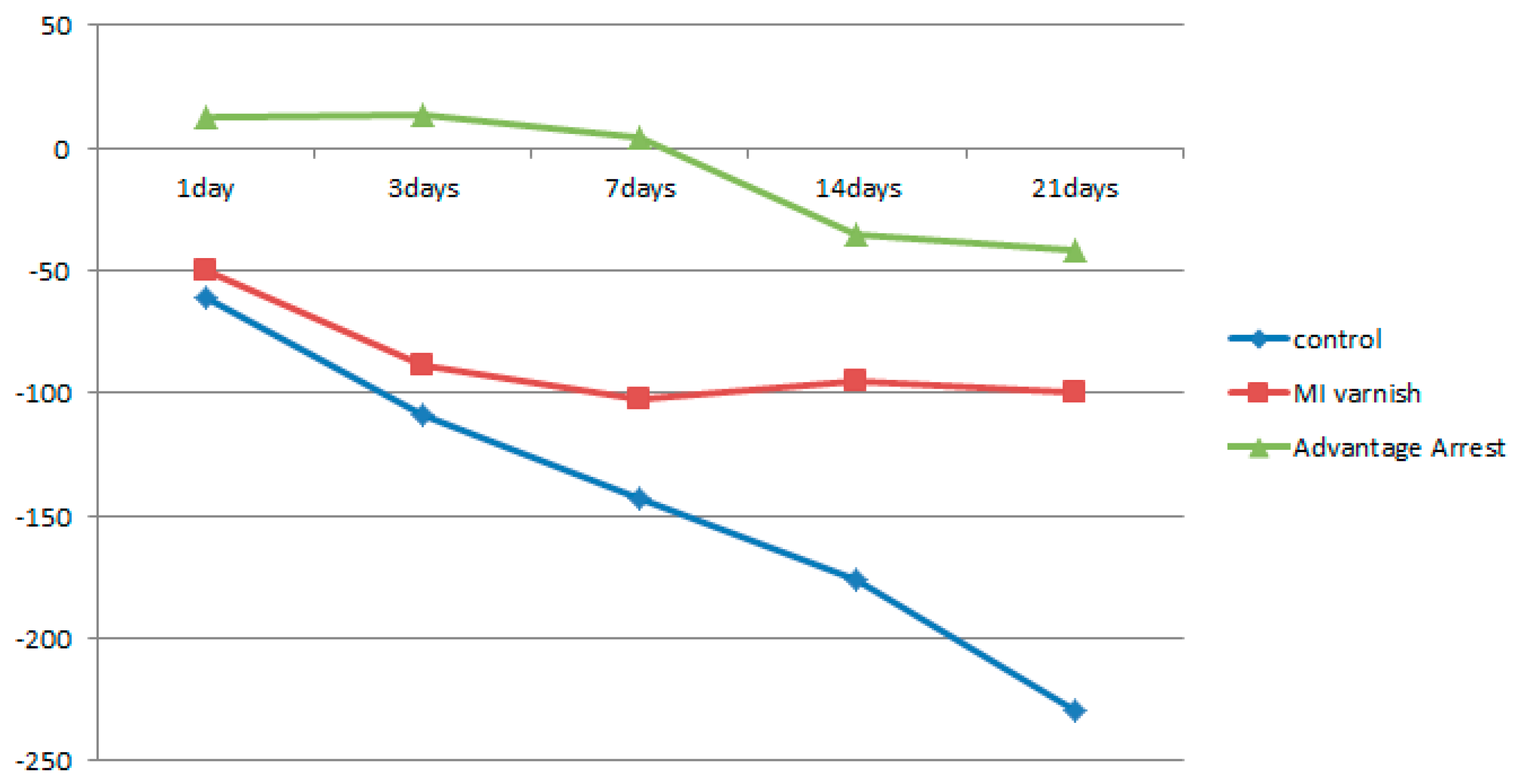
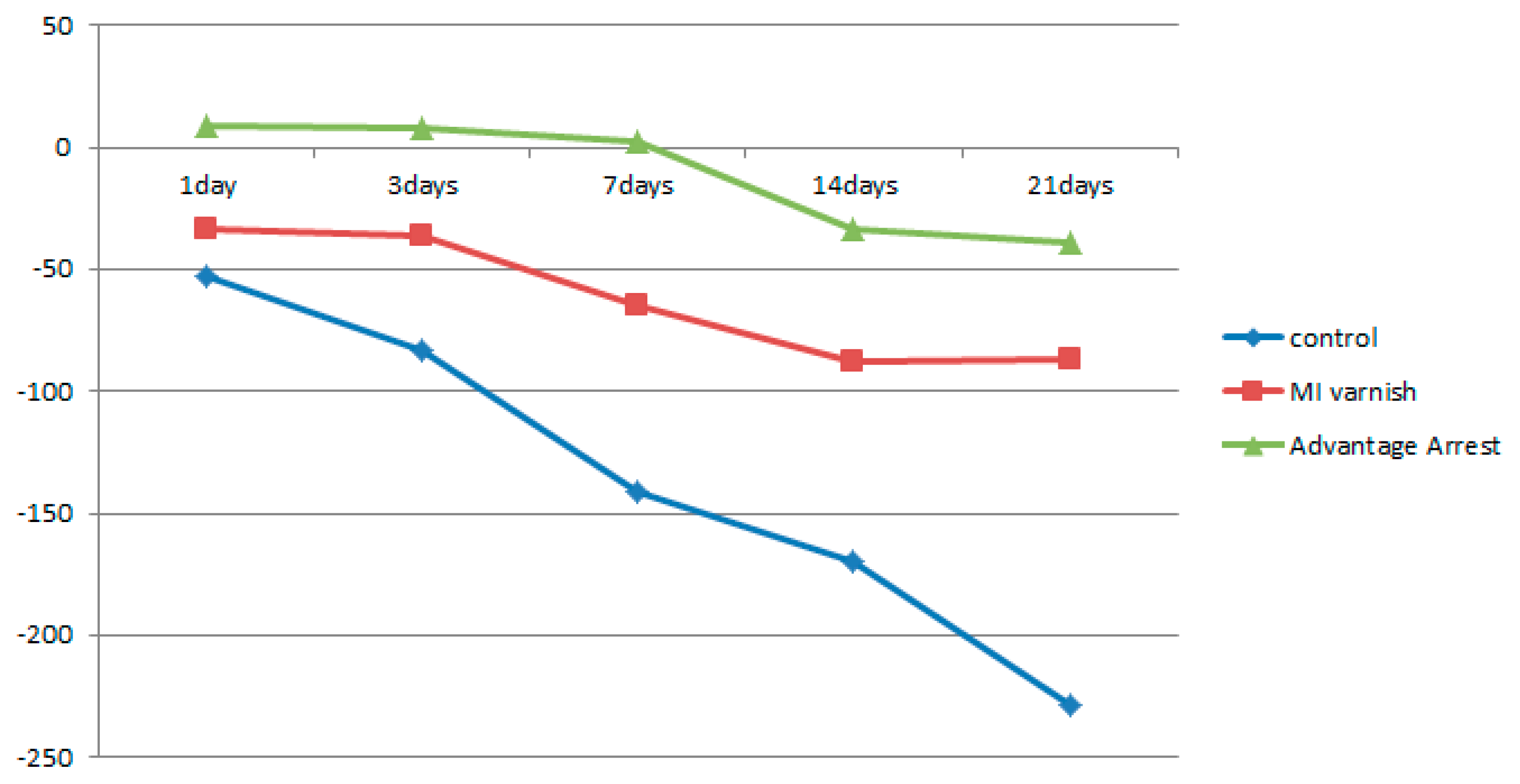
3.1.1. Comparison of Surface Density Variation
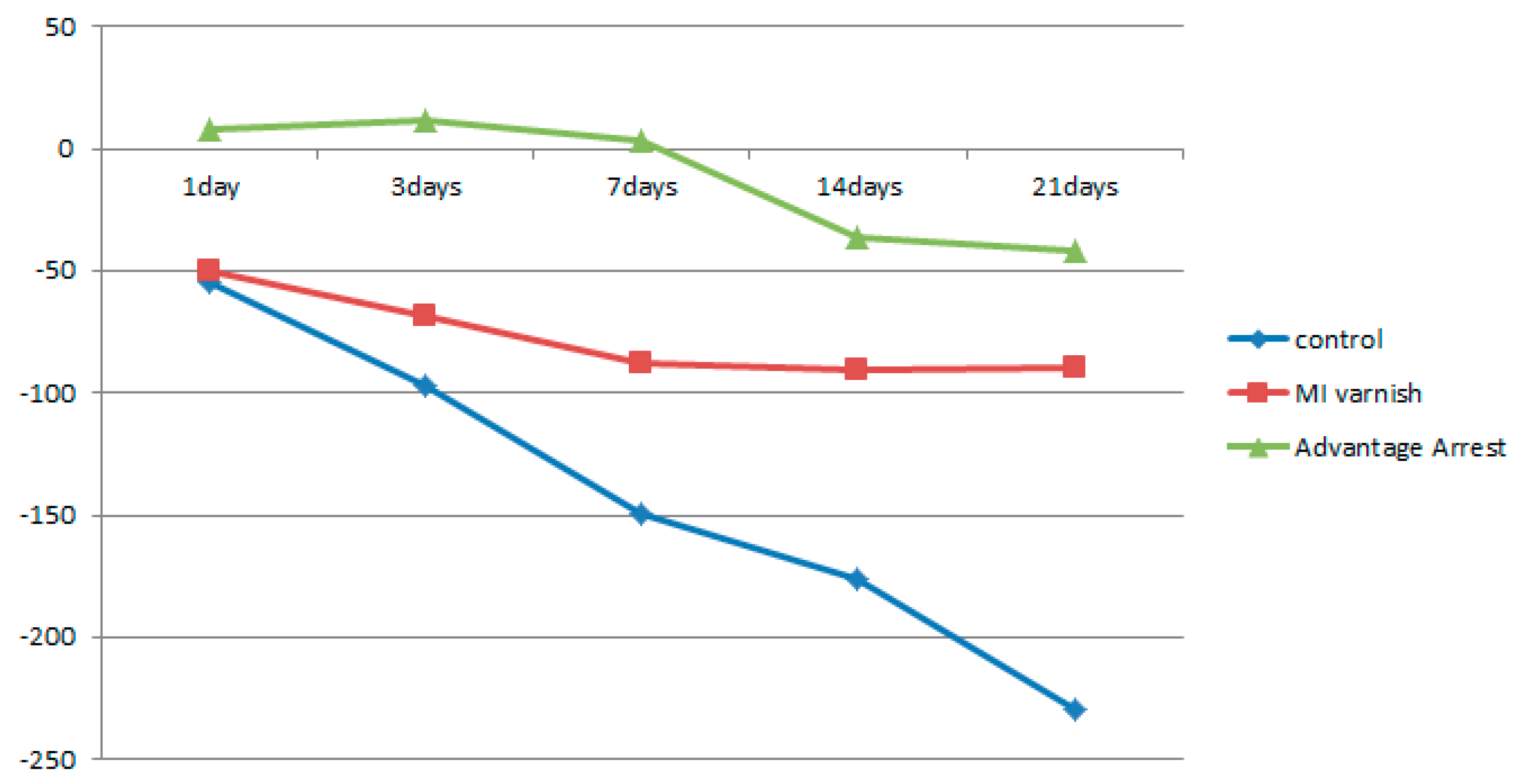
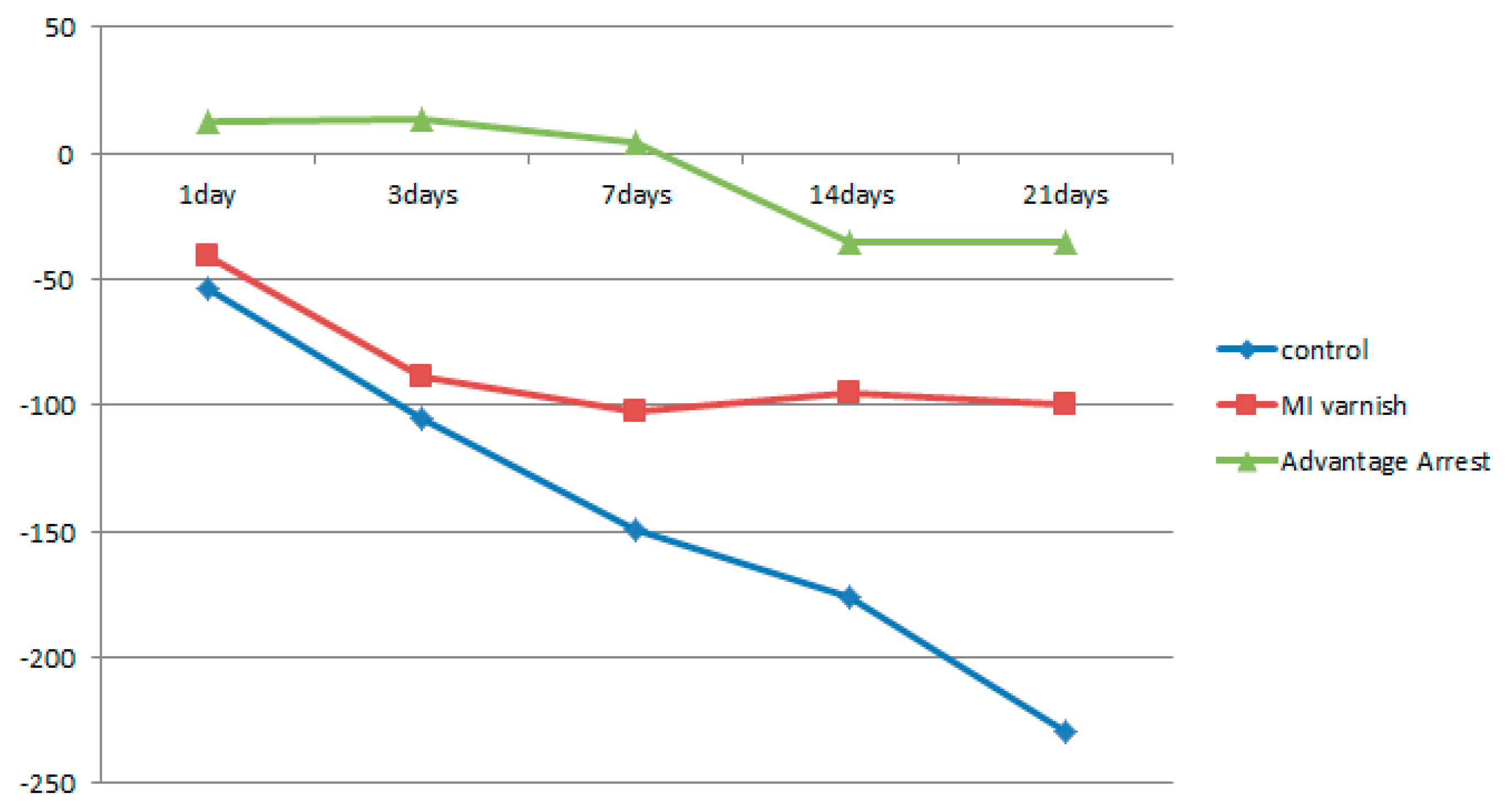
3.1.2. Comparison of Density Variation by Enamel Depth
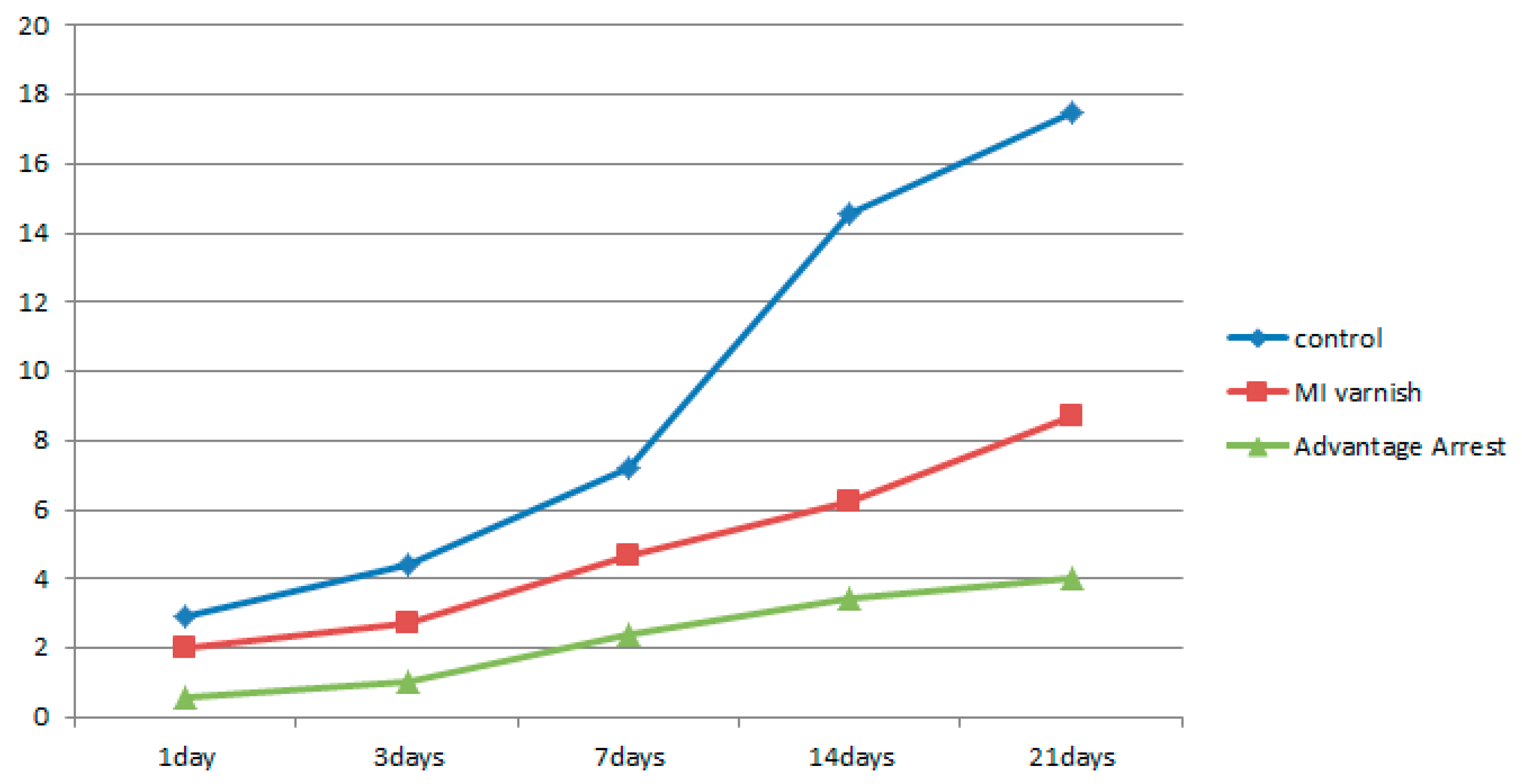
3.1.3. Comparison of Volume Change in the Demineralized Enamel
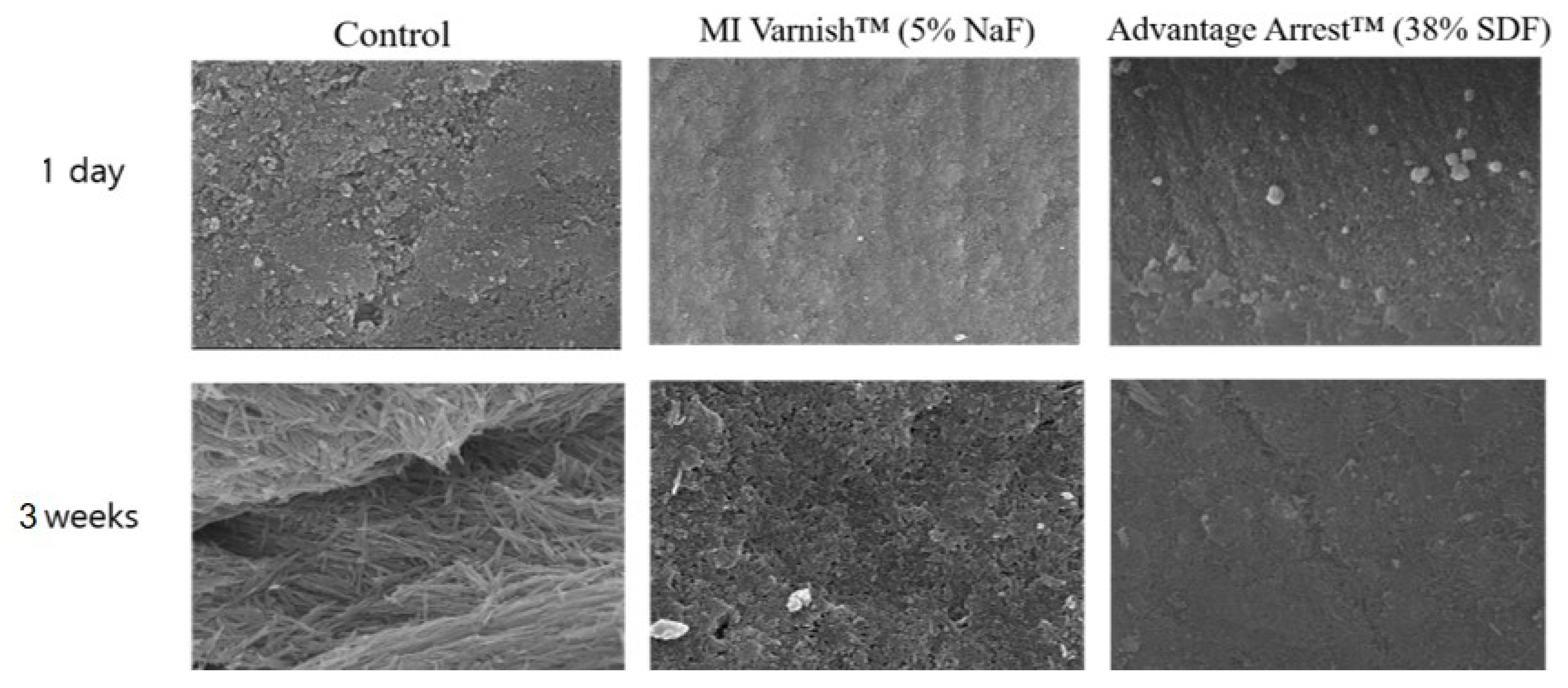
3.2. Analysis of Enamel Surface Using Scanning Electron Microscope
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 25, 3. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. Oral Health in America: A Repot of the Surgeon General; U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research: Rockville, MD, USA; National Institutes of Health: Bethesda, MD, USA, 2000. [Google Scholar]
- Cho, O.S.; Park, D.Y.; Choi, Y.H.; Lee, B.J.; Son, C.K. Korean Children’s Oral Health Survey; Korea Health Promotio Institute: Sejong, Korea, 2015; p. 132. [Google Scholar]
- Lecompte, E.J. Clinical Application of Topical Fluoride Products-Risks, Benefits, and Recommendations. J. Dent. Res. 1987, 66, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, C.B.; Donly, K.J.; Wefel, J.S.; Jakobsen, J.R.; Denehy, G.E. An in vitro Comparison of Three Fluoride Regimens on Enamel Remineralization. Caries Res. 1997, 31, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Marinho, V.C.; Higgins, J.P.; Logan, S.; Sheiham, A. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2002, 3. [Google Scholar] [CrossRef]
- Helfenstein, U.; Steiner, M. Fluoride varnishes (Duraphat): A meta-analysis. Community Dent. Oral Epidemiol. 1994, 22, 1–5. [Google Scholar] [CrossRef]
