Discharging Preterm Infants Home on Caffeine, a Single Center Experience

Abstract
:1. Introduction
2. Materials and Methods
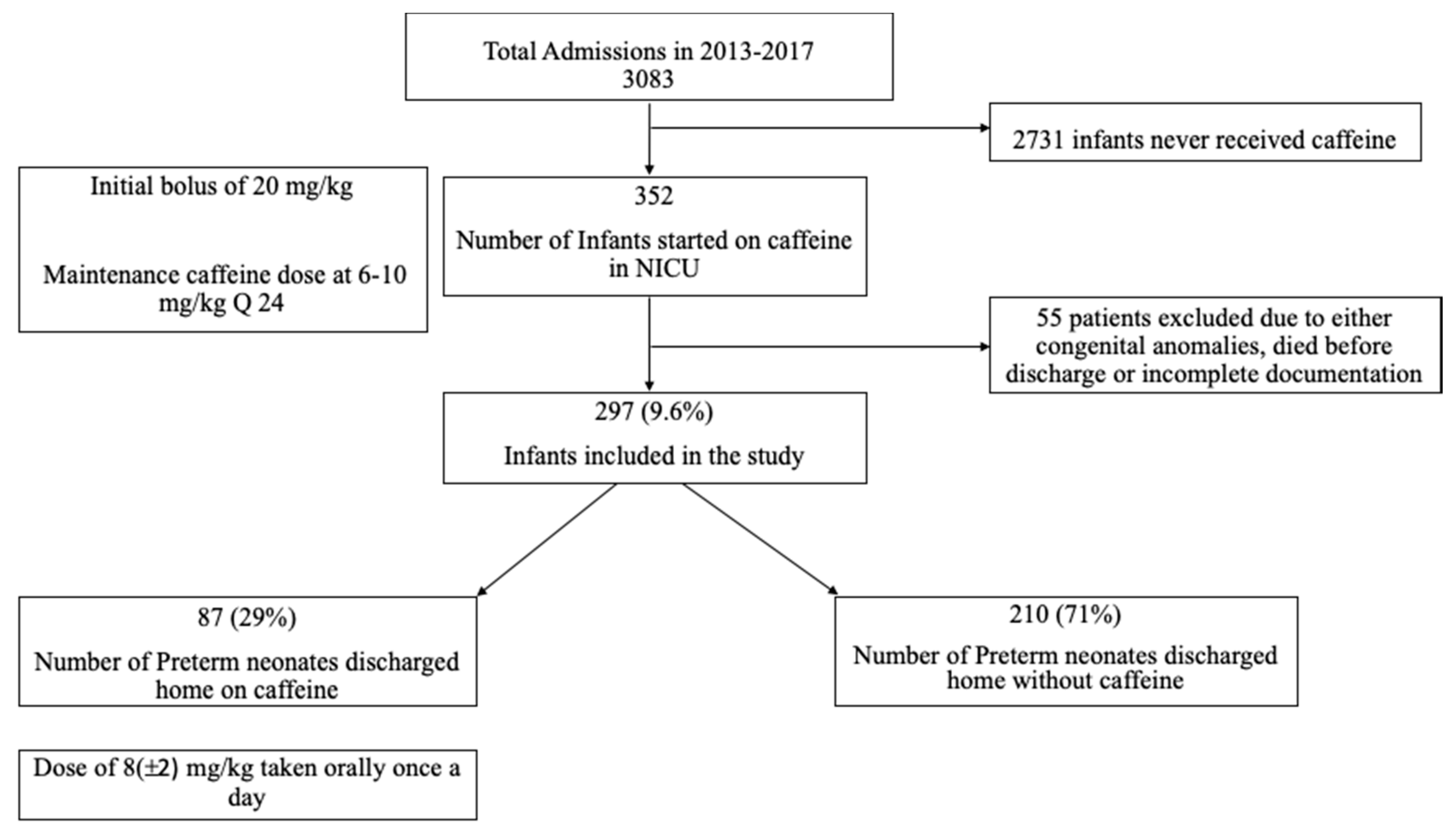
2.1. Study Population Selection
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AOP | Apnea of prematurity |
| LOS | Length of stay |
| NICU | Neonatal intensive care unit |
| CR | Cardiorespiratory monitoring |
| EPCH | El Paso Children’s Hospital |
| BRUE | Brief resolved unexplained event |
| ED | Emergency department |
| BPD | Bronchopulmonary Dysplasia |
| AGE | Acute Gastroenteritis |
| IH | Intermittent Hypoxemic Events |
| ASQ | Ages and Stages Questionnaire 3rd edition |
References
- Eichenwald, E.C. Apnea of Prematurity. Pediatrics 2016, 137, e20153757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrington, K.; Finer, N. The natural history of the appearance of apnea of prematurity. Pediatr Res. 1991, 29, 372–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.; Driscoll, A.K.; Mathews, T.J. Births: Final Data for 2015. National vital statistics reports: From the Centers for Disease Control and Prevention, National Center for Health Statistics. Natl. Vital Stat. Syst. 2017, 66, 1. [Google Scholar]
- Eichenwald, E.C.; Aina, A.; Stark, A.R. Apnea frequently persists beyond term gestation in infants delivered at 24 to 28 weeks. Pediatrics 1997, 100, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Gonzalez, F.; Mu, D. Apnea of prematurity: From cause to treatment. Eur. J. Pediatrics 2011, 170, 1097–1105. [Google Scholar] [CrossRef] [Green Version]
