
Botulinum Toxin Injections for Treatment of Drooling in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Eligibility Criteria
2.2. Search Strategy
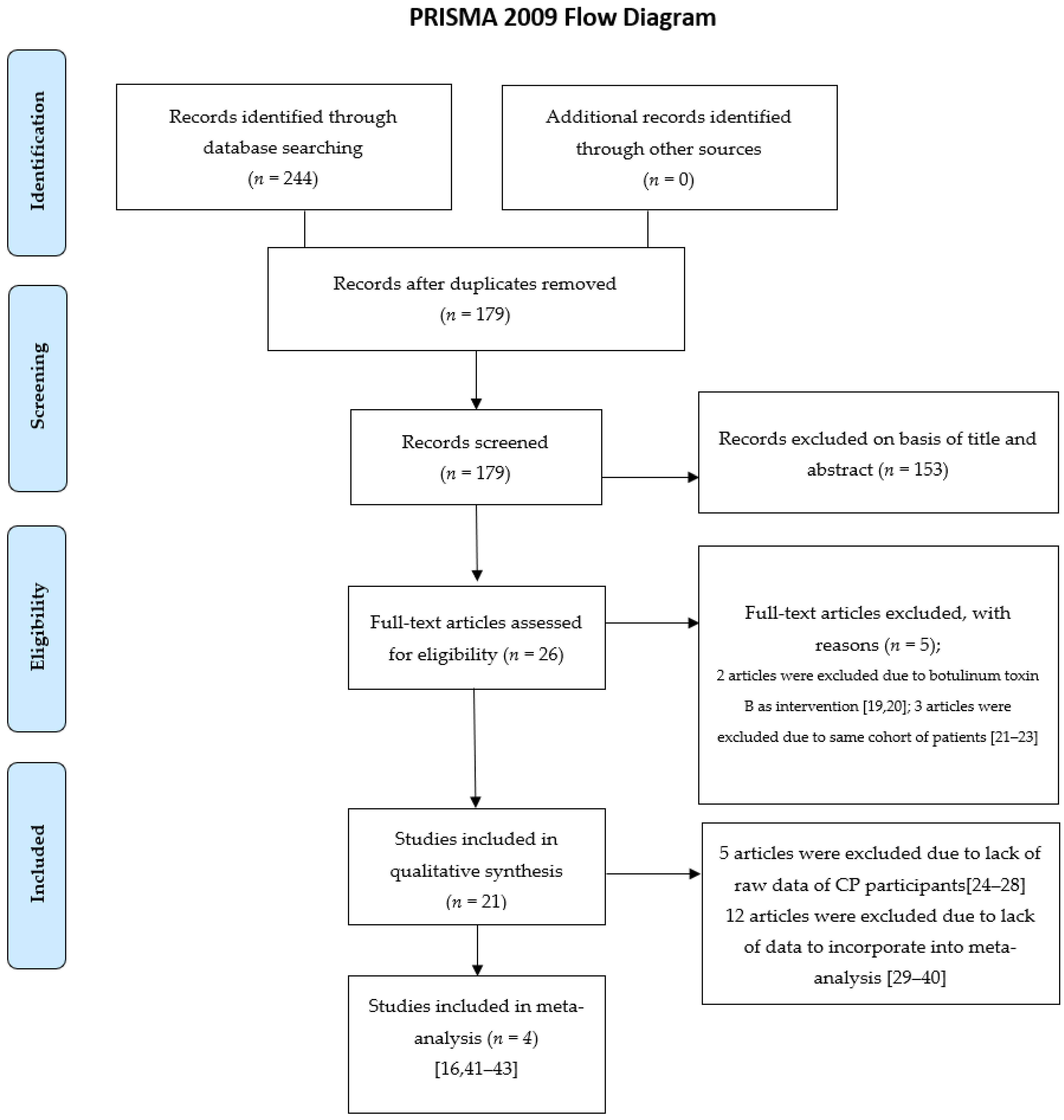
2.3. Study Selection
2.4. Quality Assessment
2.5. Data Extraction
2.6. Data Synthesis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BoNT | botulinum toxin |
| BoNT-A | botulinum neurotoxin type A |
| BoNT-B | botulinum neurotoxin type B |
| CI | confidence interval |
| CP | cerebral palsy |
| DFSS | Drooling Frequency and Severity Scale |
| DQ | Drooling Quotient |
| RCT | randomized controlled trial |
| SMD | standard difference in means |
References
- Van De Heyning, P.H.; Marquet, J.F.; Creten, W.L. Drooling in children with cerebral palsy. Acta Oto-Rhino-Laryngol. Belg. 1980, 34, 691–705. [Google Scholar]
- Koheil, R.; Sochaniwskyj, A.E.; Bablich, K.; Kenny, D.J.; Milner, M. Biofeedback techniques and behaviour modification in the conservative remediation of drooling by children with cerebral palsy. Dev. Med. Child Neurol. 1987, 29, 19–26. [Google Scholar] [CrossRef]
- Camp-Bruno, J.A.; Winsberg, B.G.; Green-Parsons, A.R.; Abrams, J.P. Efficacy of benztropine therapy for drooling. Dev. Med. Child Neurol. 1989, 31, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Crysdale, W.S. Management options for the drooling patient. Ear Nose Throat J. 1989, 68, 825–826. [Google Scholar]
- Siegel, L.K.; Klingbeil, M.A. Control of drooling with transdermal scopolamine in a child with cerebral palsy. Dev. Med. Child Neurol. 1991, 33, 1013–1014. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.; Kao, C.P. Drooling in children. Paediatr. Child Health 1999, 4, 406–411. [Google Scholar] [CrossRef]
- McInerney, M.S.; Reddihough, D.S.; Carding, P.N.; Swanton, R.; Walton, C.M.; Imms, C. Behavioural interventions to treat drooling in children with neurodisability: A systematic review. Dev. Med. Child Neurol. 2019, 61, 39–48. [Google Scholar] [CrossRef] [Green Version]
- Greensmith, A.L.; Johnstone, B.R.; Reid, S.M.; Hazard, C.J.; Johnson, H.M.; Reddihough, D.S. Prospective analysis of the outcome of surgical management of drooling in the pediatric population: A 10-year experience. Plast. Reconstr. Surg. 2005, 116, 1233–1242. [Google Scholar] [CrossRef] [PubMed]
- Scaglione, F. Conversion Ratio between Botox®, Dysport®, and Xeomin® in Clinical Practice. Toxins 2016, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.J.; Dashtipour, K. Abo-, inco-, ona-, and rima-botulinum toxins in clinical therapy: A primer. Pharmacotherapy 2013, 33, 304–318. [Google Scholar] [CrossRef]
- Marchetti, A.; Magar, R.; Findley, L.; Larsen, J.P.; Pirtosek, Z.; Růzicka, E.; Jech, R.; Sławek, J.; Ahmed, F. Retrospective evaluation of the dose of Dysport and BOTOX in the management of cervical dystonia and blepharospasm: The REAL DOSE study. Mov. Disord. Off. J. Mov. Disord. Soc. 2005, 20, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Wohlfarth, K.; Göschel, H.; Frevert, J.; Dengler, R.; Bigalke, H. Botulinum A toxins: Units versus units. Naunyn-Schmiedebergs Arch. Pharmacol. 