
The Cervico-Parasternal Thoracotomy (CPT): A New Surgical Approach for the Resection of Cervicothoracic Neuroblastomas

 ,
,  and
and
Abstract
:1. Introduction
2. Description of the Operative Technique
2.1. Patient Positioning
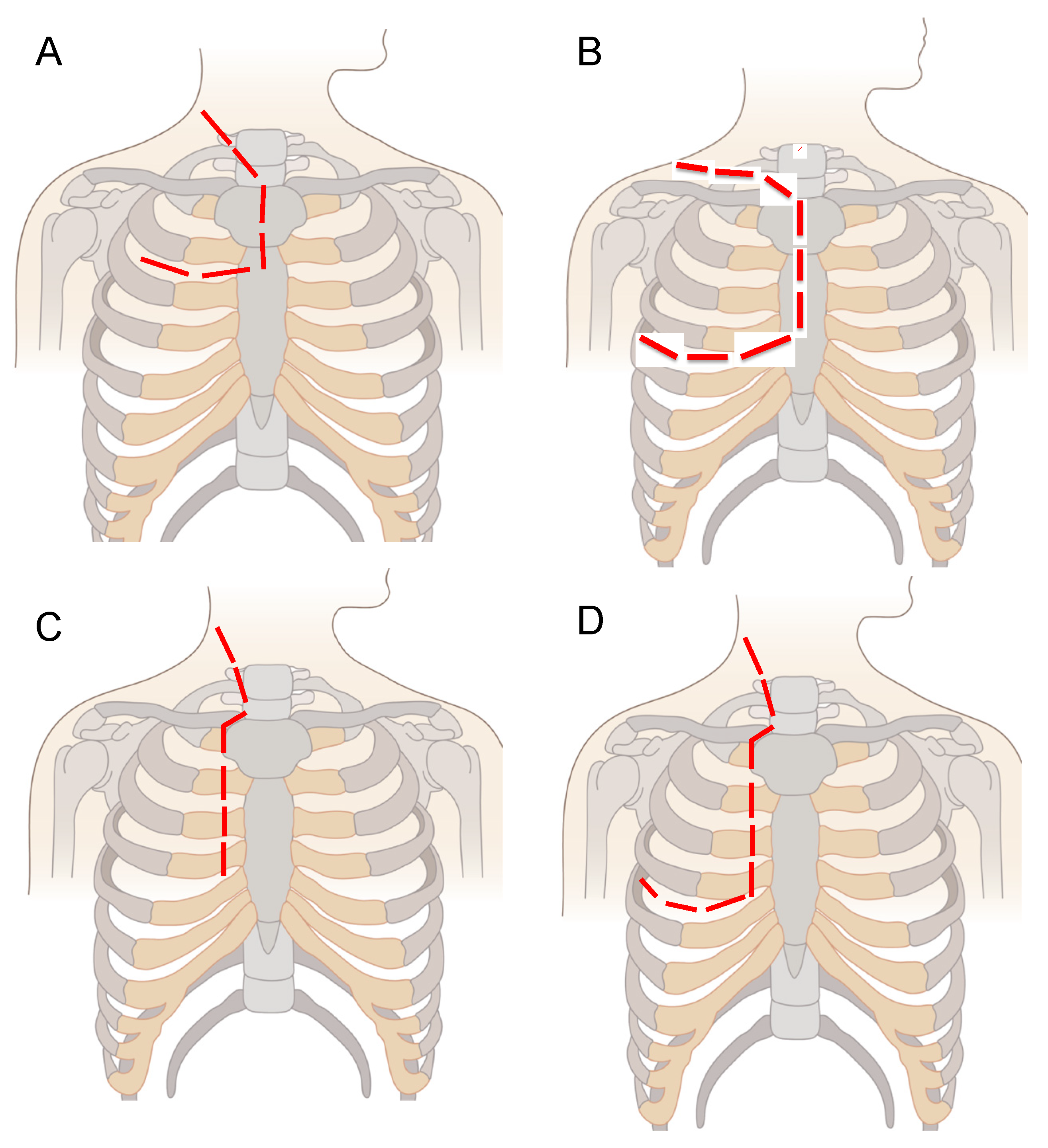
2.2. Surgical Incision
2.3. Thoracic Access
2.4. Tumour Resection
2.5. Surgical Reconstruction and Closure
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haddad, M.; Triglia, J.M.; Helardot, P.; Couanet, D.; Gauthier, F.; Neuenschwander, S.; Bourlière, B.; Bergeron, C.; Munzer, C.; Rubie, H.; et al. Localized cervical neuroblastoma: Prevention of surgical complications. Int. J. Pediatr. Otorhinolaryngol. 2003, 67, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- Chui, C.H.; Thirugnanam, A. Trapdoor anterior thoracotomy for cervicothoracic and apical thoracic neuroblastoma in children. Pediatr. Surg. Int. 2020, 36, 891–895. [Google Scholar] [CrossRef] [PubMed]
- De Corti, F.; Avanzini, S.; Cecchetto, G.; Buffa, P.; Guida, E.; Zanon, G.F.; Jasonni, V. The surgical approach for cervicothoracic masses in children. J. Pediatr. Surg. 2012, 47, 1662–1668. [Google Scholar] [CrossRef] [PubMed]
- El Madi, A.; Irtan, S.; Sauvat, F.; Zérah, M.; Schleiermacher, G.; Galmiche-Roland, L.; Minard-Colin, V.; Brisse, H.; Sarnacki, S. Long-term results of the transmanubrial osteomuscular-sparing approach for pediatric tumors. Pediatr. Blood Cancer 2017, 64, e26527. [Google Scholar] [CrossRef] [PubMed]
- Jones, V.S.; Pitkin, J. Navigating the thoracic inlet in children. Pediatr. Surg. Int. 2007, 24, 491–494. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.V.; Menon, S.; McDowell, D.T.; Yeap, B.; Russell, J.; Corbally, M.T. The use of the trapdoor incision for access to thoracic inlet pathology in children. J. Pediatr. Surg. 2013, 48, 1147–1151. [Google Scholar] [CrossRef] [PubMed]
- Parikh, D.; Short, M.; Eshmawy, M.; Brown, R. Surgical outcome analysis of paediatric thoracic and cervical neuroblastoma. Eur. J. Cardio-Thoracic Surg. 2012, 41, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Pimpalwar, A.P.; Kroeker, T.R.; Ramachandran, V. Cervicothoracic neuroblastoma arising from the stellate ganglion in children: The use of muscle and bone sparing transmanubrial transcostal approach. J. Pediatr. Surg. 2008, 43, e31–e34. [Google Scholar] [CrossRef] [PubMed]
- Pranikoff, T.; Hirschl, R.B.; Schnaufer, L. Approach to cervicothoracic neuroblastomas via a trap-door incision. J. Pediatr. Surg. 1995, 30, 546–548. [Google Scholar] [CrossRef]
