Lessons Learned from a Collaborative to Develop a Sustainable Simulation-Based Training Program in Neonatal Resuscitation: Simulating Success

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. CHOC
2.2. SMB
2.3. VCH
3. Results
3.1. CHOC
3.1.1. SMART Aim #1
3.1.2. SMART Aim #2
3.1.3. Other Notable Results
3.1.4. Lessons Learned
3.1.5. Challenges Faced
3.2. SMB
3.2.1. SMART Aim #1
3.2.2. Lessons Learned
3.2.3. Challenges Faced
3.3. VCH
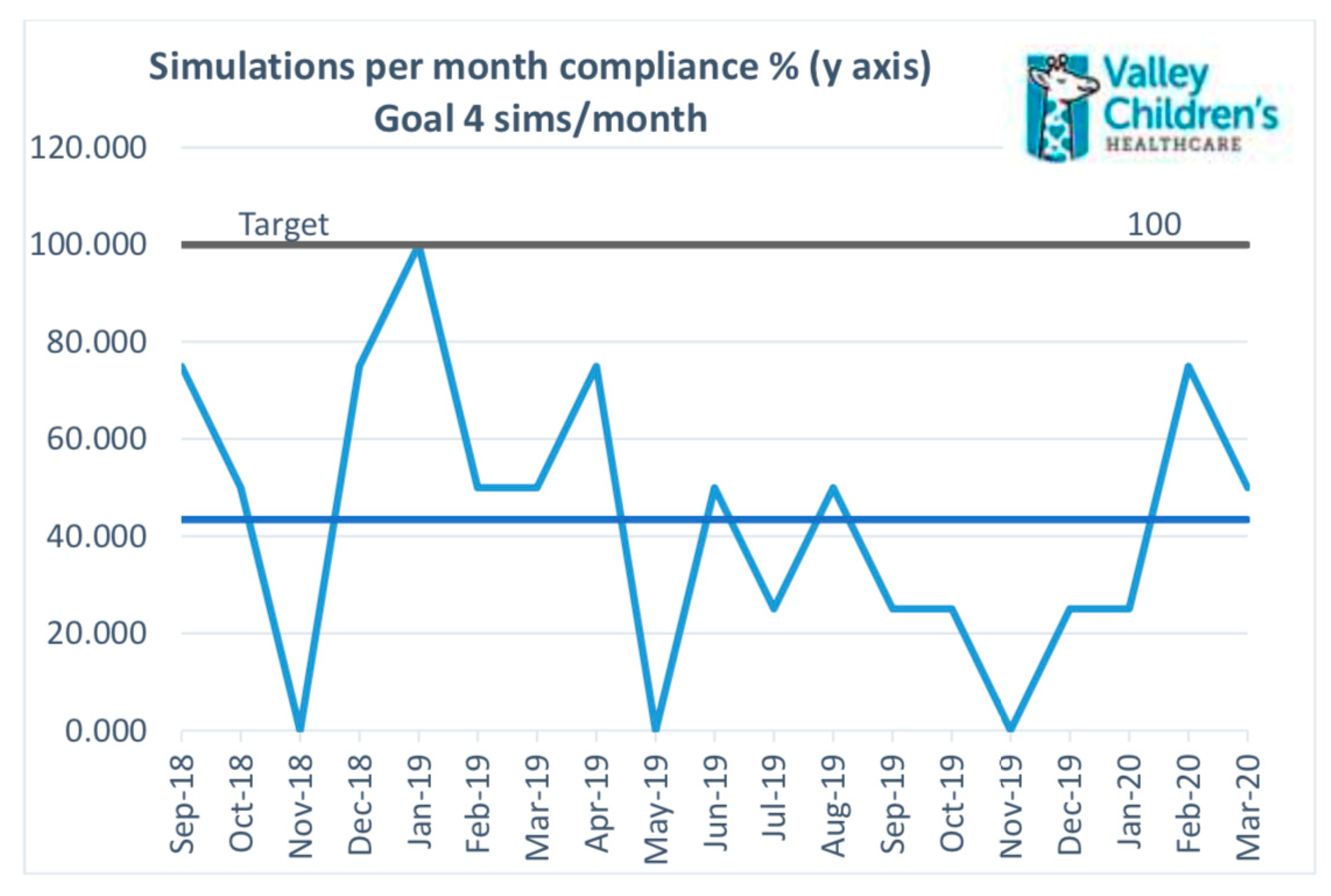
3.3.1. SMART Aim #1
3.3.2. SMART Aim #2
3.3.3. Other
- Increase participation in 2–3 simulations/year from 18% to 40%;
- Decrease dissatisfaction with simulation experience to <10%;
- Decrease lack of confidence in the ability to participate in a neonatal code blue to <10%;
- Decrease lack of confidence in the ability to lead a neonatal code blue to <10%;
- Decrease lack of comfort with communication skills required during a neonatal resuscitation to <5%.
