
The Effect of the ‘Touch Screen-Based Cognitive Training’ for Children with Severe Cognitive Impairment in Special Education


Abstract
:1. Introduction
2. Materials and Methods
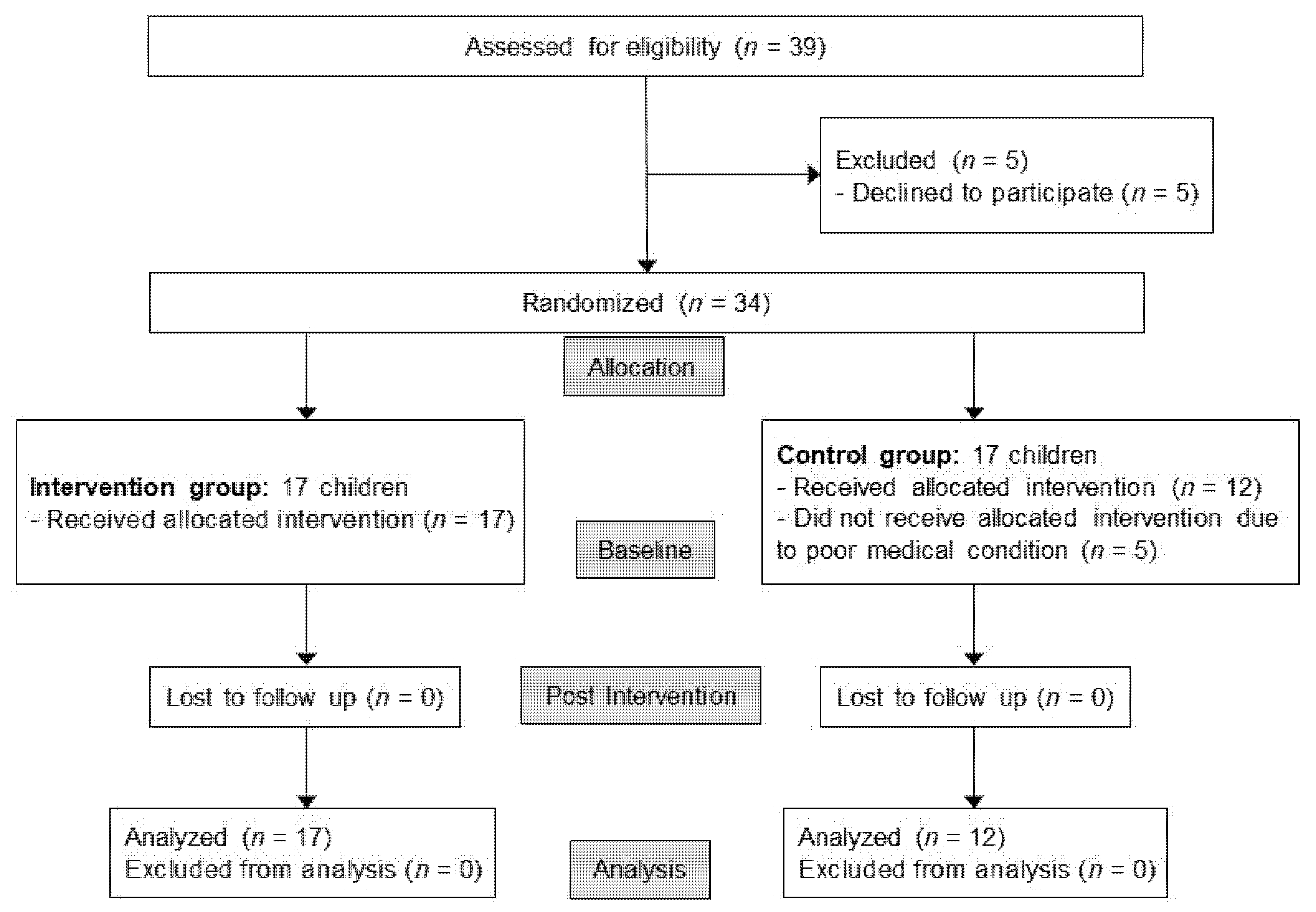
2.1. Study Design and Participants
2.2. Randomization and Blinding
2.3. Interventions
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Children and Applicability of the ‘Touch Screen-Based Cognitive Training’ in Special Education
3.2. Comparison of the Measurements within and between the Two Groups
3.3. The Efficacy of the ‘Touch Screen-Based Cognitive Training’ Considering the Severeness of Developmental Delay
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kurtz, M.M. Symptoms versus neurocognitive skills as correlates of everyday functioning in severe mental illness. Expert Rev. Neurother. 2006, 6, 47–56. [Google Scholar] [CrossRef]
- Forrest, C.B.; Bevans, K.B.; Riley, A.W.; Crespo, R.; Louis, T.A. School outcomes of children with special health care needs. Pediatrics 2011, 128, 303–312. [Google Scholar] [CrossRef] [Green Version]
- Sung, I.Y.; Jeon, J.Y.; Yun, K.J.; Yuk, J.S.; Byun, E.M.; Yoo, H.W.; Ko, T.S.; Kim, H.W.; Jang, D.H. Development of tablet personal computer-based cognitive training programs for children with developmental disabilities whose cognitive age is less than 4 years. Medicine (Baltimore) 2020, 99, e18674. [Google Scholar] [CrossRef] [PubMed]
- Ko, E.J.; Sung, I.Y.; Yuk, J.S.; Jang, D.H.; Yun, G. A tablet computer-based cognitive training program for young children with cognitive impairment: A randomized controlled trial. Medicine (Baltimore) 2020, 99, e19549. [Google Scholar] [CrossRef] [PubMed]
- Bennett, S.J.; Holmes, J.; Buckley, S. Computerized memory training leads to sustained improvement in visuospatial short-term memory skills in children with Down syndrome. Am. J. Intellect. Dev. Disabil. 2013, 118, 179–192. [Google Scholar] [CrossRef]
- Putnam, S.P.; Gartstein, M.A.; Rothbart, M.K. Measurement of fine-grained aspects of toddler temperament: The early childhood behavior questionnaire. Infant Behav. Dev. 2006, 29, 386–401. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.T.; Kim, K.H.; Yoon, H.R.; Kim, W.S. Yeong Yua Eoneobaldal Geomsa [Sequenced Language Scale for Infants (SELSI)], 1st ed.; Special Education Publication Co.: Seoul, Korea, 2003. [Google Scholar]