1997, 355, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Dashtipour, K.; Chen, J.J.; Espay, A.J.; Mari, Z.; Ondo, W. OnabotulinumtoxinA and AbobotulinumtoxinA Dose Conversion: A Systematic Literature Review. Mov. Disord. Clin. Pract. 2016, 3, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Fehlings, D.; Novak, I.; Berweck, S.; Hoare, B.; Stott, N.S.; Russo, R.N. Botulinum toxin assessment, intervention and follow-up for paediatric upper limb hypertonicity: International consensus statement. Eur. J. Neurol. 2010, 17, 38–56. [Google Scholar] [CrossRef]
- Love, S.C.; Novak, I.; Kentish, M.; Desloovere, K.; Heinen, F.; Molenaers, G.; O’Flaherty, S.; Graham, H.K. Botulinum toxin assessment, intervention and after-care for lower limb spasticity in children with cerebral palsy: International consensus statement. Eur. J. Neurol. 2010, 17, 9–37. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Shieh, J.Y.; Cheng, M.L.; Yang, P.Y. Botulinum toxin type A for control of drooling in Asian patients with cerebral palsy. Neurology 2008, 70, 316–318. [Google Scholar] [CrossRef]
- Reddihough, D.; Erasmus, C.E.; Johnson, H.; McKellar, G.M.; Jongerius, P.H. Botulinum toxin assessment, intervention and aftercare for paediatric and adult drooling: International consensus statement. Eur. J. Neurol. 2010, 17, 109–121. [Google Scholar] [CrossRef]
- Rodwell, K.; Edwards, P.; Ware, R.S.; Boyd, R. Salivary gland botulinum toxin injections for drooling in children with cerebral palsy and neurodevelopmental disability: A systematic review. Dev. Med. Child Neurol. 2012, 54, 977–987. [Google Scholar] [CrossRef]
- Basciani, M.; Di Rienzo, F.; Fontana, A.; Copetti, M.; Pellegrini, F.; Intiso, D. Botulinum toxin type B for sialorrhoea in children with cerebral palsy: A randomized trial comparing three doses. Dev. Med. Child Neurol. 2011, 53, 559–564. [Google Scholar] [CrossRef]
- Wilken, B.; Aslami, B.; Backes, H. Successful treatment of drooling in children with neurological disorders with botulinum toxin A or B. Neuropediatrics 2008, 39, 200–204. [Google Scholar] [CrossRef]
- Jongerius, P.H.; van den Hoogen, F.J.; van Limbeek, J.; Gabreëls, F.J.; van Hulst, K.; Rotteveel, J.J. Effect of botulinum toxin in the treatment of drooling: A controlled clinical trial. Pediatrics 2004, 114, 620–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erasmus, C.E.; Van Hulst, K.; Van Den Hoogen, F.J.; Van Limbeek, J.; Roeleveld, N.; Veerman, E.C.; Rotteveel, J.J.; Jongerius, P.H. Thickened saliva after effective management of drooling with botulinum toxin A. Dev. Med. Child Neurol. 2010, 52, e114–e118. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, A.R.; Erasmus, C.; Van Hulst, K.; van Limbeek, J.; Rotteveel, J.J.; Jongerius, P.H.; van den Hoogen, F.J. Botulinum toxin versus submandibular duct relocation for severe drooling. Dev. Med. Child Neurol. 2010, 52, 1038–1042. [Google Scholar] [CrossRef] [PubMed]
- Gubbay, A.; Marie Blackmore, A. Effects of salivary gland botulinum Toxin-A on drooling and respiratory morbidity in children with neurological dysfunction. Int. J. Pediatr. Otorhinolaryngol. 2019, 124, 124–128. [Google Scholar] [CrossRef]
- Scheffer, A.R.; Erasmus, C.; van Hulst, K.; van Limbeek, J.; Jongerius, P.H.; van den Hoogen, F.J. Efficacy and duration of botulinum toxin treatment for drooling in 131 children. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 873–877. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.H.; Liang, C.; Wilson, P.; Higgins, D.; Allen, G.C. Long-term safety and efficacy data on botulinum toxin type A: An injection for sialorrhea. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Khan, W.U.; Campisi, P.; Nadarajah, S.; Shakur, Y.A.; Khan, N.; Semenuk, D.; McCann, C.; Roske, L.; McConney-Ellis, S.; Joseph, M.; et al. Botulinum toxin A for treatment of sialorrhea in children: An effective, minimally invasive approach. Arch. Otolaryngol. Head Neck Surg. 2011, 137, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Jongerius, P.H.; Rotteveel, J.J.; van Limbeek, J.; Gabreëls, F.J.; van Hulst, K.; van den Hoogen, F.J. Botulinum toxin effect on salivary flow rate in children with cerebral palsy. Neurology 2004, 63, 1371–1375. [Google Scholar] [CrossRef] [PubMed]
- Suskind, D.L.; Tilton, A. Clinical study of botulinum-A toxin in the treatment of sialorrhea in children with cerebral palsy. Laryngoscope 2002, 112, 73–81. [Google Scholar] [CrossRef]
- Savarese, R.; Diamond, M.; Elovic, E.; Millis, S.R. Intraparotid injection of botulinum toxin A as a treatment to control sialorrhea in children with cerebral palsy. Am. J. Phys. Med. Rehabil. 2004, 83, 304–311. [Google Scholar] [CrossRef]
- Erasmus, C.E.; Scheffer, A.R.; van Hulst, K.; van Limbeek, J.; van den Hoogen, F.J.; Rotteveel, J.J.; Jongerius, P.H. Does motor performance matter in botulinum toxin efficacy for drooling? Pediatr. Neurol. 2011, 45, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, N.; Penn, C. Botox(®) to reduce drooling in a paediatric population with neurological impairments: A Phase I study. Int. J. Lang. Commun. Disord. 2011, 46, 550–563. [Google Scholar] [CrossRef]
- Wu, K.P.; Ke, J.Y.; Chen, C.Y.; Chen, C.L.; Chou, M.Y.; Pei, Y.C. Botulinum toxin type A on oral health in treating sialorrhea in children with cerebral palsy: A randomized, double-blind, placebo-controlled study. J. Child Neurol. 2011, 26, 838–843. [Google Scholar] [CrossRef]
- Nordgarden, H.; Østerhus, I.; Møystad, A.; Asten, P.; Johnsen, U.L.; Storhaug, K.; Loven, J. Drooling: Are botulinum toxin injections into the major salivary glands a good treatment option? J. Child Neurol. 2012, 27, 458–464. [Google Scholar] [CrossRef]
- Tiigimäe-Saar, J.; Leibur, E.; Kolk, A.; Talvik, I.; Tamme, T. Use of botulinum neurotoxin A in uncontrolled salivation in children with cerebral palsy: A pilot study. Int. J. Oral Maxillofac. Surg. 2012, 41, 1540–1545. [Google Scholar] [CrossRef] [PubMed]
- Sidebottom, A.J.; May, J.E.; Madahar, A.K. Role of botulinum toxin A injection into the submandibular salivary glands as an assessment for the subsequent removal of the submandibular glands in the management of children with sialorrhoea. Br. J. Oral Maxillofac. Surg. 2013, 51, 113–116. [Google Scholar] [CrossRef]