- Lam, A.; Chu, C.H. Caries Management with Fluoride Varnish of Children in US. N. Y. State Dent. J. 2011, 77, 38–42. [Google Scholar] [PubMed]
- Chu, C.H.; Lo, E.C.M. Promoting Caries Arrest in Children with Silver Diamine Fluoride: A Review. Oral Health Prev. Dent. 2008, 6, 315–321. [Google Scholar]
- Peng, J.J.-Y.; Botelho, M.G.; Matinlinna, J.P. Silver compounds used in dentistry for caries management: A review. J. Dent. 2012, 40, 531–541. [Google Scholar] [CrossRef]
- Mei, M.L.; Lo, E.C.M.; Chu, C.H. Clinical Use of Silver Diamine Fluoride in Dental Treatment. Compend. Contin. Educ. Dent. 2016, 37, 93–98. [Google Scholar]
- Yamaga, R.; Yokomizo, I. Arrestment of caries of deciduous teeth with diamine silver fluoride. Dental Outlook 1969, 33, 1007–1013. [Google Scholar]
- Horst, J.A.; Ellenikiotis, H.; Milgrom, P.L. UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride: Rationale, Indications and Consent. J. Calif. Dent. Assoc. 2016, 44, 16–28. [Google Scholar] [PubMed]
- Chu, C.H.; Mei, L.; Seneviratne, C.J.; Lo, E.C.M. Effects of silver diamine fluoride on dentine carious lesions induced by Streptococcus mutans and Actinomyces naeslundii biofilms. Int. J. Paediatr. Dent. 2012, 22, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.Y.; Lo, E.C.M.; Li, C.M. Effect of silver and fluoride ions on enamel demineralization: A quantitative study using micro-computed tomography. Aust. Dent. J. 2012, 57, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Li, Q.L.; Chu, C.H.; Yiu, C.K.Y.; Lo, E.C.M. The inhibitory effects of silver diamine fluoride at different concentrations on matrix metalloproteinases. Dent. Mater. 2012, 28, 903–908. [Google Scholar] [CrossRef]
