
Fifteen-Years Follow-Up in a Cohort of Children with Functional Gastrointestinal Disorders: Prevalence and Risk Factors to Develop Neuropsychiatric Disorders and Other Comorbidities

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Le Gal, J.; Michel, J.-F.; Rinaldi, V.E.; Spiri, D.; Moretti, R.; Bettati, D.; Romanello, S.; Berlese, P.; Lualdi, R.; Boizeau, P.; et al. Association between functional gastrointestinal disorders and migraine in children and adolescents: A case-control study. Lancet Gastroenterol. Hepatol. 2016, 1, 114–121. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Subcommittee on Chronic Abdominal Pain and NASPGHAN Committee on Abdominal Pain. Chronic Abdominal Pain in Children: A Clinical Report of the American Academy of Pediat-rics and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. JPGN 2005, 40, 245–248. [Google Scholar]
- Waters, A.M.; Schilpzand, E.; Bell, C.; Walker, L.S.; Baber, K. Functional Gastrointestinal symptoms in children with anxiety dosorderes. J. Abnorm. Child Psychol. 2013, 41, 151–163. [Google Scholar] [CrossRef]
- Black, C.J.; Drossman, D.A.; Talley, N.J.; Ruddy, J.; Ford, A.C. Functional gastrointestinal Disorders: Advances in under-standing and management. Lancet 2020, 21, 1664–1674. [Google Scholar] [CrossRef]
- Zeevenhooven, J.; Koppen, I.G.N.; Benninga, M.A. The New Rome IV Criteria for Functional Gastrointestinal Disor-ders in Infants and Toddlers. Pediatr. Gastroenterol. Hepatol. Nutr. 2017, 20, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, E.; Labus, J.; Aziz, Q.; Tracey, I.; Kilpatrick, L.; Elsenbruch, S.; Schweinhardt, P.; Van Oudenhove, L.; Borsook, D. Role of brain imaging in disorders of brain–gut interaction: A Rome Working Team Report. Gut 2019, 68, 1701–1715. [Google Scholar] [CrossRef]
- Lee, I.-S.; Wang, H.; Chae, Y.; Preißl, H.; Enck, P. Functional neuroimaging studies in functional dyspepsia patients: A systematic review. Neurogastroenterol. Motil. 2016, 28, 793–805. [Google Scholar] [CrossRef]
- Jones, M.P.; Tack, J.; Van Oudenhove, L.; Walker, M.M.; Holtmann, G.; Koloski, N.A. Mood and anxiety disorders pre-cede development of functional gastrointestinal disorders in patients but not in the population. Clin. Gastroen-terol. Hepatol. 2017, 15, 1014–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koloski, N.A.; Jones, M.; Talley, N.J. Evidence that independent gut-to-brain and brain-to-gut pathways operate in the irritable bowel syndrome and functional dyspepsia: A 1-year population-based prospective study. Aliment. Pharmacol. Ther. 2016, 44, 592–600. [Google Scholar] [CrossRef]