- Qureshi, S.S.; Kembhavi, S.; Ramadwar, M.; Chinnaswamy, G.; Laskar, S.; Talole, S.; Desai, S.; Khanna, N.; Vora, T.; Kurkure, P. Outcome and morbidity of surgical resection of primary cervical and cervicothoracic neuroblastoma in children: A comparative analysis. Pediatr. Surg. Int. 2013, 30, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Sauvat, F.; Brisse, H.; Magdeleinat, P.; Lopez, M.; Philippe-Chomette, P.; Orbach, D.; Aerts, I.; Brugieres, L.; Revillon, Y.; Sarnacki, S. The transmanubrial approach: A new operative approach to cervicothoracic neuroblastoma in children. Surgery 2006, 139, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Luksch, R.; Castellani, M.R.; Collini, P.; De Bernardi, B.; Conte, M.; Gambini, C.; Gandola, L.; Garaventa, A.; Biasoni, D.; Podda, M.; et al. Neuroblastoma (Peripheral neuroblastic tumours). Crit. Rev. Oncol. 2016, 107, 163–181. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PATIENT 1 | PATIENT 2 | PATIENT 3 | PATIENT 4 | PATIENT 5 | |
|---|---|---|---|---|---|
| Age at surgery (years) | 11 | 9 | 2 | 2 | 7 |
| Gender | male | female | female | male | male |
| Site | right | right | right | right | right |
| ASA status | 2 | 3 | 3 | 3 | 3 |
| IN Staging System | III | III | III | III | IV |
| INRG Staging System | L2 | L2 | L2 | L2 | M |
| MYCN status | not amplified | not amplified | not amplified | not amplified | amplified |
| Histology | favourable | favourable | favourable | favourable | unfavourable |
| Previous surgery | no | yes (laminectomy D5–D12) | no | no | yes (recurrent NB) |
| Operative time (min) | 240 | 480 | 480 | 370 | 230 |
| RBC transfusion | no | yes | yes | no | yes |
| Hospital stay (days) | 10 | 13 | 14 | 11 | 7 |
| ICU stay (hours) | 24 | 48 | 72 | 96 | 24 |
| Preoperative chemotherapy | no | yes | yes | yes | yes |
| Postoperative therapy | no | no | cis-retinoic acid) | radiotherapy | cis-retinoic acid & immunotherapy comprising anti-GD2 antibody (ch14.18) and IL-2 |
| Postoperative complications | no | no | no | no | no |
| Follow up (months) | 21 | 18 | 13 | 15 | 17 |
| Follow up status | alive, disease-free | alive, disease-free | alive, disease-free | alive, disease-free | alive, disease-free |
| AUTHORS | PATIENTS’ POPULATION | AGE (Average, Range; Months) | SURGICAL APPROACH | OPERATIVE TIME (Average, Range; Minutes) | TUMOUR TYPE | HOSPITAL STAY (Average, Range; Days) | COMPLICATIONS | SURVIVAL OUTCOMES | FOLLOW-UP PERIOD (Average, Range; Months) |
|---|---|---|---|---|---|---|---|---|---|
| Pranikoff T et al., 1995 [9] | 2 | 10.5 (4–17) | Trap-door (n = 2) | nd | Ganglioneuroblastoma (n = 2) | 7.5 (5–10) | None | nd | nd |
| Sauvat F et al., 2006 [11] | 4 | 35 (10–84) | Trans-manubrial (n = 4) | nd | Neuroblastoma (n = 4) | nd | Chylotorax (n = 1); gastroparesis (n = 1); diaphragmatic paresis (n = 2); Bernard–Horner Syndrome (n = 4) | Alive: 4/4 (100.0%); complete remission: 4/4 (100.0%) | nd (8–32) |
| Pimpalwar AP et al., 2007 [8] | 1 | 24 (na) | Trans-manubrial (n = 1) | 160 | Ganglioneuroblastoma (n = 1) | 2 | Bernard–Horner Syndrome (n = 1) | Alive: 1/1 (100.0%); complete remission: 1/1 (100.0%) | 6 (na) |