- Lo, E.C.; Chu, C.H.; Lin, H.C. A community-based caries control program for pre-school children using topical fluorides: 18-month results. J. Dent. Res. 2001, 80, 2071–2074. [Google Scholar] [CrossRef]
- Li, Y.J. Effect of al silver ammonia fluoride solution on the prevention and inhibition of caries. Zhonghua Kou Qiang Ke Za Zhi. 1984, 19, 97–100. [Google Scholar]
- Delbem, A.C.B.; Bergamaschi, M.; Sassaki, K.T.; Cunha, R.F. Effect of fluoridated varnish and silver diamine fluoride solution on enamel demineralization: pH-cycling study. J. Appl. Oral Sci. 2006, 14, 88–92. [Google Scholar] [CrossRef] [Green Version]
- Luedemann, T.N.R.C. Micro-Computed Tomography in Caries Research. Master’s Thesis, LMU Munchen Medizinische Fakultat, Munich, Germany, 2007. [Google Scholar]
- Ten Cate, J.M.; Duijsters, P.P. Alternating demineralization and remineralization of artificial enamel lesions. Caries Res. 1982, 16, 201–210. [Google Scholar] [CrossRef]
- Sayed, M.; Matsui, N.; Hiraishi, N.; Inoue, G.; Nikaido, T.; Burrow, M.F.; Tagami, J. Evaluation of discoloration of sound/demineralized root dentin with silver diamine fluoride: In-vitro study. Dent. Mater. J. 2019, 38, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Mei, M.L.; Chu, C.H.; Lo, E.C.M.; Samaranayake, L.P. Fluoride and silver concentrations of silver diamine fluoride solutions for dental use. Int. J. Paediatr. Dent. 2013, 23, 279–285. [Google Scholar] [CrossRef]
- Yamage, R.; Nishino, M.; Yoshida, S.; Yokomizo, I. Diammine silver fluoride and its clinical application. J. Osaka Univ. Dent. Sch. 1972, 12, 1–20. [Google Scholar]