- Haley, S.M.; Coster, W.J.; Ludlow, L.H.; Haltiwanger, J.T.; Andrellos, P.J. Pediatric Evaluation of Disability Inventory (PEDI); New England Medical Central Hospitals/PEDI Research Group: Boston, MA, USA, 1992. [Google Scholar]
- Steenbeek, D.; Meester-Delver, A.; Becher, J.G.; Lankhorst, G.J. The effect of botulinum toxin type A treatment of the lower extremity on the level of functional abilities in children with cerebral palsy: Evaluation with goal attainment scaling. Clin. Rehabil. 2005, 19, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Schopler, E.; Reichler, R.J.; Bashford, A.; Lansing, M.D.; Marcus, L. Psychoeducational Profile Revised (PEP-R); Pro-Ed: Austin, TX, USA, 1990. [Google Scholar]
- Martin, E.W.; Martin, R.; Terman, D.L. The legislative and litigation history of special education. Future Child. 1996, 6, 25–39. [Google Scholar] [CrossRef] [Green Version]
- Dalton, M.A. Education rights and the special needs child. Child Adolesc. Psychiatr. Clin. N. Am. 2002, 11, 859–868. [Google Scholar] [CrossRef]
- Van Someren, M.W.; Reimann, P.; Boshuizen, H.P.A.; de Jong, T. Learning with Multiple Representations; Pergamon: Amsterdam, The Netherlands, 1998. [Google Scholar]
- Mayer, R.E.; Sims, V.K. For whom is a picture worth a thousand words? Extensions of a dual-coding theory of multimedia learning. J. Educ. Psychol. 1994, 86, 389–401. [Google Scholar] [CrossRef]
- Clark, J.M.; Paivio, A. Dual coding theory and education. Educ. Psychol. Rev. 1991, 3, 149–210. [Google Scholar] [CrossRef] [Green Version]
- Schnotz, W.; Bannert, M. Construction and interference in learning from multiple representation. Learn. Instr. 2003, 13, 141–156. [Google Scholar] [CrossRef]
- Klingberg, T.; Fernell, E.; Olesen, P.J.; Johnson, M.; Gustafsson, P.; Dahlström, K.; Gillberg, C.G.; Forssberg, H.; Westerberg, H. Computerized training of working memory in children with ADHD-a randomized, controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Mezzacappa, E.; Buckner, J.C. Working memory training for children with attention problems or hyperactivity: A school-based pilot study. School Ment. Health 2010, 2, 202–208. [Google Scholar] [CrossRef]
- Steiner, N.J.; Sheldrick, R.C.; Gotthelf, D.; Perrin, E.C. Computer-based attention training in the schools for children with attention deficit/hyperactivity disorder: A preliminary trial. Clin. Pediatr. (Phila) 2011, 50, 615–622. [Google Scholar] [CrossRef]
