
Update on Acute Disseminated Encephalomyelitis in Children and Adolescents


Abstract
:1. Introduction
2. Insights in the Acute Disseminated Encephalomyelitis (ADEM)
2.1. Epidemiology
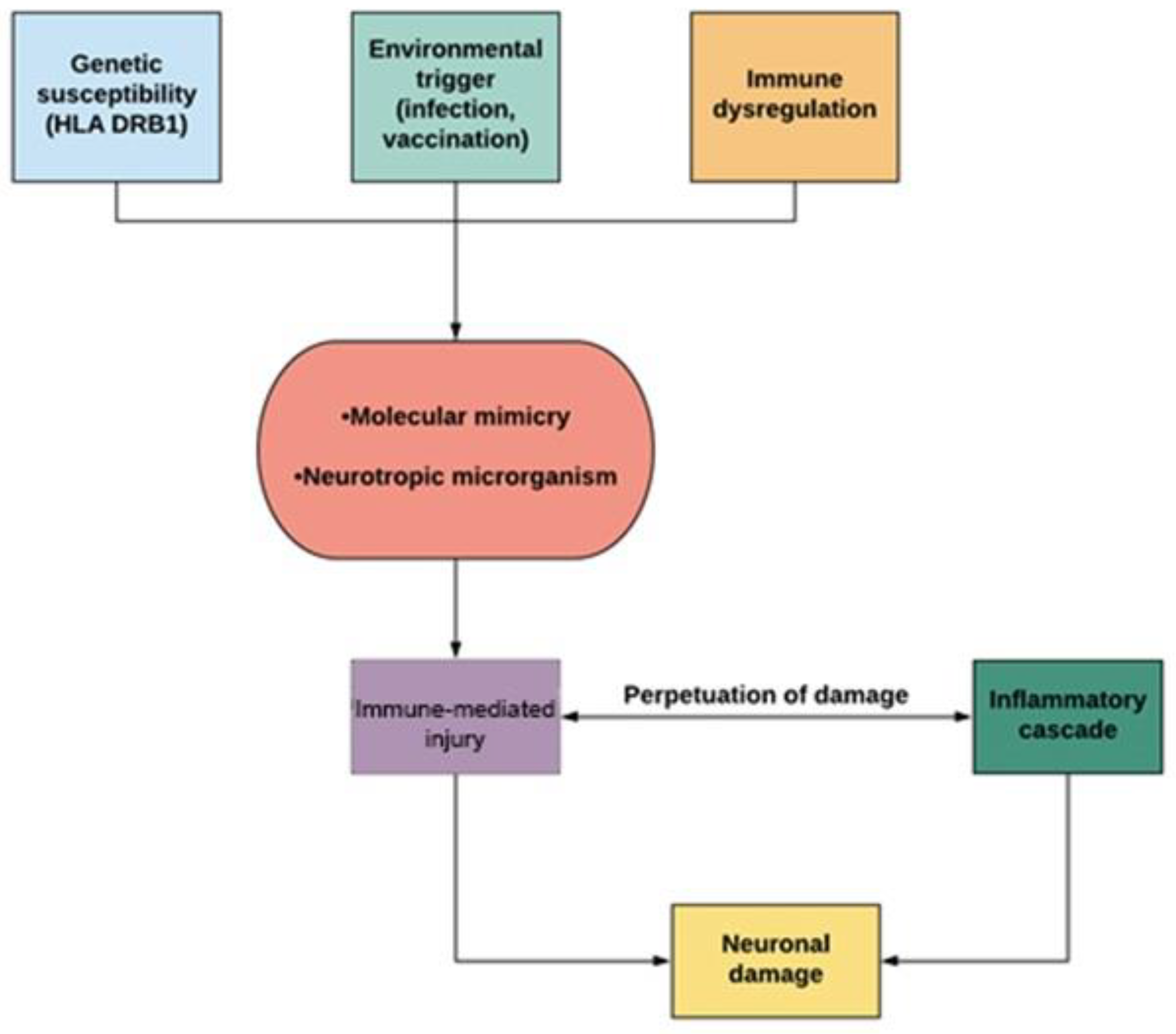
2.2. Pathogenesis
2.3. Clinical Presentation
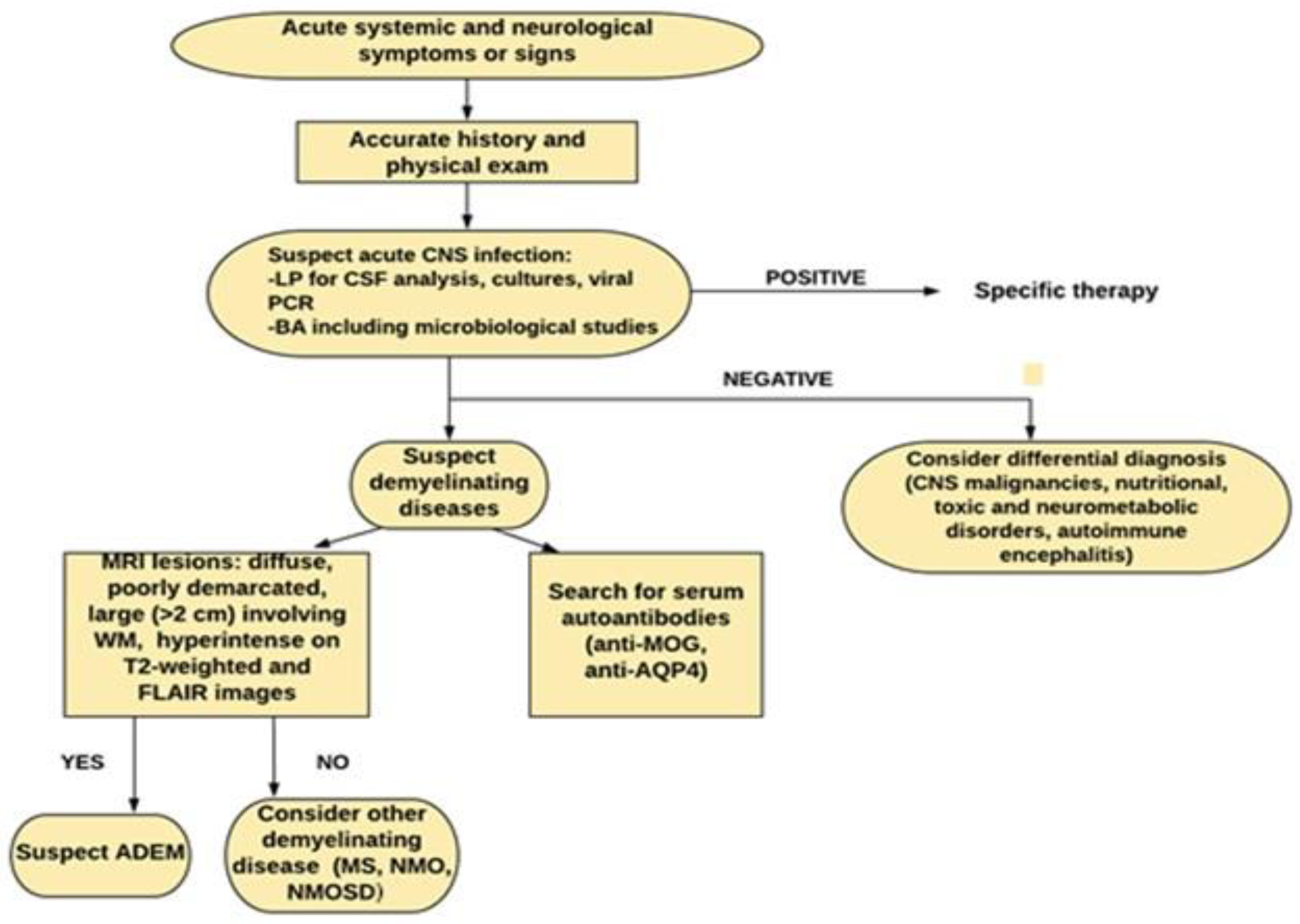
2.4. Diagnosis
2.5. Outcome
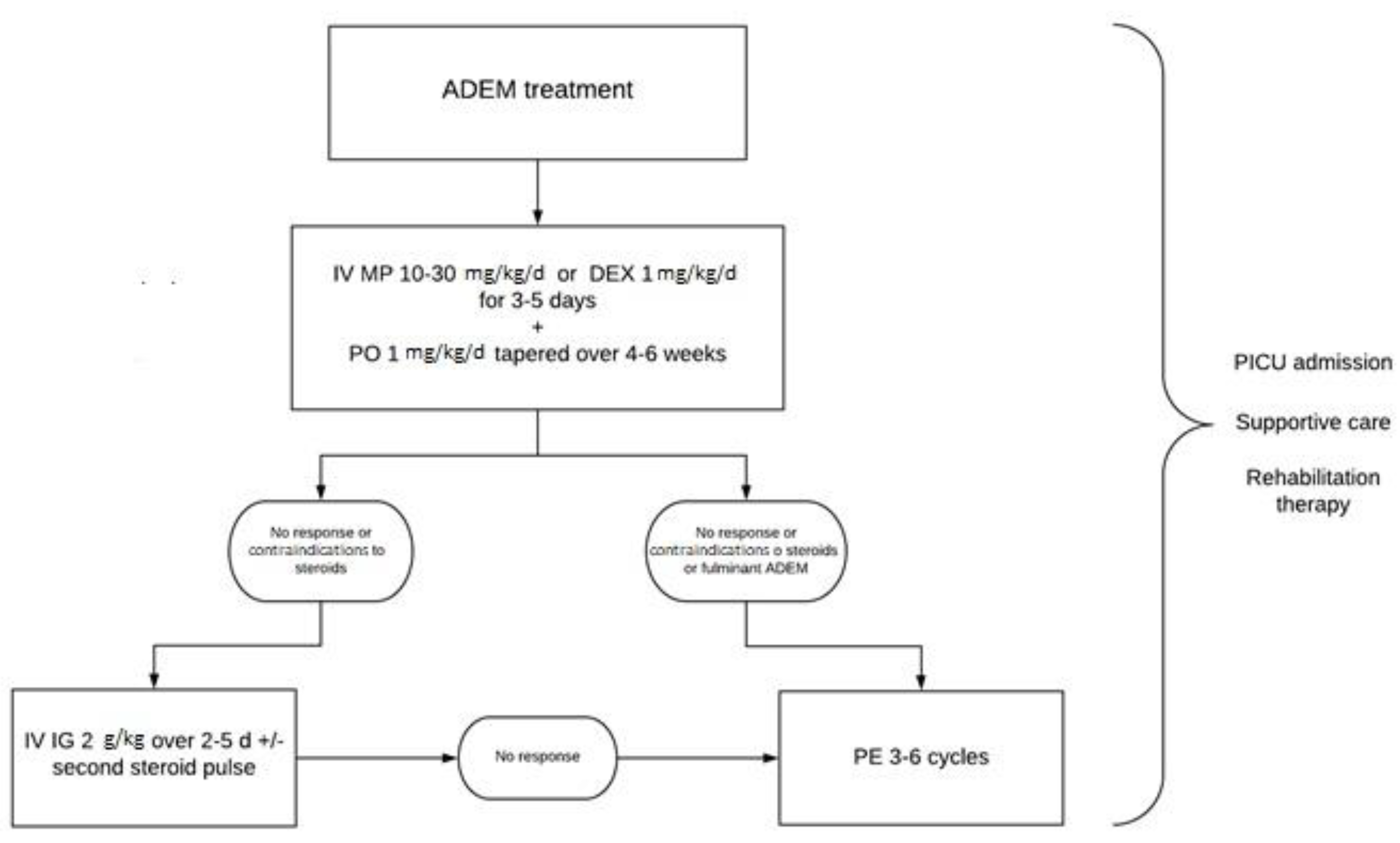
3. Treatment
3.1. Corticosteroids (CS)
3.2. Intravenous Immunoglobulin (IVIG) Therapy
3.3. Plasma Exchange (PE)
3.4. Cyclophosphamide (CYC) and Other Immunomodulatory Therapies
3.5. Supportive Care
3.6. Rehabilitation Therapy
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carlisi, E.; Pavese, C.; Mandrini, S.; Carenzio, G.; Toffola, E.D. Early rehabilitative treatment for pediatric acute disseminated encephalomyelitis: Case report. Eur. J. Phys. Rehabil. Med. 2014, 51, 341–343. [Google Scholar]
- Paolilo, R.B.; Deiva, K.; Neuteboom, R.; Rostásy, K.; Lim, M. Acute Disseminated Encephalomyelitis: Current Perspectives. Children 2020, 7, 210. [Google Scholar] [CrossRef]
- Matricardi, S.; Farello, G.; Savasta, S.; Verrotti, A. Understanding Childhood Neuroimmune Diseases of the Central Nervous System. Front. Pediatr. 2019, 7, 511. [Google Scholar] [CrossRef] [Green Version]