3.3.4. Lessons Learned
3.3.5. Challenges Faced
4. Discussion
4.1. Future Directions: CHOC
4.2. Future Directions: SMB
4.3. Future Directions: VCH
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1a. I clearly understood the purpose and objectives of this simulation exercise: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 59 | 33 |
| Agree | 32 | 18 |
| Disagree | 2 | 1 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 1b. The scenario represented a real-life situation: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 59 | 33 |
| Agree | 34 | 19 |
| Disagree | 0 | 0 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 1c. The debriefing discussion after the simulation was constructive: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 68 | 38 |
| Agree | 21 | 12 |
| Disagree | 4 | 2 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 1d. I felt that the learning environment was safe: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 71 | 40 |
| Agree | 21 | 12 |
| Disagree | 0 | 0 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 1e. I would like to participate in another simulation experience: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 52 | 29 |
| Agree | 38 | 21 |
| Disagree | 2 | 1 |
| Strongly Disagree | 7 | 4 |
| Total | 55 | |
| 2a. As a result of the simulation experience, I have increased my ability to anticipate the needs of other team members: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 52 | 29 |
| Agree | 39 | 22 |
| Disagree | 2 | 1 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 2b. As a result of the simulation experience, I have increased my ability to communicate efficiently with other team members: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 50 | 28 |
| Agree | 41 | 23 |
| Disagree | 2 | 1 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 3a. The facilitators were knowledgeable about patient care in the scenario: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 64 | 36 |
| Agree | 29 | 16 |
| Disagree | 0 | 0 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 3b. The facilitators were well prepared for the session: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 68 | 38 |
| Agree | 21 | 12 |
| Disagree | 4 | 2 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 3c. The facilitators encouraged active participation during the debriefing session: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 70 | 39 |
| Agree | 23 | 13 |
| Disagree | 0 | 0 |
| Strongly Disagree | 7 | 4 |
| Total | 56 | |
| 4a. The scenario was presented in a realistic environment: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 59 | 33 |
| Agree | 36 | 20 |
| Disagree | 0 | 0 |
| Strongly Disagree | 5 | 3 |
| Total | 56 | |
| 4b. The location and time worked for me: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 46 | 26 |
| Agree | 36 | 20 |
| Disagree | 13 | 7 |
| Strongly Disagree | 5 | 3 |
| Total | 56 | |
| 4c. The session lasted about the right time: | ||
| Answer Choices | Percentage % | Responses |
| Strongly Agree | 54 | 30 |
| Agree | 36 | 20 |
| Disagree | 5 | 3 |
| Strongly Disagree | 5 | 3 |
| Total | 56 | |
| 5. What were the positive aspects of the experience? | ||
| 6. What changes would you recommend to improve future simulation experiences? | ||
| 7. Additional Comments: Examples below: “Created a great learning environment and the multidisciplinary aspect was helpful and made it more realistic.” “I liked the discussion of the medical aspect and the crisis resource management for each simulation.” “Non-judgmental, Informative.” “The situation was more real than other simulations I have been a part of in the past 3 years.” “Being able to work through common hiccups with critical situations, work through the and debrief afterwards improved confidence in being at bedside.” | ||
Appendix C
| 1. What is your current role in the NICU: | |||
| Answer Choices | Percentage % | Responses | |
| Advanced Life Support Nurse | 3.6 | 2 | |