- Ramanathan, R.; Corwin, M.J.; Hunt, C.E.; Lister, G.; Tinsley, L.R.; Baird, T.; Silvestri, J.M.; Crowell, D.H.; Hufford, D.; Martin, R.J.; et al. Cardiorespiratory events recorded on home monitors: Comparison of healthy infants with those at increased risk for, SIDS. JAMA 2001, 285, 2199–2207. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, B.; Roberts, R.S.; Davis, P.; Doyle, L.W.; Barrington, K.J.; Ohlsson, A.; Solimano, A.; Tin, W. Caffeine therapy for apnea of prematurity. N. Engl. J. Med. 2006, 354, 2112–2121. [Google Scholar] [CrossRef] [Green Version]
- Dukhovny, D.; Lorch, S.A.; Schmidt, B.; Doyle, L.W.; Kok, J.H.; Roberts, R.S.; Kamholz, K.L.; Wang, N.; Mao, W.; Zupancic, J.A.; et al. Economic evaluation of caffeine for apnea of prematurity. Pediatrics 2011, 127, e146–e155. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Hady, H.; Nasef, N.; Shabaan, A.E.; Nour, I. Caffeine therapy in preterm infants. World J. Clin. Pediatrics 2015, 4, 81–93. [Google Scholar] [CrossRef]
- Dobson, N.R.; Rhein, L.M.; Darnall, R.A.; Corwin, M.J.; Heeren, T.C.; Eichenwald, E.; James, L.P.; McEntire, B.L.; Hunt, C.E. Caffeine decreases intermittent hypoxia in preterm infants nearing term-equivalent age. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2017, 37, 1135–1140. [Google Scholar] [CrossRef]
- Darnall, R.A.; Kattwinkel, J.; Nattie, C.; Robinson, M. Margin of safety for discharge after apnea in preterm infants. Pediatrics 1997, 100, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Martin, R. Management of Apnea of Prematurity. 2018. Available online: https://www.uptodate.com/contents/management-of-apnea-of-prematurity (accessed on 20 August 2020).