- Cole, J.; Evans, E.; Mwangi, M.; Mar, S. Acute Disseminated Encephalomyelitis in Children: An Updated Review Based on Current Diagnostic Criteria. Pediatr. Neurol. 2019, 100, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Alper, G. Acute Disseminated Encephalomyelitis. J. Child. Neurol. 2012, 27, 1408–1425. [Google Scholar] [CrossRef] [PubMed]
- Berzero, G.; Cortese, A.; Ravaglia, S.; Marchioni, E. Diagnosis and therapy of acute disseminated encephalomyelitis and its variants. Expert Rev. Neurother. 2015, 16, 83–101. [Google Scholar] [CrossRef]
- Esposito, S.; Di Pietro, G.M.; Madini, B.; Mastrolia, M.V.; Rigante, D. A spectrum of inflammation and demyelination in acute disseminated encephalomyelitis (ADEM) of children. Autoimmun. Rev. 2015, 14, 923–929. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Qian, L.; Tartof, S.Y.; Brara, S.M.; Jacobsen, S.J.; Beaber, B.E.; Sy, L.S.; Chao, C.; Hechter, R.; Tseng, H.F. Vaccines and the Risk of Multiple Sclerosis and Other Central Nervous System Demyelinating Diseases. JAMA Neurol. 2014, 71, 1506–1513. [Google Scholar] [CrossRef] [Green Version]
- Garg, R.K.; Malhotra, H.S.; Kumar, N. Chapter 10—Pathophysiology of acute disseminated encephalomyelitis. In Multiple Sclerosis; Minagar, A., Ed.; Academic Press: San Diego, CA, USA, 2016; pp. 201–248. [Google Scholar]