| Registered Nurse | 67.3 | 37 | |
| Respiratory Therapist | 20.0 | 11 | |
| Physician | 3.6 | 2 | |
| Nurse Practitioner | 1.8 | 1 | |
| Other | 3.6 | 2 | |
| Total | 55 | ||
| Mean | SD | ||
| 2. # Years in Current Role | 14.02 | 10.6 | |
| 3. # Years in Current Role at SMB | 9.82 | 8.5 | |
| 4. # Sim & Debrief sessions in past year | 2.33 | 1.9 | |
| 5. # Code Pink Events in past year | 0.68 | 1.1 | |
| 6. Since participating in NICU Simulation and Debriefing, I have become more confident in my ability to communicate effectively during an emergency: | |||
| Answer Choices | Percentage % | Responses | |
| Strongly Agree | 50 | 27 | |
| Agree | 50 | 27 | |
| Disagree | 0 | 0 | |
| Strongly Disagree | 0 | 0 | |
| Total | 54 | ||
| 7. Since participating in NICU Simulation and Debriefing, I am able to recognize and intervene in a rapidly changing patient situation: | |||
| Answer Choices | Percentage % | Responses | |
| Strongly Agree | 46.3 | 25 | |
| Agree | 53.7 | 29 | |
| Disagree | 0 | 0 | |
| Strongly Disagree | 0 | 0 | |
| Total | 54 | ||
| 8. I am able to voice my concerns during a critical situation: | |||
| Answer Choices | Percentage % | Responses | |
| Strongly agree | 63.0 | 34 | |
| Agree | 37.0 | 20 | |
| Disagree | 0 | 0 | |
| Strongly disagree | 0 | 0 | |
| Total | 54 | ||
| 9. Overall, I am confident in my ability to participate as an essential team member in a neonatal code: | |||
| Answer Choices | Percentage % | Responses | |
| Strongly agree | 40.7 | 22 | |
| Agree | 59.3 | 32 | |
| Disagree | 0 | 0 | |
| Strongly disagree | 0 | 0 | |
| Total | 54 | ||
| 10. The debriefing process is effective in aiding the team and learner to reflect on team performance and identify potential learning opportunities: | |||
| Answer Choices | Percentage % | Responses | |
| Strongly agree | 70.4 | 38 | |
| Agree | 29.6 | 16 | |
| Disagree | 0 | 0 | |
| Strongly disagree | 0 | 0 | |
| Total | 54 | ||
Appendix D
| 1. Number of simulations (excluding NRP) you have participated in during the last year: | ||
| Answer Choices | Percentage % | Responses |
| 0–1 | 79 | 110 |
| 2–3 | 18 | 24 |
| 4+ | 3 | 4 |
| Total | 139 | |
| 2. I am satisfied with simulation experience: | ||
| Answer Choices | Percentage % | Responses |
| Strongly disagree | 7 | 9 |
| Disagree | 14 | 19 |
| Agree | 61 | 83 |
| Strongly agree | 19 | 26 |
| Total | 137 | |
| 3. I am confident in my ability to participate in a neonatal code blue: | ||
| Answer Choices | Percentage % | Responses |
| Strongly disagree | 4 | 5 |
| Disagree | 11 | 15 |
| Agree | 56 | 77 |
| Strongly agree | 30 | 41 |
| Total | 138 | |
| 4. I am confident in my ability to be a team leader during a neonatal code blue: | ||
| Answer Choices | Percentage % | Responses |
| Strongly disagree | 8 | 11 |
| Disagree | 28 | 38 |
| Agree | 38 | 53 |
| Strongly agree | 26 | 36 |
| Total | 138 | |
| 5. I am confident with my ability to perform skills of neonatal resuscitation (i.e., positive pressure ventilation, chest compression, dosing and administering medications): | ||
| Answer Choices | Percentage % | Responses |
| Strongly disagree | 1 | 2 |
| Disagree | 7 | 9 |
| Agree | 59 | 82 |
| Strongly agree | 33 | 46 |
| Total | 139 | |
| 6. I am confident in my ability to anticipate clinical changes and interventions needed at bedside: | ||
| Answer Choices | Percentage % | Responses |
| Strongly disagree | 1 | 2 |
| Disagree | 2 | 3 |
| Agree | 57 | 79 |
| Strongly agree | 40 | 55 |
| Total | 139 | |
| 7. I am comfortable with my communication skills required during a neonatal resuscitation: | ||
| Answer Choices | Percentage % | Responses |
| Strongly disagree | 2 | 3 |
| Disagree | 8 | 11 |
| Agree | 58 | 80 |
| Strongly agree | 32 | 45 |
| Total | 139 | |
References
- The Joint Commission: Sentinel Event Alert Issue 30. Available online: https://www.jointcommission.org/-/media/deprecated-unorganized/imported-assets/tjc/system-folders/topics-library/sea_30pdf.pdf (accessed on 18 September 2020).
- Edwards, E.M.; Soll, R.F.; Ferrelli, K.; Morrow, K.A.; Suresh, G.; Celenza, J.; Horbar, J.D. Identifying improvements for deliv-ery room resuscitation management: Results from a multicenter safety audit. Matern. Health Neonatol. Perinatol. 2015, 1, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carbine, D.N.; Finer, N.N.; Knodel, E.; Rich, W. Video recording as a means of evaluating neonatal resuscitation perfor-mance. Pediatrics 2000, 106, 654–658. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, L.K.; Morley, C.J.; Davis, P.G.; Kamlin, C.O.F.; O’Donnell, C.P. Timing of Interventions in the Delivery Room: Does Reality Compare with Neonatal Resuscitation Guidelines? Pediatrics 2013, 163, 1553–1557.e1. [Google Scholar] [CrossRef] [PubMed]
- Halamek, L.P.; Kaegi, D.M.; Gaba, D.M.; Sowb, Y.A.; Smith, B.C.; Howard, S.K. Time for a New Paradigm in Pediatric Medical Education: Teaching Neonatal Resuscitation in a Simulated Delivery Room Environment. Pediatrics 2000, 106, e45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaeger, K.A.; Halamek, L.P.; Coyle, M.; Murphy, A.; Anderson, J.; Boyle, K.; Braccia, K.; McAuley, J.; De Sandre, G.; Smith, B. High-fidelity simulation-based training in neonatal nursing. Adv. Neonatal Care 2004, 4, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Nadkarni, V.M.; Mancini, M.B.; Hunt, E.A.; Sinz, E.H.; Merchant, R.M.; Donoghue, A.; Duff, J.P.; Eppich, W.; Auerbach, M.; et al. Resuscitation Education Science: Educational Strategies to Im-prove Outcomes from Cardiac Arrest: A Scientific Statement From the American Heart Association. Circulation 2018, 138, e82–e122. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.J.; Sexton, J.B.; Lasky, R.E.; Helmreich, R.L.; Crandell, D.S.; Tyson, J. Teamwork and quality during neonatal care in the delivery room. J. Perinatol. 2006, 26, 163–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunt, E.A.; Shilkofski, N.A.; Stavroudis, T.A.; Nelson, K.L. Simulation: Translation to Improved Team Performance. Anesthesiol. Clin. 2007, 25, 301–319. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.J.; Taggart, B.; Crandell, S.; Lasky, R.E.; Williams, A.L.; Love, L.J.; Sexton, J.B.; Tyson, J.E.; Helmreich, R.L. Teaching teamwork during the Neonatal Resuscita-tion Program: A randomized trial. J. Perinatol. 2007, 27, 409–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ades, A.M.; Lee, H.C. Update on simulation for the Neonatal Resuscitation Program. Semin. Perinatol. 2016, 40, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Mytton, O.T.; Derbrew, M.; Hananel, D.; Heydenburg, M.; Issenberg, B.; Macaulay, C.; Mancini, M.E.; Morimoto, T.; Soper, N.; et al. Training and simulation for patient safety. Qual. Saf. Health Care 2010, 19, i34–i43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubio-Gurung, S.; Putet, G.; Touzet, S.; Gauthier-Moulinier, H.; Jordan, I.; Beissel, A.; Labaune, J.-M.; Blanc, S.; Amamra, N.; Balandras, C.; et al. In Situ Simulation Training for Neonatal Resuscitation: An RCT. Pediatrics 2014, 134, e790–e797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guise, J.-M.; Mladenovic, J. In situ simulation: Identification of systems issues. Semin. Perinatol. 2013, 37, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Shojania, K.G.; Duncan, B.W.; McDonald, K.M.; Wachter, R.M.; Markowitz, A.J. Making health care safer: A critical analysis of patient safety practices. Evid. Rep. Technol. Assess. 2001, 43, 1–668. [Google Scholar]
- World Health Organization’s World Alliance for Patient Safety: Summary of the Evidence on Patient Safety: Implications for Research. Available online: https://www.who.int/patientsafety/information_centre/Summary_evidence_on_patient_safety.pdf (accessed on 18 September 2020).
- Wetzel, E.A.; Lang, T.R.; Pendergrass, T.L.; Taylor, R.G.; Geis, G.L. Identification of Latent Safety Threats Using High-Fidelity Simulation-Based Training with Multidisciplinary Neonatology Teams. Jt. Comm. J. Qual. Patient Saf. 2013, 39, 268–273. [Google Scholar] [CrossRef]
- Patterson, M.D.; Blike, G.T.; Nadkarni, V.M. In Situ Simulation: Challenges and Results. In Advances in Patient Safety: New Directions and Alternative Approaches; Henriksen, K., Battles, J.B., Keyes, M.A., Grady, M.L., Eds.; Agency for Healthcare Re-search and Quality: Rockville, MD, USA, 2008; Volume 3. [Google Scholar]
- Reed, D.J.W.; Hermelin, R.L.; Kennedy, C.S.; Sharma, J. Interdisciplinary onsite team-based simulation training in the neonatal intensive care unit: A pilot report. J. Perinatol. 2017, 37, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Halamek, L.P. Simulation and debriefing in neonatology 2016: Mission incomplete. Semin. Perinatol. 2016, 40, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, T.; Sierocka-Castaneda, A.; Chan, D.; Berg, B.; Lustik, M.; Thompson, M. Deliberate practice using simulation im-proves neonatal resuscitation performance. Simul. Healthc. 2011, 6, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Rivera, E.K.; Siple, L.M.; Wicks, E.J.; Johnson, H.S.; Skov, C.M. In Situ Neonatal Mock Codes: Assessing the Impact. Neonatal Netw. 2020, 39, 29–34. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arul, N.; Ahmad, I.; Hamilton, J.; Sey, R.; Tillson, P.; Hutson, S.; Narang, R.; Norgaard, J.; Lee, H.C.; Bergin, J.; et al. Lessons Learned from a Collaborative to Develop a Sustainable Simulation-Based Training Program in Neonatal Resuscitation: Simulating Success. Children 2021, 8, 39. https://doi.org/10.3390/children8010039
Arul N, Ahmad I, Hamilton J, Sey R, Tillson P, Hutson S, Narang R, Norgaard J, Lee HC, Bergin J, et al. Lessons Learned from a Collaborative to Develop a Sustainable Simulation-Based Training Program in Neonatal Resuscitation: Simulating Success. Children. 2021; 8(1):39. https://doi.org/10.3390/children8010039
Chicago/Turabian StyleArul, Nandini, Irfan Ahmad, Justin Hamilton, Rachelle Sey, Patricia Tillson, Shandee Hutson, Radhika Narang, Jennifer Norgaard, Henry C. Lee, Janine Bergin, and et al. 2021. "Lessons Learned from a Collaborative to Develop a Sustainable Simulation-Based Training Program in Neonatal Resuscitation: Simulating Success" Children 8, no. 1: 39. https://doi.org/10.3390/children8010039
APA StyleArul, N., Ahmad, I., Hamilton, J., Sey, R., Tillson, P., Hutson, S., Narang, R., Norgaard, J., Lee, H. C., Bergin, J., Quinn, J., Halamek, L. P., Yamada, N. K., Fuerch, J., & Chitkara, R. (2021). Lessons Learned from a Collaborative to Develop a Sustainable Simulation-Based Training Program in Neonatal Resuscitation: Simulating Success. Children, 8(1), 39. https://doi.org/10.3390/children8010039