- Horst, S.; Shelby, G.; Anderson, J.; Acra, S.; Polk, D.B.; Saville, B.R.; Garber, J.; Walker, L.S. Predicting Persistence of Functional Abdominal Pain From Childhood Into Young Adulthood. Clin. Gastroenterol. Hepatol. 2014, 12, 2026–2032. [Google Scholar] [CrossRef] [Green Version]
- Cooke, H.J. Role of the ‘‘little brain’’ in the gut in water and electrolyte homeostasis. FASEB J. 1989, 3, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.P.; Crowell, M.D.; Olden, K.W.; Creed, F. Functional Gastrointestinal Disorders: An Update for the Psychiatrist. J. Psychosom. Res. 2007, 48, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.C.; Forman, D.; Bailey, A.G.; Axon, A.T.R.; Moayyedi, P. Fluctuation of gastrointestinal symptoms in the com-munity: A 10¬year longitudinal follow-up study. Aliment Pharmacol. Ther. 2008, 28, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Aro, P.; Talley, N.J.; Johansson, S.-E.; Agréus, L.; Ronkainen, J. Anxiety Is Linked to New-Onset Dyspepsia in the Swedish Population: A 10-Year Follow-up Study. Gastroenterology 2015, 148, 928–937. [Google Scholar] [CrossRef] [PubMed]
- Halder, S.L.; Locke, G.R., 3rd; Schleck, C.D.; Zinsmeister, A.R.; Melton, L.J., 3rd; Talley, N.J. Natural history of functional gastrointestinal disorders: A 12-year longitudinal population¬based study. Gastroenterology 2007, 133, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2016, 150, 1456–1468.e2. [Google Scholar] [CrossRef]
- Cámara-Lemarroy, C.R.; Rodriguez-Gutierrez, R.; Monreal-Robles, R.; Marfil-Rivera, A. Gastrointestinal disorders associated with migraine: A comprehensive review. World J. Gastroenterol. 2016, 22, 8149–8160. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, E.A.; Russo, A.F. CGRP and migraine: Could PACAP play a role too? Neuropeptides 2013, 47, 451–461. [Google Scholar] [CrossRef] [Green Version]
- Sándor, K.; Kormos, V.; Botz, B.; Imreh, A.; Bölcskei, K.; Gaszner, B.; Markovics, A.; Szolcsányi, J.; Shintani, N.; Hashimoto, H.; et al. Impaired nocifensive behaviours and mechanical hyperalgesia, but enhanced thermal allodynia in pituitary adenylate cyclase-activating polypeptide deficient mice. Neuropeptides 2010, 44, 363–371. [Google Scholar] [CrossRef]
- Atkinson, W.; Lockhart, S.; Whorwell, P.J.; Keevil, B.; Houghton, L.A. Altered 5-hydroxytryptamine signaling in pa-tients with constipation- and diarrhea-predominant irritable bowel syndrome. Gastroenterology 2006, 130, 34–43. [Google Scholar] [CrossRef]