- Ayed, H.; Chaudhary, M.W.; AlBaradie, R.; Mir, A. Use of Cyclophosphamide in a Child with Fulminant Acute Disseminated Encephalomyelitis. Child. Neurol. Open 2018, 5, PMC5851101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippi, M.; Rocca, M.A. Acute Disseminated Encephalomyelitis. White Matter Dis. 2020, 109–125. [Google Scholar] [CrossRef]
- Esposito, S.; Picciolli, I.; Semino, M.; Principi, N. Steroids and Childhood Encephalitis. Pediatr. Infect. Dis. J. 2012, 31, 759–760. [Google Scholar] [CrossRef] [Green Version]
- Santoro, J.D.; Chitnis, T. Diagnostic Considerations in Acute Disseminated Encephalomyelitis and the Interface with MOG Antibody. Neuropediatrics 2019, 50, 273–279. [Google Scholar] [CrossRef]
- Steiner, I.; Kennedy, P.G.E. Acute disseminated encephalomyelitis: Current knowledge and open questions. J. Neurovirol. 2015, 21, 473–479. [Google Scholar] [CrossRef]
- Anilkumar, A.C.; Foris, L.A.; Tadi, P. Acute Disseminated Encephalomyelitis; Stat Pearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Lin, C.-H.; Jeng, J.-S.; Hsieh, S.-T.; Yip, P.-K.; Wu, R.-M. Acute disseminated encephalomyelitis: A follow-up study in Taiwan. J. Neurol. Neurosurg. Psychiatry 2007, 78, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koelman, D.L.H.; Mateen, F.J. Acute disseminated encephalomyelitis: Current controversies in diagnosis and outcome. J. Neurol. 2015, 262, 2013–2024. [Google Scholar] [CrossRef] [PubMed]
- Chitnis, T. Pediatric Central Nervous System Demyelinating Diseases. Contin. Lifelong Learn. Neurol. 2019, 25, 793–814. [Google Scholar] [CrossRef] [PubMed]
- Tenembaum, S.; Chitnis, T.; Ness, J.; Hahn, J.S.; The International Pediatric MS Study Group. Acute disseminated encephalomyelitis. Neurology 2007, 68, 23–36. [Google Scholar] [CrossRef]
- Ketelslegers, I.A.; Visser, I.E.R.; Neuteboom, R.F.; Boon, M.; Catsman-Berrevoets, C.E.; Hintzen, R.Q. Disease course and outcome of acute disseminated encephalomyelitis is more severe in adults than in children. Mult. Scler. J. 2011, 17, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Tardieu, M.; Amato, M.P.; Banwell, B.; Chitnis, T.; Dale, R.C.; Ghezzi, A.; Hintzen, R.; Kornberg, A.; Pohl, D.; et al. International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: Revisions to the 2007 definitions. Mult. Scler. J. 2013, 19, 1261–1267. [Google Scholar] [CrossRef]
- Waters, P.; Fadda, G.; Woodhall, M.; O’Mahony, J.; Brown, R.A.; Castro, D.A.; Longoni, G.; Irani, S.R.; Sun, B.; Yeh, E.A.; et al. Serial Anti–Myelin Oligodendrocyte Glycoprotein Antibody Analyses and Outcomes in Children with Demyelinating Syndromes. JAMA Neurol. 2020, 77, 82. [Google Scholar] [CrossRef] [Green Version]
- Ramanathan, S.; Mohammad, S.; Tantsis, E.; Nguyen, T.K.; Merheb, V.; Fung, V.S.C.; White, O.B.; Broadley, S.; Lechner-Scott, J.; Vucic, S.; et al. Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination. J. Neurol. Neurosurg. Psychiatry 2018, 89, 127–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banwell, B.; Tenembaum, S.; Lennon, V.A.; Ursell, E.; Kennedy, J.; Bar-Or, A.; Weinshenker, B.G.; Lucchinetti, C.F.; Pittock, S.J. Neuromyelitis optica-IgG in childhood inflammatory demyelinating CNS disorders. Neurology 2007, 70, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Bigi, S.; Banwell, B.; Yeh, E.A. Outcomes After Early Administration of Plasma Exchange in Pediatric Central Nervous System Inflammatory Demyelination. J. Child. Neurol. 2014, 30, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Lee, R.; Lee, J.C.; Tse, A.C.; Pang, S.Y.; Lau, G.K.; Teo, K.C.; Ho, P.W. Central nervous system inflammatory demyelinating disorders among Hong Kong Chinese. J. Neuroimmunol. 2013, 262, 100–105. [Google Scholar] [CrossRef]
- Lademann, H.; Bertsche, A.; Petzold, A.; Zack, F.; