All-Trans Retinoic Acid-Induced Ototoxicity during Chemotherapy in Pediatric Acute Promyelocytic Leukemia


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
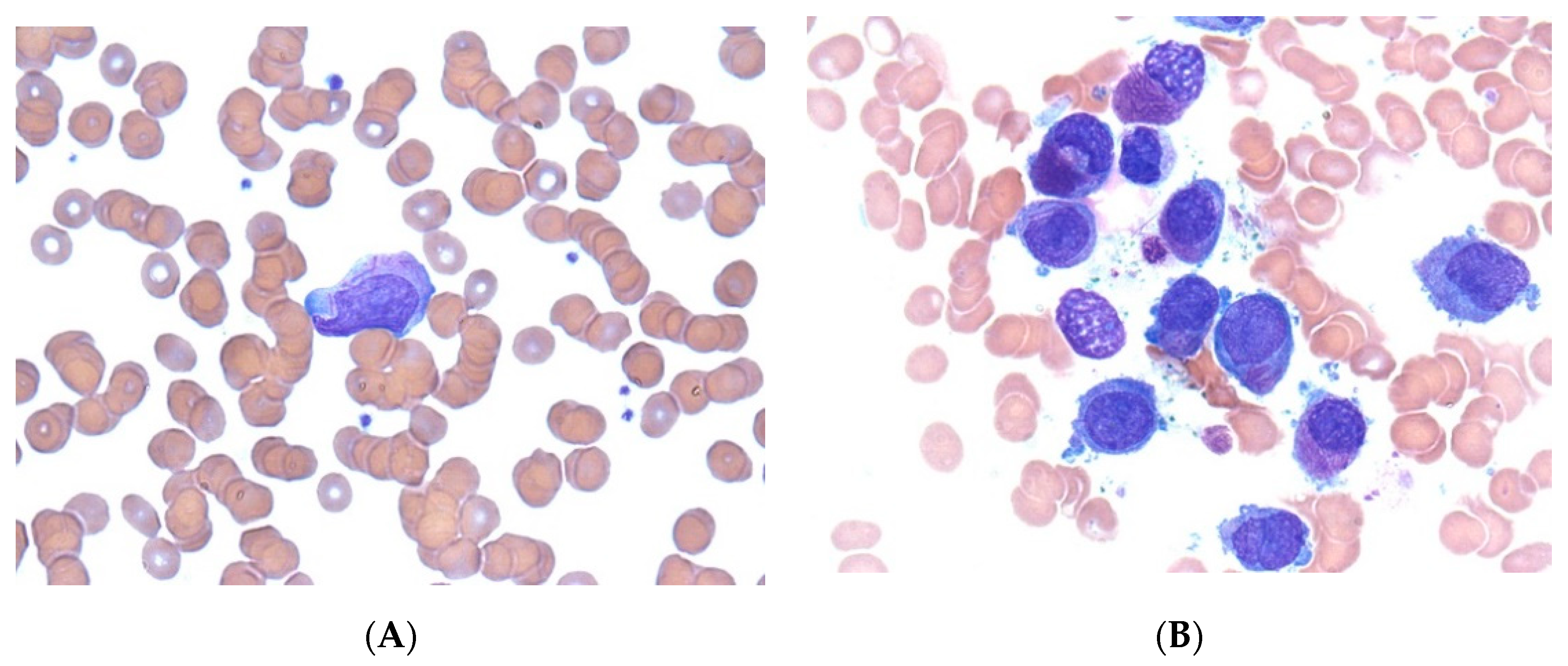
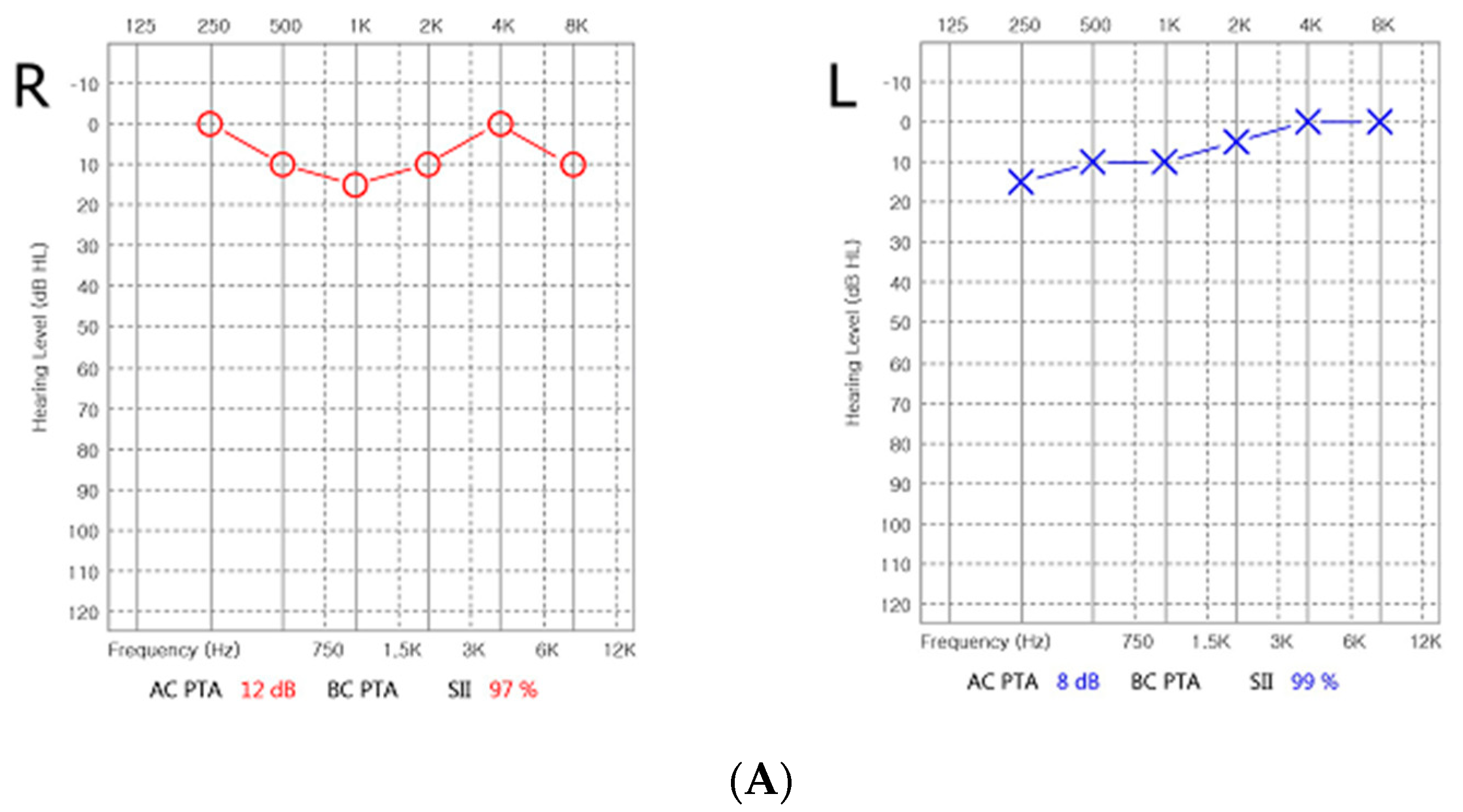
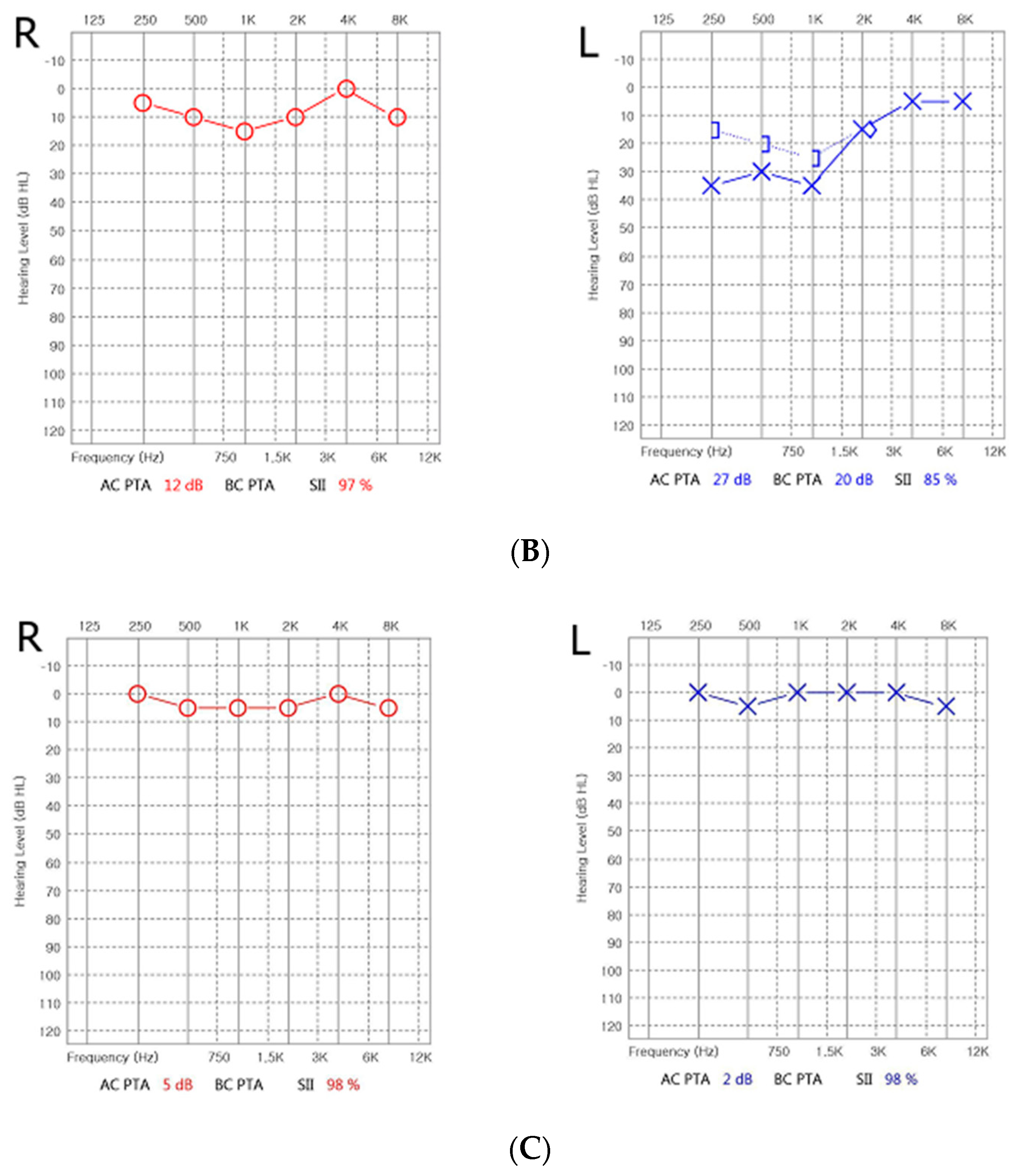
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stahl, M.; Tallman, M.S. Acute promyelocytic leukemia (APL): Remaining challenges towards a cure for all. Leuk. Lymphoma 2019, 60, 3107–3115. [Google Scholar] [CrossRef] [PubMed]
- Stahl, M.; Tallman, M.S. Differentiation syndrome in acute promyelocytic leukaemia. Br. J. Haematol. 2019, 187, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Fujiki, T.; Nishimura, R.; Ikawa, Y.; Noguchi, K.; Mase, S.; Kuroda, R.; Araki, R.; Maeba, H.; Yachie, A. Hearing impairment accompanied with low-tone tinnitus during all trans retinoic acid containing chemotherapy. Pediatr. Blood Cancer 2018, 65. [Google Scholar] [CrossRef] [PubMed]
- Bernard, J.; Weil, M.; Boiron, M.; Jacquillat, C.; Flandrin, G.; Gemon, M.F. Acute promyelocytic leukemia: Results of treatment by daunorubicin. Blood 1973, 41, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.