- Møller, E.; Pedersen, S.A.; Vinicoff, P.G.; Bardow, A.; Lykkeaa, J.; Svendsen, P.; Bakke, M. Onabotulinumtoxin A Treatment of Drooling in Children with Cerebral Palsy: A Prospective, Longitudinal Open-Label Study. Toxins 2015, 7, 2481–2493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lungren, M.P.; Halula, S.; Coyne, S.; Sidell, D.; Racadio, J.M.; Patel, M.N. Ultrasound-Guided Botulinum Toxin Type A Salivary Gland Injection in Children for Refractory Sialorrhea: 10-Year Experience at a Large Tertiary Children’s Hospital. Pediatr. Neurol. 2016, 54, 70–75. [Google Scholar] [CrossRef]
- Sürmelioğlu, Ö.; Dağkıran, M.; Tuncer, Ü.; Özdemir, S.; Tarkan, Ö.; Çetik, F.; Kıroğlu, M. The Effectiveness of Botulinum Toxin Type A Injections in the Management of Sialorrhea. Turk. Arch. Otorhinolaryngol. 2018, 56, 111–113. [Google Scholar] [CrossRef]
- Bekkers, S.; Delsing, C.P.; Kok, S.E.; van Hulst, K.; Erasmus, C.E.; Scheffer, A.R.T.; van den Hoogen, F.J.A. Randomized controlled trial comparing botulinum vs surgery for drooling in neurodisabilities. Neurology 2019, 92, e1195–e1204. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, K.J.; Glasson, C.; O’Flaherty, S.J. Parotid and submandibular botulinum toxin A injections for sialorrhoea in children with cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Alrefai, A.H.; Aburahma, S.K.; Khader, Y.S. Treatment of sialorrhea in children with cerebral palsy: A double-blind placebo controlled trial. Clin. Neurol. Neurosurg. 2009, 111, 79–82. [Google Scholar] [CrossRef]
- Ong, L.C.; Wong, S.W.; Hamid, H.A. Treatment of drooling in children with cerebral palsy using ultrasound guided intraglandular injections of botulinum toxin A. J. Pediatr. Neurol. 2009, 7, 141–145. [Google Scholar]
- Rashnoo, P.; Daniel, S.J. Drooling quantification: Correlation of different techniques. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1201–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hulst, K.; Lindeboom, R.; van der Burg, J.; Jongerius, P. Accurate assessment of drooling severity with the 5-min drooling quotient in children with developmental disabilities. Dev. Med. Child Neurol. 2012, 54, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Porcheri, C.; Mitsiadis, T.A. Physiology, Pathology and Regeneration of Salivary Glands. Cells 2019, 8, 976. [Google Scholar] [CrossRef] [Green Version]
- Gok, G.; Cox, N.; Bajwa, J.; Christodoulou, D.; Moody, A.; Howlett, D.C. Ultrasound-guided injection of botulinum toxin A into the submandibular gland in children and young adults with sialorrhoea. Br. J. Oral Maxillofac. Surg. 2013, 51, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Çiftçi, T.; Akıncı, D.; Yurttutan, N.; Akhan, O. US-guided botulinum toxin injection for excessive drooling in children. Diagn. Interv. Radiol. 2013, 19, 56–60. [Google Scholar] [CrossRef]
- Kok, S.E.; van Valenberg, H.; van Hulst, K.; Jongerius, P.; Erasmus, C.E.; van den Hoogen, F.J.A. Submandibular gland botulinum neurotoxin A injection for predicting the outcome of submandibular duct relocation in drooling: A retrospective cohort study. Dev. Med. Child Neurol. 2019, 61, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.; Mace, A.; Nouraei, S.A.; Sandhu, G. Botulinum toxin in the management of sialorrhoea: A systematic review. Clin. Otolaryngol. 2006, 31, 267–272. [Google Scholar] [CrossRef]
- Cardona, I.; Saint-Martin, C.; Daniel, S.J. Effect of recurrent onabotulinum toxin A injection into the salivary glands: An ultrasound measurement. Laryngoscope 2015, 125, E328–E332. [Google Scholar] [CrossRef] [PubMed]
- Petracca, M.; Guidubaldi, A.; Ricciardi, L.; Ialongo, T.; Del Grande, A.; Mulas, D.; Di Stasio, E.; Bentivoglio, A.R. Botulinum Toxin A and B in sialorrhea: Long-term data and literature overview. Toxicon 2015, 107, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Guidubaldi, A.; Fasano, A.; Ialongo, T.; Piano, C.; Pompili, M.; Mascianà, R.; Siciliani, L.; Sabatelli, M.; Bentivoglio, A.R. Botulinum toxin A versus B in sialorrhea: A prospective, randomized, double-blind, crossover pilot study in patients with amyotrophic lateral sclerosis or Parkinson’s disease. Mov. Disord. 2011, 26, 313–319. [Google Scholar] [CrossRef]
- An, J.S.; Hyun Won, C.; Si Han, J.; Park, H.S.; Seo, K.K. Comparison of onabotulinumtoxinA and rimabotulinumtoxinB for the treatment of axillary hyperhidrosis. Dermatol. Surg. 2015, 41, 960–967. [Google Scholar] [CrossRef]
- Blitzer, A. Botulinum toxin A and B: A comparative dosing study for spasmodic dysphonia. Otolaryngol. Head Neck Surg. 2005, 133, 836–838. [Google Scholar] [CrossRef] [PubMed]
- Kranz, G.; Paul, A.; Voller, B.; Posch, M.; Windischberger, C.; Auff, E.; Sycha, T. Long-term efficacy and respective potencies of botulinum toxin A and B: A randomized, double-blind study. Br. J. Dermatol. 2011, 164, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Ondo, W.G.; Hunter, C.; Moore, W. A double-blind placebo-controlled trial of botulinum toxin B for sialorrhea in Parkinson’s disease. Neurology 2004, 62, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Dashtipour, K.; Bhidayasiri, R.; Chen, J.J.; Jabbari, B.; Lew, M.; Torres-Russotto, D. RimabotulinumtoxinB in sialorrhea: Systematic review of clinical trials. J. Clin. Mov. Disord. 2017, 4, 9. [Google Scholar] [CrossRef]
- Dressler, D.; Bigalke, H. Botulinum toxin type B de novo therapy of cervical dystonia: Frequency of antibody induced therapy failure. J. Neurol. 2005, 252, 904–907. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Hunter, C.; Dolimbek, B.Z.; Dolimbek, G.S.; Adler, C.H.; Brashear, A.; Comella, C.L.; Gordon, M.; Riley, D.E.; Sethi, K.; et al. Clinico-immunologic aspects of botulinum toxin type B treatment of cervical dystonia. Neurology 2006, 67, 2233–2235. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Study | Treatment (n) | Mean Age, y (range) | Diagnosis | Injection Type and Dose | Ultrasound Guidance | Site | Registration Number of RCT |
|---|---|---|---|---|---|---|---|
| Randomized control trials | |||||||
| Lin et al., 2008 [16] | 13 | 14.2 | CP | Botox, 2 U/kg/gland | Y | One PG and the contralateral SMG gland | NCT00173745 |
| Alrefai et al., 2009 [42] | 24 | 3.5 (1.75–7) | CP | Dysport, 100 U | N | Bil. PG | Not provided |
| Wu et al., 2011 [33] | 20 | 3–16 | CP | Botox, 30–50 U | Y | Bil. PG and SMG | Not provided |
| Nordgarden et al., 2012 [34] | 6 | 13.7 (10–18) | CP | Botox, 25 U/gland | Y | Bil. PG and SMG | Not provided |
| Bekkers et al., 2019 [40] | 26 | 11 | CP DD | Botox 25 U/gland | Y | Bil. SMG | NTR3537 |
| Observational studies | |||||||
| Suskind et al., 2002 [29] | 22 | 8–21 | CP | Botox, 10–70 U | Y | Bil. PG and SMG | |
| Jongerius et al., 2004 [28] | 45 | 9.5 (3–16) | CP | Botox, 30–50 U | Y | Bil. SMG | |
| Savarese et al., 2004 [30] | 21 | 5–18 | CP | Botox, 15 U/gland | N | Bil. SMG | |
| Banerjee et al., 2006 [41] | 19 | 10.8 (6–16) | CP | Botox, 2 U/kg, max 70 U | Y | Bil. PG and SMG | |
| Ong et al., 2009 [43] | 21 | 8.4 (4–12) | CP | Botox, 60–80 U | Y | Bil. PG and SMG | |
| Scheffer et al., 2010 [23] | 131 | 10.9 | CP PR | Botox, 30–50 U | Y | Bil. SMG | |
| Khan et al., 2010 [27] | 45 | 10.5 | CP Other | Botox, max 5 U/kg | Y | Bil. PG and SMG | |
| Erasmus et al., 2011 [31] | 126 | 10 y 11 m | CP ID | Botox, 50 U | Y | Bil. SMG | |
| Nicola et al., 2011 [32] | 9 | 9.3 (5–17) | CP OS | Botox, 30–50 U | N | Bil. PG and SMG | |
| Tiigimäe-Saar et al., 2012 [35] | 12 | 1.6–11 | CP | Botox, 2 U/kg | Y | Bil. PG and SMG | |
| Sidebottom et al., 2013 [36] | 30 | 11 (4–17) | CP NS | Dysport, 1 U/kg/gland | Y | Bil. SMG | |
| Chan et al., 2013 [26] | 69 | 9.5 | CP Other | BoNT A a, 8 U/kg | Y | Bil. PG and SMG | |
| Møller et al., 2015 [37] | 14 | 9 | CP | Botox, 20–120 U | Y | Bil. PG and SMG | |
| Matthew et al., 2016 [38] | 111 | 7 | CP NS | Botox, 100 U | Y | Bil. PG and SMG | |
| Sürmelioğlu et al., 2018 [39] | 27 | 11.5 (6–16) | CP | Botox, 60 U | N | Bil. PG and SMG | |
| Gubbay et al., 2019 [24] | 15 | 9.9 (3–14) | CP Other | Botox, 1 unit/kg/gland, max: 100 U | Y | Bil. PG and SMG | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, S.-A.; Liao, C.-L.; Lin, W.-P.; Hsu, J.C.; Guo, Y.-H.; Lin, Y.-C. Botulinum Toxin Injections for Treatment of Drooling in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis. Children 2021, 8, 1089. https://doi.org/10.3390/children8121089
Hung S-A, Liao C-L, Lin W-P, Hsu JC, Guo Y-H, Lin Y-C. Botulinum Toxin Injections for Treatment of Drooling in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis. Children. 2021; 8(12):1089. https://doi.org/10.3390/children8121089
Chicago/Turabian StyleHung, Shang-An, Chung-Lun Liao, Wei-Pin Lin, Jason C. Hsu, Yao-Hong Guo, and Yu-Ching Lin. 2021. "Botulinum Toxin Injections for Treatment of Drooling in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis" Children 8, no. 12: 1089. https://doi.org/10.3390/children8121089
APA StyleHung, S.-A., Liao, C.-L., Lin, W.-P., Hsu, J. C., Guo, Y.-H., & Lin, Y.-C. (2021). Botulinum Toxin Injections for Treatment of Drooling in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis. Children, 8(12), 1089. https://doi.org/10.3390/children8121089