- Jefferies, A.L. Going home: Facilitating discharge of the preterm infant. Paediatr. Child Health 2014, 19, 31–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekharan, P.; Rawat, M.; Reynolds, A.M.; Phillips, K.; Lakshminrusimha, S. Apnea, bradycardia and desaturation spells in premature infants: Impact of a protocol for the duration of ‘spell-free’ observation on interprovider variability and readmission rates. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2018, 38, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Tieder, J.S.; Bonkowsky, J.L.; Etzel, R.A.; Franklin, W.H.; Gremse, D.A.; Herman, B.; Katz, E.S.; Krilov, L.R.; Merritt, J.L.; Norlin, C.; et al. Clinical Practice Guideline: Brief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk Infants: Executive Summary. Pediatrics 2016, 137, e20160591. [Google Scholar] [CrossRef] [Green Version]
- Ehrenkranz, R.A.; Walsh, M.C.; Vohr, B.R.; Jobe, A.H.; Wright, L.L.; Fanaroff, A.A.; Wrage, L.A.; Poole, K. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics 2005, 116, 1353–1360. [Google Scholar] [CrossRef] [Green Version]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Murphy, S.L.; Mathews, T.J.; Martin, J.A.; Minkovitz, C.S.; Strobino, D.M. Annual Summary of Vital Statistics: 2013–2014. Pediatrics 2017, 139, e20163239. [Google Scholar] [CrossRef] [Green Version]
- Russell, R.B.; Green, N.S.; Steiner, C.A.; Meikle, S.; Howse, J.L.; Poschman, K.; Dias, T.; Potetz, L.; Davidoff, M.J.; Damus, K.; et al. Cost of hospitalization for preterm and low birth weight infants in the United States. Pediatrics 2007, 120, e1–e9. [Google Scholar] [CrossRef] [Green Version]
- Muraskas, J.; Parsi, K. The Cost of Saving the Tiniest Lives: NICUs versus Prevention. Virtual Mentor VM 2008, 10, 655–658. [Google Scholar]
- Rogowski, J. Measuring the cost of neonatal and perinatal care. Pediatrics 1999, 103 (Suppl. 1E), 329–335. [Google Scholar]
- Rhein, L.M.; Dobson, N.R.; Darnall, R.A.; Corwin, M.J.; Heeren, T.C.; Poets, C.F.; McEntire, B.L.; Hunt, C.E.; Bada, H.; Carlo, W.; et al. Effects of caffeine on intermittent hypoxia in infants born prematurely: A randomized clinical trial. JAMA Pediatrics 2014, 168, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Dobson, N.R.; Hunt, C.E. Caffeine: An evidence-based success story in VLBW pharmacotherapy. Pediatric Res. 2018, 84, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Fiore, J.M.; Bloom, J.N.; Orge, F.; Schutt, A.; Schluchter, M.; Cheruvu, V.K.; Walsh, M.; Finer, N.; Martin, R.J. A higher incidence of intermittent hypoxemic episodes is associated with severe retinopathy of prematurity. J. Pediatrics 2010, 157, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, R.J.; Wang, K.; Köroğlu, O.; Di Fiore, J.; Kc, P. Intermittent hypoxic episodes in preterm infants: Do they matter? Neonatology 2011, 100, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Schonhaut, L.; Armijo, I.; Schönstedt, M.; Alvarez, J.; Cordero, M. Validity of the ages and stages questionnaires in term and preterm infants. Pediatrics 2013, 131, e1468–e1474. [Google Scholar] [CrossRef] [Green Version]
- Apnea, sudden infant death syndrome, and home monitoring. Pediatrics 2003, 111, 914–917. [CrossRef] [Green Version]
- Michael, J.; Corwin, M. Use of Home Cardiorespiratory Monitors in Infants; George, B., Mallory, M., Leonard, E., Weisman, M.D., Eds.; Uptodate: Waltham, MA, USA, 2020. [Google Scholar]
- Samra, H.A.; McGrath, J.M.; Fischer, S.; Schumacher, B.; Dutcher, J.; Hansen, J. The NICU Parent Risk Evaluation and Engagement Model and Instrument (PREEMI) for neonates in intensive care units. J. Obstet. Gynecol. Neonatal Nurs. JOGNN 2015, 44, 114–126. [Google Scholar] [CrossRef]


{kind=link}
| Maternal & Newborn Characteristics | Preterm Infants Home on Caffeine (87) | Preterm Infants Home without Caffeine (210) | p Value |
|---|---|---|---|
| Gestational age, weeks a | 28 ± 3 | 29 ± 2 | <0.05 Ω |
| Birth weight, grams a | 1236 ± 420 | 1349 ± 416 | 0.03 Ω |
| Hispanic, n (%) | 64(74) | 143(68) | NS |
| Vaginal, n (%) | 32(37) | 71(34) | NS |
| Male, n (%) | 51(58) | 98(47) | NS |
| Apgar score, n b, min | |||
| 1 | 6(3–7) | 6(4–7) | NS |
| 5 | 7(6–8) | 7(6–8) | NS |
| Apgar ≤ 5 at 5 min, n (%) | 16(18) | 31(15) | NS |
| Maternal Prenatal care n (%) | 84(96) | 196(93) | NS |
| SGA n (%) | 12(14) | 27(13) | NS |
| Antenatal Steroids, n (%) | 66(76) | 164(79) | NS |
| In Hospital Morbidity | Preterm Infants Home on Caffeine (87) | Preterm Infants Home without Caffeine (210) | p Value |
|---|---|---|---|
| Respiratory distress syndrome, n (%) Given surfactant | 64(74) | 135(64) | NS |
| No. of days of mechanical Ventilation a | 19 ± 27 | 19 ± 32 | NS Ω |
| BPD, n (%) | 29(33) | 46(22) | 0.05 |
| Oxygen at discharge *, n (%) | 21(24) | 27(13) | 0.02 |
| Intraventricular hemorrhage (IVH) | |||
| Any IVH, n (%) | 57(72) | 152(66) | NS |
| Severe IVH (grade III or IV), n (%) | 8(9) | 8(4) | NS |
| Retinopathy of prematurity (ROP)requiring anti vascular endothelial growth factor (VEGF) treatment, n (%) | 4(4.5) | 10(4.7) | NS |
| Necrotizing enterocolitis, any stage, n (%) | 1(1) | 14(6) | NS |
| Discharge weight (grams) a | 2654 ± 493 | 2625 ± 632 | NS Ω |
| Discharge head circumference a | 33 ± 1.7 | 33 ± 1.5 | NS Ω |
| Length of Stay, days a | 68 ± 30 | 62 ± 36 | NS Ω |
| Parameters at Discharge and During First Year of Life | Preterm Infants Home on Caffeine (87) | Preterm Infants Home without Caffeine (210) | p Value |
|---|---|---|---|
| Apnea Monitor at discharge, n (%) | 80(91) | 1(0.04) | - |
| Number of days on Caffeine till first attempt to stop a | 47 ± 28 | 39 ± 28 | 0.02 Ω |
| Ever an attempt to stop caffeine, n (%) | 73(84) | 210(100) | <0.05 |
| Corrected gestation at first attempt to stop in nicu a | 35 ± 3 | 35 ± 3 | NS |
| Gestation at discharge a | 38 ± 2 | 38 ± 4 | NS |
| No. of adjustments to dose made during hospitalization a | 7 ± 4 | 5 ± 3 | <0.05 Ω |
| Median days to restarting caffeine after initial attempt | 5(3–9) | - | - |
| Reasons for Restarting Caffeine | - | ||
| No. of infants with persistent Apneic events | 2 | ||
| No. of infants with combination of persistent Apneic, Bradycardia and Desaturations events | 35 | ||
| No. of infants with combination of persistent bradycardia and events | 54 | ||
| No. of days from Caffeine Stop to discharge b | - | 16(10–25) | - |
| Dose (mg/kg/day)of Caffeine at discharge a | 8 ± 2 | - | - |
| No. of days monitored in NICU from caffeine restart to discharge | 7(5–13) | - | - |
| No. of days on caffeine post discharge b | 31(28–42) | - | - |
| Cost of Apnea monitor use post discharge in dollars USD 750 per 30 days (Medicaid reimbursement) a | USD 1326 ± 970 | - | - |
| Cost of Caffeine at home in dollars a | USD 50 ± 34 | - | - |
| Corrected gestational age caffeine stopped after discharge a | 43 ± 4 | - | |
| No. of days on apnea monitor after caffeine stop at home b | 31(11–36) | - | - |
| No. Infants with follow up in Neonatal follow up clinic, n (%) | 83(95) | 173(82) | 0.02 Ω |
| Weight (kg) at 6 months clinic visit a | 6.5 ± 1.2 | 6.4 ± 1 | NS |