- Cheung, C.K.; Lee, Y.Y.; Chan, Y.; Cheong, P.K.; Law, W.T.; Lee, S.F.; Sung, J.J.; Chan, F.K.; Wu, J.C. Decreased Basal and Postprandial Plasma Serotonin Levels in Patients with Functional Dyspepsia. Clin. Gastroenterol. Hepatol. 2013, 11, 1125–1129. [Google Scholar] [CrossRef]
- Kakisaka, Y.; Wakusawa, K.; Haginoya, K.; Saito, A.; Uematsu, M.; Yokoyama, H.; Sato, T.; Tsuchiya, S. Efficacy of sumatriptan in two pediatric cases with abdominal pain-related functional gastrointestinal disorders: Does the mechanism overlap that of migraine? J. Child Neurol. 2010, 25, 234–237. [Google Scholar] [CrossRef]
- Spiri, D.; Rinaldi, V.E.; Titomanlio, L. Pediatric migraine and episodic syndromes that may be associated with mi-graine. Ital. J. Pediatr. 2014, 40, 92. [Google Scholar] [CrossRef] [Green Version]
- Park, J.W.; Cho, Y.S.; Lee, S.Y.; Kim, E.S.; Cho, H.; Shin, H.E.; Suh, G.I.; Choi, M.-G. Concomitant functional gastrointestinal symptoms in-fluence psychological status in Korean migraine patients. Gut Liver 2013, 7, 668–674. [Google Scholar] [CrossRef] [Green Version]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef] [PubMed]
- Basheti, I.A.; Mhaidat, Q.N.; Mhaidat, H.N. Prevalence of anxiety and depression during COVID-19 pandemic among healthcare students in Jordan and its effect on their learning process: A national survey. PLoS ONE 2021, 16, e0249716. [Google Scholar] [CrossRef] [PubMed]
- Hawes, M.T.; Szenczy, A.K.; Klein, D.N.; Hajcak, G.; Nelson, B.D. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Control Group n = 201 | Case Group n = 79 | p-Value | |
|---|---|---|---|
| Current Age, mean (SD) | 23.0 (2.7) | 23.2 (5.4) | 0.833 |
| Sex, n (%) | |||
| Males | 78 (38.8) | 39 (49.4) | 0.138 |
| Females | 123 (61.2) | 40 (50.6) | |
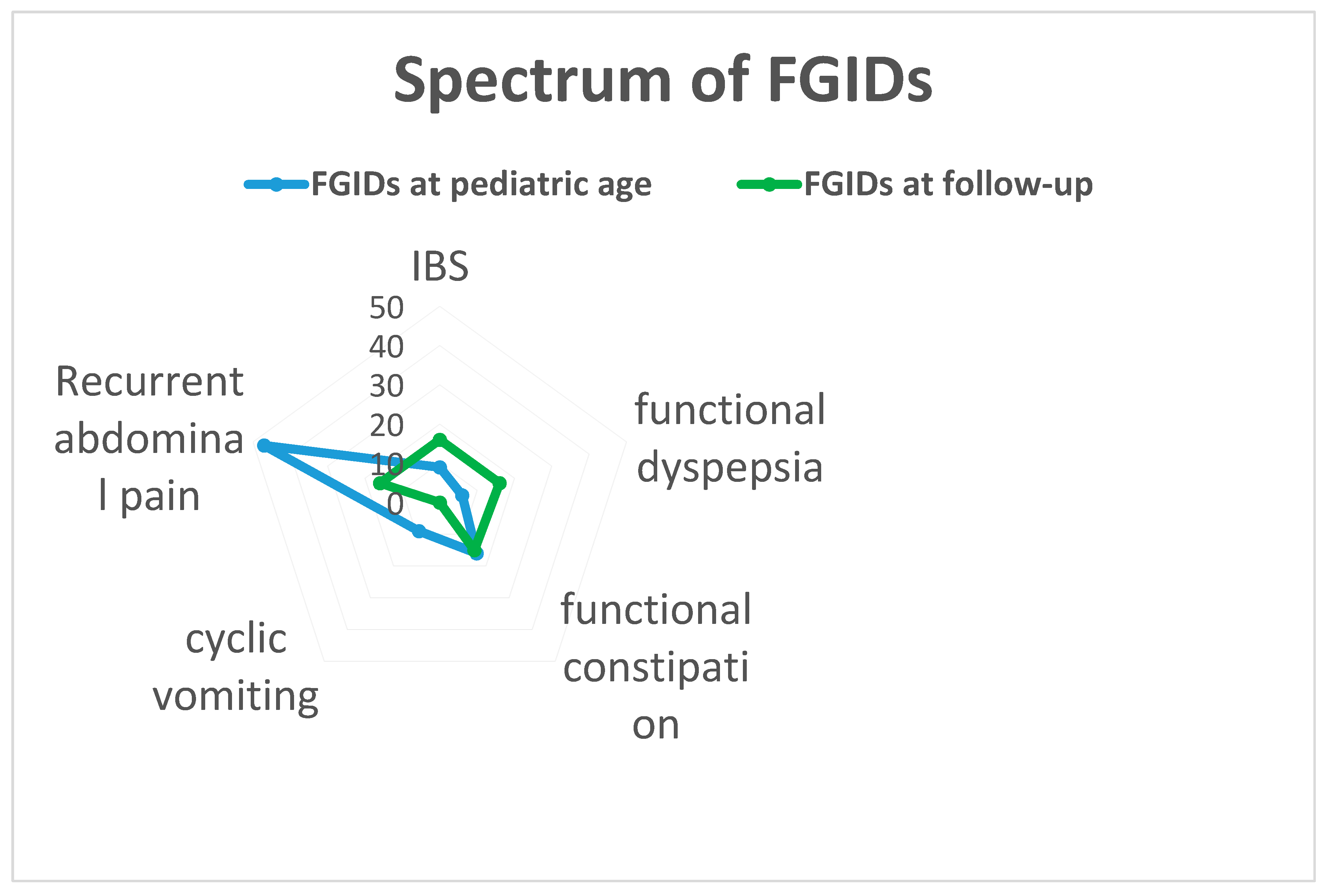
| FGIDs at pediatric age, n (%) | |||
| IBS | 9 (11) | ||
| Functional dyspepsia | 6 (8) | ||
| Functional constipation | 16 (20) | ||
| Cyclic vomiting | 9 (11) | ||
| Functional abdominal pain | 47 (59) | ||
| FGIDs at follow-up, n (%) | |||
| c | 14 (7.0) | 16 (20.2) | 0.002 |
| Functional dyspepsia | 4 (2.0) | 16 (20.2) | <0.001 |
| Functional constipation | 5 (2.5) | 15 (19.0) | <0.001 |
| Cyclic vomiting | 1 (0.5) | 0 | 1.000 |
| Functional abdominal pain | 10 (5.0) | 16 (20.2) | <0.001 |
| Organic disease, n (%) | |||
| Coeliac disease | 2 (1.0) | 2 (2.5) | 0.316 |
| Migraine or headache, n (%) | 26 (12.9) | 26 (32.9) | <0.001 |
| Psychiatric disorders, n (%) | |||
| Anxiety | 26 (12.9) | 15 (19.0) | 0.195 |