- Fung, M.H.T.; Wong, M.C.M.; Lo, E.C.M.; Chu, C.H. Arresting Early Childhood Caries with Silver Diamine Fluoride-A Literature Review. J. Oral. Hyg. Health 2013, 1, 117. [Google Scholar]
- Cury, J.A.; Tenuta, L.M.A. Enamel remineralization: Controlling the caries disease or treating early caries lesion? Braz. Oral. Res. 2009, 23, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, I.S.; Gao, S.S.; Hiraishi, N.; Burrow, M.F.; Duangthip, D.; Mei, M.L.; Lo, E.C.M.; Chu, C.H. Mechanisms of silver diamine fluoride on arresting caries: A literature review. Int. Dent. J. 2018, 68, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duperon, D.F. Early childhood caries: A continuing dilemma. J. Calif. Dent. Assoc. 1995, 23, 15–16. [Google Scholar] [PubMed]
- Mei, M.L.; Li, Q.L.; Chu, C.H.; Lo, E.C.M.; Samaranayake, L.P. Antibacterial effects of silver diamine fluoride on multi-species cariogenic biofilm on caries. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsumi, N. Studies on topical application of Ag(NH3)2F for the control of interproximal caries in human primary molars. 2. effect of Ag(NH3)2F on Streptococcus mutans on interproximal plaque. Jpn. J. Paediatr. Dent. 1981, 19, 523–536. [Google Scholar]
- Knight, G.M.; Mclntyre, J.M.; Craig, G.G.; Dalidjan, M.; Zilm, P.S.; Gully, N.J. An in vitro model to measure the effect of a silver fluoride and potassium iodide treatment on the permeability of demineralized dentine to Streptococcus mutans. Aust. Dent. J. 2005, 50, 242–245. [Google Scholar] [CrossRef]
- Ling, L.I.; Sizhen, S.H.I. Comparison of the remineralizations of three preparations on deciduous enamel. Shanghai Med. J. 2001, 24, 29–31. [Google Scholar]
- Wu, L.; Yang, F. The effects of three fluoride-containing agents on the remineralization of deciduous teeth in vitro. J. Pract. Stomatol. 2002, 18, 347–349. [Google Scholar]
- Wu, L.; Yang, F. Comparison of the effects of three fluoride-containing agents on the demineralization of deciduous teeth in vitro. J. Mod. Stomatol. 2002, 16, 216–218. [Google Scholar]
- Kim, S.Y.; Lee, S.H.; Lee, N.Y.; Jih, M.K. Effect of Silver Diamine Fluoride and Sodium Fluoride Varnish on Remineralization in Artificially Induced Enamel Caries: An in vitro Study. J. Korean Acad. Pediatr. Dent. 2020, 47, 266–276. [Google Scholar] [CrossRef]
- Chu, C.H.; Lo, E.C.M.; Lin, H.C. Effectiveness of Silver Diamine Fluoride and Sodium Fluoride Varnish in Arresting Dentin Caries in Chinese Pre-school Children. J. Dent. Res. 2002, 81, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Llodra, J.C.; Rodriguez, A.; Ferrer, B.; Menardia, V.; Ramos, T.; Morato, M. Efficacy of Silver Diamine Fluoride for Caries Reduction in Primary Teeth and First Permanent Molars of Schoolchildren: 36-month Clinical Trial. J. Dent. Res. 2005, 84, 721–724. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.Y.; Lo, E.C.M.; Chu, C.H.; Lin, H.C. Randomized Trial on Fluorides and Sealants for Fissure Caries Prevention. J. Dent. Res. 2012, 91, 753–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamama, H.H.; Yiu, C.K.; Burrow, M.F. Effect of silver diamine fluoride and potassium iodide on residual bacteria in dentinal tubules. Aust. Dent. J. 2015, 60, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, V.E.; Vasconcelos Filho, A.; Targino, A.G.R.; Flores, M.A.P.; Galembeck, A.; Franca Caldas, A.; Rosenblatt, A. A New “Silver-Bullet” to treat caries in children—Nano Silver Fluoride: A randomised clinical trial. J. Dent. 2014, 42, 945–951. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, R.B.; Haiter-Neto, F.; Carlo, H.L.; Soares, C.J.; Sinhoreti, M.A.C.; Puppin-Rontani, R.M.; Correr-Sobrinho, L. Radiodensity and hardness of enamel and dentin of human and bovine teeth, varying bovine teeth age. Arch. Oral Biol. 2008, 53, 1023–1029. [Google Scholar] [CrossRef]
- Donassollo, T.A.; Romano, A.R.; Demarco, F.F. Evaluation of the surface microhardness of the enamel and dentin of bovine and human teeth (permanent and deciduous). Dent Sci. J. 2007, 22, 311–316. [Google Scholar]
- Ghisi, A.C.; Kopper, P.M.; Baldasso, F.E.; Sturmer, C.P.; Rossi-Fedele, G.; Steier, L.; de Figueiredo, J.A.; Morgental, R.D.; Vier-Pelisser, F.V. Effect of superoxidized water and sodium hypochlorite, associated or not with EDTA, on organic and inorganic components of bovine root dentin. J. Endod. 2015, 41, 925–930. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Brand Name | Composition |
|---|---|---|
| Control (saline) | Daihan Pharm Co. Ltd., Seoul, Korea | Sodium Chloride |
| MI VarnishTM | GC Corp., Tokyo, Japan | 5% Sodium Fluoride |
| Advantage ArrestTM | Elevate Oral Care, West Palm Beach, FL, USA | 38% Silver Diamine Fluoride |
| Group | Materials | Time Progression (pH Cycling Periods) | N |
|---|---|---|---|
| 1 | Control (saline) | 1 days | 7 |
| 2 | 3 days | 7 | |
| 3 | 7 days | 7 | |
| 4 | 14 days | 7 | |
| 5 | 21 days | 7 | |
| 6 | MI VarnishTM | 1 days | 7 |
| 7 | 3 days | 7 | |
| 8 | 7 days | 7 | |
| 9 | 14 days | 7 | |
| 10 | 21 days | 7 | |
| 11 | Advantage ArrestTM | 1 days | 7 |
| 12 | 3 days | 7 | |
| 13 | 7 days | 7 | |
| 14 | 14 days | 7 | |
| 15 | 21 days | 7 |
| Control (Saline) | MI VarnishTM | Advantage ArrestTM | |
|---|---|---|---|
| 1 day | −53.980 ± 20.800 | −40.874 ± 9.832 | 12.534 ± 11.331 |
| 3 days | −105.388 ± 18.074 | −88.800 ± 21.848 | 13.130 ± 2.441 |
| 7 days | −149.798 ± 18.966 | −102.284 ± 9.999 | 4.696 ± 1.506 |
| 14 days | −175.902 ± 24.960 | −94.636 ± 9.050 | 4.696 ± 1.506 |
| 21 days | −229.452 ± 17.225 | −99.706 ± 4.099 | −35.678 ± 11.073 |
| Materials | Control (Saline) | MI VarnishTM | Advantage ArrestTM |
|---|---|---|---|
| 1 day | −61.484 ± 5.856 | −57.224 ± 7.070 | 11.668 ± 15.623 |
| 3 days | −108.892 ± 9.829 | −88.796 ± 21.846 | 13.130 ± 2.114 |
| 7 days | −149.798 ± 18.966 | −102.280 ± 9.993 | 4.696 ± 1.506 |
| 14 days | −175.902 ± 24.960 | −94.636 ± 9.050 | −35.678 ± 11.073 |
| 21 days | −229.454 ± 17.223 | −99.706 ± 4.099 | −41.342 ± 3.155 |
| Materials | Control (Saline) | MI VarnishTM | Advantage ArrestTM |
|---|---|---|---|
| 1 day | −54.374 ± 7.008 | −50.228 ± 15.445 | 8.388 ± 7.166 |
| 3 days | −96.662 ± 8.420 | −68.856 ± 13.090 | 11.232 ± 5.869 |
| 7 days | −149.282 ± 15.681 | −88.064 ± 6.272 | 2.994 ± 1.696 |
| 14 days | −176.304 ± 28.169 | −90.236 ± 10.379 | −36.436 ± 4.327 |
| 21 days | −229.332 ± 22.719 | −89.432 ± 11.396 | −41.544 ± 9.066 |
| Materials | Control (Saline) | MI VarnishTM | Advantage ArrestTM |
|---|---|---|---|