-Y.; Chen, Z. Acute promyelocytic leukemia: From highly fatal to highly curable. Blood 2008, 111, 2505–2515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breitman, T.R.; Selonick, S.E.; Collins, S.J. Induction of differentiation of the human promyelocytic leukemia cell line (HL-60) by retinoic acid. Proc. Natl. Acad. Sci. USA 1980, 77, 2936–2940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomita, A.; Kiyoi, H.; Naoe, T. Mechanisms of action and resistance to all-trans retinoic acid (ATRA) and arsenic trioxide (As2O3) in acute promyelocytic leukemia. Int. J. Hematol. 2013, 97, 717–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libien, J.; Kupersmith, M.J.; Blaner, W.; McDermott, M.P.; Gao, S.; Liu, Y.; Corbett, J.; Wall, M. Role of vitamin A metabolism in IIH: Results from the idiopathic intracranial hypertension treatment trial. J. Neurol. Sci. 2017, 372, 78–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinker, T.; Stopa, E.; Morrison, J.; Klinge, P. A new look at cerebrospinal fluid circulation. Fluids Barriers CNS 2014, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montesinos, P.; Bergua, J.M.; Vellenga, E.; Rayón, C.; Parody, R.; de la Serna, J.; León, A.; Esteve, J.; Milone, G.; Debén, G.; et al. Differentiation syndrome in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline chemotherapy: Characteristics, outcome, and prognostic factors. Blood 2009, 113, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.A.; Fenaux, P.; Tallman, M.S.; Estey, E.H.; Löwenberg, B.; Naoe, T.; Lengfelder, E.; Döhner, H.; Burnett, A.K.; Chen, S.-J.; et al. Management of acute promyelocytic leukemia: Updated recommendations from an expert panel of the European LeukemiaNet. Blood 2019, 133, 1630–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Lee, J.H.; Lee, J.M. All-Trans Retinoic Acid-Induced Ototoxicity during Chemotherapy in Pediatric Acute Promyelocytic Leukemia. Children 2021, 8, 27. https://doi.org/10.3390/children8010027
Lee JH, Lee JH, Lee JM. All-Trans Retinoic Acid-Induced Ototoxicity during Chemotherapy in Pediatric Acute Promyelocytic Leukemia. Children. 2021; 8(1):27. https://doi.org/10.3390/children8010027
Chicago/Turabian StyleLee, Jong Hyeon, Jong Ho Lee, and Jae Min Lee. 2021. "All-Trans Retinoic Acid-Induced Ototoxicity during Chemotherapy in Pediatric Acute Promyelocytic Leukemia" Children 8, no. 1: 27. https://doi.org/10.3390/children8010027
APA StyleLee, J. H., Lee, J. H., & Lee, J. M. (2021). All-Trans Retinoic Acid-Induced Ototoxicity during Chemotherapy in Pediatric Acute Promyelocytic Leukemia. Children, 8(1), 27. https://doi.org/10.3390/children8010027