| Jones vs. et al., 2008 [5] | 1 | 42 (na) | Trap-door (n = 1) | nd | Ganglioneuroma (n = 1) | nd | Bernard–Horner Syndrome (n = 1) | Alive: 1/1 (100.0%); complete remission: 1/1 (100.0%) | 3 (na) |
| Parikh D et al., 2011 [7] | 3 | 24 (nd) | Trap-door (n = 3) | nd | Neuroblastoma (n = 4) | nd | nd | Alive: 2/3 (66.7%); complete remission: 2/3 (66.7%) | 57.3 (16–96) |
| De Corti et al., 2012 [3] | 8 | 45.6 (nd) | Trans-manubrial (n = 6); trap-door (n = 2) | 263.8 (140–410) | Neuroblastoma (n = 5); ganglioneuroblastoma (n = 3) | 11.9 (9–26) | Chylotorax (n = 1); hemothorax (n = 1); Bernard–Horner Syndrome (n = 3) | Alive: 8/8 (100.0%); complete remission: 7/8 (87.5%) | 24 |
| McMahon et al., 2013 [6] | 1 | 48 (na) | Trap-door (n = 1) | nd | Ganglioneuroblastoma (n = 1) | nd | Bernard–Horner Syndrome | Alive: 1/1 (100.0%); complete remission: 1/1 (100.0%) | 60 |
| Qureshi SS et al., 2014 [10] | 7 | 36 (11–72) | Trans-manubrial (n = 4); trap-door (n = 3) | 327 (69–240) | Neuroblastoma (n = 7) | 6.5 (5–10) | Diaphragmatic paralysis (n = 1) | Alive: 5/7 (66.7%); complete remission: 5/7 (66.7%) | nd |
| El Madi A et al., 2007 [4] | 9 | 71.8 (4–188) | Trans-manubrial (n = 9) | nd | Neuroblastoma (n = 6); ganglioneuroblastoma (n = 3) | 7 | Chylothorax (n = 2); Bernard–Horner Syndrome (n = 2); diaphragmatic paralysis (n = 2); left hand paresthesia (n = 1) | Alive: 7/9 (77.8%); complete remission: 4/9 (44.4%) | 92.6 (3–190) |
| Chui CH et al., 2020 [2] | 21 | 42 (3.6–94.8) | Trap-door (n = 21) | 312 (150–546) | Neuroblastoma (n = 18); ganglioneuroblastoma (n = 3) | nd | Klumpke’s palsy (n = 1); winged scapula (n = 1); diaphragmatic paralysis (n = 1); bronchomalacia (n = 2); Bernard–Horner Syndrome (n = 21) | Alive: 16/21 (75.0%); complete remission: nd | 33.6 (3.6–92.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martucciello, G.; Fati, F.; Avanzini, S.; Senes, F.M.; Paraboschi, I. The Cervico-Parasternal Thoracotomy (CPT): A New Surgical Approach for the Resection of Cervicothoracic Neuroblastomas. Children 2021, 8, 229. https://doi.org/10.3390/children8030229
Martucciello G, Fati F, Avanzini S, Senes FM, Paraboschi I. The Cervico-Parasternal Thoracotomy (CPT): A New Surgical Approach for the Resection of Cervicothoracic Neuroblastomas. Children. 2021; 8(3):229. https://doi.org/10.3390/children8030229
Chicago/Turabian StyleMartucciello, Giuseppe, Federica Fati, Stefano Avanzini, Filippo Maria Senes, and Irene Paraboschi. 2021. "The Cervico-Parasternal Thoracotomy (CPT): A New Surgical Approach for the Resection of Cervicothoracic Neuroblastomas" Children 8, no. 3: 229. https://doi.org/10.3390/children8030229
APA StyleMartucciello, G., Fati, F., Avanzini, S., Senes, F. M., & Paraboschi, I. (2021). The Cervico-Parasternal Thoracotomy (CPT): A New Surgical Approach for the Resection of Cervicothoracic Neuroblastomas. Children, 8(3), 229. https://doi.org/10.3390/children8030229