| 1 day | −53.096 ± 14.884 | −33.686 ± 7.534 | 9.170 ± 9.832 |
| 3 days | −82.746 ± 18.518 | −35.778 ± 2.706 | 7.760 ± 5.089 |
| 7 days | −140.966 ± 5.693 | −64.384 ± 2.089 | 2.414 ± 0.256 |
| 14 days | −170.016 ± 33.814 | −87.360 ± 11.585 | −33.072 ± 6.789 |
| 21 days | −228.406 ± 39.752 | −87.030 ± 11.233 | −39.310 ± 10.056 |
| Materials | Control (mm3) | MI VarnishTM (mm3) | Advantage ArrestTM (mm3) |
|---|---|---|---|
| 1 day | 2.940 ± 0.520 | 1.992 ± 0.564 | 0.588 ± 0.245 |
| 3 days | 4.394 ± 0.735 | 2.710 ± 0.635 | 1.020 ± 0.291 |
| 7 days | 7.234 ± 2.193 | 4.684 ± 0.946 | 2.404 ± 0.467 |
| 14 days | 14.554 ± 1.650 | 6.258 ± 1.340 | 3.432 ± 0.996 |
| 21 days | 17.504 ± 0.869 | 8.672 ± 1.572 | 4.008 ± 1.377 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, J.-H.; Kim, J.-W.; Yoon, Y.-M.; Lee, N.-Y.; Lee, S.-H.; Jih, M.-K. Time-Dependent Anti-Demineralization Effect of Silver Diamine Fluoride. Children 2020, 7, 251. https://doi.org/10.3390/children7120251
Ahn J-H, Kim J-W, Yoon Y-M, Lee N-Y, Lee S-H, Jih M-K. Time-Dependent Anti-Demineralization Effect of Silver Diamine Fluoride. Children. 2020; 7(12):251. https://doi.org/10.3390/children7120251
Chicago/Turabian StyleAhn, Ji-Hye, Ji-Woong Kim, Young-Mi Yoon, Nan-Young Lee, Sang-Ho Lee, and Myeong-Kwan Jih. 2020. "Time-Dependent Anti-Demineralization Effect of Silver Diamine Fluoride" Children 7, no. 12: 251. https://doi.org/10.3390/children7120251
APA StyleAhn, J.-H., Kim, J.-W., Yoon, Y.-M., Lee, N.-Y., Lee, S.-H., & Jih, M.-K. (2020). Time-Dependent Anti-Demineralization Effect of Silver Diamine Fluoride. Children, 7(12), 251. https://doi.org/10.3390/children7120251