- Kirk, H.E.; Spencer-Smith, M.; Wiley, J.F.; Cornish, K.M. Gamified attention training in the primary school classroom: A cluster-randomized controlled trial. J. Atten. Disord. 2021, 25, 1146–1159. [Google Scholar] [CrossRef] [PubMed]
- Merzenich, M.M.; Jenkins, W.M.; Johnston, P.; Schreiner, C.; Miller, S.L.; Tallal, P. Temporal processing deficits of language-learning impaired children ameliorated by training. Science 1996, 271, 77–81. [Google Scholar] [CrossRef] [Green Version]
- Bosseler, A.; Massaro, D.W. Development and evaluation of a computer-animated tutor for vocabulary and language learning in children with autism. J. Autism Dev. Disord. 2003, 33, 653–672. [Google Scholar] [CrossRef]
- Heimann, M.; Nelson, K.E.; Tjus, T.; Gillberg, C. Increasing reading and communication skills in children with autism through an interactive multimedia computer program. J. Autism Dev. Disord. 1995, 25, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Meara, E.R.; Richards, S.; Cutler, D.M. The gap gets bigger: Changes in mortality and life expectancy, by education, 1981–2000. Health Aff. (Millwood) 2008, 27, 350–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donohue, J.M.; Miller, E. COVID-19 and school closures. JAMA 2020, 324, 845–847. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Main Cognitive Targets | |
|---|---|
| Adaptive programs | |
| Puzzles | Attention, Visuospatial function, Language, Eye-hand coordination |
| Hidden object games | Attention, Memory, Visuospatial function, Executive function, Language |
| Animal matching | Attention, Visuospatial function, Executive function, Language |
| Pattern matching | Attention, Executive function |
| Identical image identification | Attention, Visuospatial function, Eye-hand coordination |
| Memory games | Attention, Memory, Executive function |
| Non-adaptive programs | |
| Tracing | Attention, Visuospatial function, Language, Eye-hand coordination |
| Object matching | Attention |
| Sound matching | Attention, Memory, Language, Auditory cognition |
| Balloon games | Attention, Memory, Visuospatial function, Language, Eye-hand coordination |
| Farm games | Attention |
| Daily activity games | Attention |
| Intervention Group (n = 17) | Control Group (n = 12) | p-Value | |
|---|---|---|---|
| Age (months) | 140.1 ± 49.1 | 143.6 ± 60.3 | 0.98 |
| Sex (Male:Female) | 9:8 | 10:2 | 0.13 |
| Diagnosis (ID:ASD) | 12:5 | 8:4 | 1.00 |
| PEP-R (Developmental score) | 61.6 ± 12.5 | 59.6 ± 9.6 | 0.66 |
| PEP-R (Developmental age) | 24.1 ± 8.5 | 22.8 ± 6.5 | 0.67 |
| ECBQ (Attentional focusing) | 41.1 ± 15.0 | 37.8 ± 7.3 | 0.49 |
| ECBQ (Attentional shifting) | 46.5 ± 12.4 | 35.2 ± 12.7 | 0.88 |
| SELSI (Comprehension, raw score) | 36.8 ± 13.4 | 34.3 ± 13.7 | 0.64 |
| SELSI (Comprehension, age) | 20.0 ± 7.1 | 18.6 ± 7.1 | 0.61 |
| SELSI (Expression, raw score) | 25.7 ± 13.1 | 19.2 ± 7.3 | 0.13 |
| SELSI (Expression, age) | 15.4 ± 8.2 | 11.4 ± 3.9 | 0.13 |
| PEDI (Self-care) | 47.0 ± 12.6 | 39.8 ± 16.3 | 0.13 |
| PEDI (Mobility) | 50.1 ± 13.2 | 47.1 ± 14.9 | 0.42 |
| PEDI (Social function) | 26.8 ± 6.2 | 24.7 ± 9.2 | 0.46 |
| GAS | −2.0 ± 0.0 | −2.0 ± 0.0 | 1.00 |
| Variables | Time | Intervention Group (n=17) | Control Group (n = 12) | p-Value (Group × Time) | p-Value (Group) | p-Value (Time) |
|---|---|---|---|---|---|---|
| PEP-R (Developmental score) | Pre | 61.6 ± 12.5 | 59.6 ± 9.6 | 0.07 | 0.30 | <0.001 * |
| Post | 71.2 ± 13.7 | 63.5 ± 12.1 | ||||
| PEP-R (Developmental age) | Pre | 24.1 ± 8.5 | 22.8 ± 6.5 | 0.07 | 0.30 | <0.001 * |
| Post | 30.7 ± 9.3 | 25.5 ± 8.1 | ||||
| ECBQ (Attentional focusing) | Pre | 41.1 ± 15.0 | 37.8 ± 7.3 | 0.16 | 0.31 | 0.003 * |
| Post | 45.5 ± 14.0 | 39.5 ± 7.8 | ||||
| ECBQ (Attentional shifting) | Pre | 46.5 ± 12.4 | 35.2 ± 12.7 | 0.88 | 0.005 * | 0.004 * |
| Post | 52.0 ± 9.9 | 40.2 ± 7.2 | ||||
| SELSI (Comprehension, raw score) | Pre | 36.8 ± 13.4 | 34.3 ± 13.7 | 0.22 | 0.33 | 0.002 * |
| Post | 44.1 ± 9.3 | 37.7 ± 12.7 | ||||
| SELSI (Comprehension, age) | Pre | 20.0 ± 7.1 | 18.6 ± 7.1 | 0.21 | 0.29 | 0.003 * |
| Post | 23.8 ± 4.9 | 20.3 ± 6.5 | ||||
| SELSI (Expression, raw score) | Pre | 25.7 ± 13.1 | 19.2 ± 7.3 | 0.12 | 0.08 | <0.001 * |
| Post | 30.6 ± 14.8 | 21.3 ± 7.6 | ||||
| SELSI (Expression, age) | Pre | 15.4 ± 8.2 | 11.4 ± 3.9 | 0.60 | 0.08 | 0.03 * |
| Post | 17.3 ± 7.8 | 12.6 ± 4.0 | ||||
| PEDI (Self-care) | Pre | 47.0 ± 12.6 | 39.8 ± 16.3 | 0.13 | 0.24 | 0.002 * |
| Post | 51.5 ± 13.1 | 43.0 ± 16.4 | ||||
| PEDI (Mobility) | Pre | 50.1 ± 13.2 | 47.1 ± 14.9 | 0.89 | 0.56 | 0.14 |
| Post | 50.8 ± 13.4 | 47.7 ± 15.2 | ||||
| PEDI (Social function) | Pre | 26.8 ± 6.2 | 24.7 ± 9.2 | 0.13 | 0.24 | 0.002 * |
| Post | 30.7 ± 7.0 | 26.2 ± 8.5 | ||||
| GAS | Pre | −2.0 ± 0.0 | −2.0 ± 0.0 | 0.03 * | 0.03 * | <0.001 * |
| Post | 0.0 ± 1.4 | 1.1 ± 1.1 |
| Beta | SE | p-Value | 95% CI | |
|---|---|---|---|---|
| PEP-R (Developmental score) | −5.957 | 3.095 | 0.066 | −12.344–0.430 |
| PEP-R (Developmental age) | −4.045 | 2.093 | 0.065 | −8.364–0.275 |
| ECBQ (Attentional focusing) | −3.161 | 1.830 | 0.096 | −6.923–0.601 |
| ECBQ (Attentional shifting) | −6.132 | 2.649 | 0.029 * | −11.576–−0.687 |
| SELSI (Comprehension, raw score) | −4.858 | 2.590 | 0.072 | −10.192–0.475 |
| SELSI (Comprehension, age) | −2.673 | 1.362 | 0.061 | −5.477–0.132 |
| SELSI (Expression, raw score) | −2.543 | 1.842 | 0.180 | −6.388–1.251 |
| SELSI (Expression, age) | −1.415 | 1.324 | 0.295 | −4.141–1.311 |
| PEDI (Self-care) | −1.822 | 2.279 | 0.431 | −6.507–2.863 |
| PEDI (Mobility) | −0.106 | 0.862 | 0.903 | −1.879–1.666 |
| PEDI (Social function) | −2.659 | 1.526 | 0.093 | −5.797–0.478 |
| GAS | −1.083 | 0.479 | 0.032 * | −2.068–−0.099 |
| r | p-Value | |
|---|---|---|
| PEP-R (Developmental score) | −0.209 | 0.276 |
| PEP-R (Developmental age) | −0.211 | 0.272 |
| ECBQ (Attentional focusing) | −0.081 | 0.678 |
| ECBQ (Attentional shifting) | −0.161 | 0.404 |
| SELSI (Comprehension, raw score) | 0.036 | 0.855 |
| SELSI (Comprehension, age) | 0.056 | 0.774 |
| SELSI (Expression, raw score) | 0.037 | 0.847 |
| SELSI (Expression, age) | 0.009 | 0.963 |
| PEDI (Self-care) | −0.283 | 0.137 |
| PEDI (Mobility) | 0.065 | 0.739 |
| PEDI (Social function) | −0.036 | 0.855 |
| GAS | 0.019 | 0.922 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, I.Y.; Yuk, J.S.; Jang, D.-H.; Yun, G.; Kim, C.; Ko, E.J. The Effect of the ‘Touch Screen-Based Cognitive Training’ for Children with Severe Cognitive Impairment in Special Education. Children 2021, 8, 1205. https://doi.org/10.3390/children8121205
Sung IY, Yuk JS, Jang D-H, Yun G, Kim C, Ko EJ. The Effect of the ‘Touch Screen-Based Cognitive Training’ for Children with Severe Cognitive Impairment in Special Education. Children. 2021; 8(12):1205. https://doi.org/10.3390/children8121205
Chicago/Turabian StyleSung, In Young, Jin Sook Yuk, Dae-Hyun Jang, Gijeong Yun, Chunye Kim, and Eun Jae Ko. 2021. "The Effect of the ‘Touch Screen-Based Cognitive Training’ for Children with Severe Cognitive Impairment in Special Education" Children 8, no. 12: 1205. https://doi.org/10.3390/children8121205
APA StyleSung, I. Y., Yuk, J. S., Jang, D.-H., Yun, G., Kim, C., & Ko, E. J. (2021). The Effect of the ‘Touch Screen-Based Cognitive Training’ for Children with Severe Cognitive Impairment in Special Education. Children, 8(12), 1205. https://doi.org/10.3390/children8121205