| Weight (kg) at 1 year clinic visit a | 8 ± 1 | 8.3 ± 1 | NS |
| Scores in 5 domains of Ages and Stages Questionnaire | |||
| At 6 months clinic visit a | |||
| Communication | 53 ± 9 | 55 ± 6 | NS Ω |
| Gross motor | 50 ± 11 | 48 ± 13 | NS Ω |
| Fine motor | 50 ± 12 | 51 ± 11 | NS Ω |
| Problem solving | 53 ± 11 | 53 ± 10 | NS Ω |
| Personal social | 51 ± 10 | 49 ± 12 | NS Ω |
| At 1-year clinic visit a | |||
| Communication | 42 ± 16 | 47 ± 13 | NS Ω |
| Gross motor | 47 ± 20 | 48 ± 16 | NS Ω |
| Fine motor | 47 ± 16 | 51 ± 12 | NS Ω |
| Problem solving | 46 ± 16 | 50 ± 19 | NS Ω |
| Personal social | 41 ± 16 | 47 ± 19 | NS Ω |
| Parameters during First Year of Life Post NICU Discharge | Preterm Infants Home on Caffeine (87) | Preterm Infants Home without Caffeine (210) | p Value * |
|---|---|---|---|
| Infant with ED Visits Post Discharge | |||
| No. of infants with ED visit after discharge in first year of life, n (%) | 26(30) | 67(32) | NS |
| Reasons and number for ED visits within first year of life after discharging home | |||
| BRUE, n (% of total no. of infant with ED visit) | 6(23) | 6(9) | NS |
| Respiratory disease, n (%of total no. of infant with ED visit) | 15(57) | 44(65) | NS |
| Fever, n(%of total no. of infant with ED visit) | 6(2) | 12(2) | NS |
| AGE, n(% of total no. of infant with ED visit) | 4(2) | 20(30) | NS |
| Rash, n (% of total no. of infant with ED visit) | 0(0) | 4(1) | NS |
| Other, n (% of total no. of infant with ED visit) | 25(96) | 50(75) | NS |
| Total number of ED visits, n | 56 | 136 | NS |
| Ratio of Total number of ED visit to total infants visiting ED | 2.1 | 2 | |
| Infants Hospitalized Post Discharge | |||
| Total number of infants hospitalized after discharge in first year of life, n (%) | 10(11) | 20(10) | NS |
| Respiratory disease, n (% of total no. of infant Hospitalized) | 2(20) | 6(30) | NS |
| Fever, n (% of total no. of infant Hospitalized) | 1(10) | 1(5) | NS |
| AGE, n (% of total no. of infant Hospitalized) | 0 | 3(15) | NS |
| Rash, n (% of total no. of infant Hospitalized) | 0 | 0 | NS |
| Other, n (%of total no. of infant Hospitalized) | 1(10) | 6(30) | NS |
| Details of Brief Resolved Unexplained Events (BRUE/ALTE) | |||
| Preterm infants home on caffeine | Preterm infants home without caffeine | ||
| Total number of infants | 6 | 6 | |
| ED visits only | 0 | 4 | |
| On caffeine at home when ED/Hospitalized | 3 | ||
| Deaths in First year of life, n (% of all infants) | 0 | 3(1.4) | NS |
| Cause of death | SIDS in all three | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, C.; Broadbent, D.; Levin, G.; Panda, S.; Sambalingam, D.; Garcia, N.; Ruiz, E.; Singh, A.P. Discharging Preterm Infants Home on Caffeine, a Single Center Experience. Children 2020, 7, 114. https://doi.org/10.3390/children7090114
Ma C, Broadbent D, Levin G, Panda S, Sambalingam D, Garcia N, Ruiz E, Singh AP. Discharging Preterm Infants Home on Caffeine, a Single Center Experience. Children. 2020; 7(9):114. https://doi.org/10.3390/children7090114
Chicago/Turabian StyleMa, Cheng, Denisse Broadbent, Garrett Levin, Sanjeet Panda, Devaraj Sambalingam, Norma Garcia, Edson Ruiz, and Ajay Pratap Singh. 2020. "Discharging Preterm Infants Home on Caffeine, a Single Center Experience" Children 7, no. 9: 114. https://doi.org/10.3390/children7090114
APA StyleMa, C., Broadbent, D., Levin, G., Panda, S., Sambalingam, D., Garcia, N., Ruiz, E., & Singh, A. P. (2020). Discharging Preterm Infants Home on Caffeine, a Single Center Experience. Children, 7(9), 114. https://doi.org/10.3390/children7090114