| Depression | 13 (6.5) | 5 (6.3) | 1.000 |
| Univariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|
| Anxiety or Depression | Events | n | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Current age | 17 | 79 | 1.07 | (0.96; 1.18) | 0.215 | 1.02 | (0.91; 1.13) | 0.738 |
| Sex | ||||||||
| Male | 4 | 39 | ||||||
| Female | 13 | 40 | 4.21 | (1.23; 14.38) | 0.022 | 3.96 | (1.02; 15.36) | 0.046 |
| Any FGIDs at current age | ||||||||
| No | 7 | 43 | ||||||
| Yes | 10 | 36 | 1.98 | (0.67; 5.88) | 0.220 | 1.69 | (0.50; 5.76) | 0.402 |
| Univariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|
| Migraine or Headache | Events | n | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Current age | 26 | 79 | 1.00 | (0.92; 1.09) | 0.998 | 0.95 | (0.86; 1.05) | 0.311 |
| Sex | ||||||||
| Male | 8 | 39 | ||||||
| Female | 18 | 40 | 3.17 | (1.17; 8.58) | 0.023 | 2.47 | (0.83; 7.34) | 0.104 |
| Any FGIDs at current age | ||||||||
| No | 10 | 43 | ||||||
| Yes | 16 | 36 | 2.64 | (1.01; 6.93) | 0.049 | 2.11 | (0.73; 6.12) | 0.170 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanchi, C.; Pintaldi, S.; Di Leo, G.; Ronfani, L.; Zamagni, G.; Viel, M.; Barbi, E.; Cozzi, G. Fifteen-Years Follow-Up in a Cohort of Children with Functional Gastrointestinal Disorders: Prevalence and Risk Factors to Develop Neuropsychiatric Disorders and Other Comorbidities. Children 2021, 8, 838. https://doi.org/10.3390/children8100838
Zanchi C, Pintaldi S, Di Leo G, Ronfani L, Zamagni G, Viel M, Barbi E, Cozzi G. Fifteen-Years Follow-Up in a Cohort of Children with Functional Gastrointestinal Disorders: Prevalence and Risk Factors to Develop Neuropsychiatric Disorders and Other Comorbidities. Children. 2021; 8(10):838. https://doi.org/10.3390/children8100838
Chicago/Turabian StyleZanchi, Chiara, Stefano Pintaldi, Grazia Di Leo, Luca Ronfani, Giulia Zamagni, Marialuisa Viel, Egidio Barbi, and Giorgio Cozzi. 2021. "Fifteen-Years Follow-Up in a Cohort of Children with Functional Gastrointestinal Disorders: Prevalence and Risk Factors to Develop Neuropsychiatric Disorders and Other Comorbidities" Children 8, no. 10: 838. https://doi.org/10.3390/children8100838
APA StyleZanchi, C., Pintaldi, S., Di Leo, G., Ronfani, L., Zamagni, G., Viel, M., Barbi, E., & Cozzi, G. (2021). Fifteen-Years Follow-Up in a Cohort of Children with Functional Gastrointestinal Disorders: Prevalence and Risk Factors to Develop Neuropsychiatric Disorders and Other Comorbidities. Children, 8(10), 838. https://doi.org/10.3390/children8100838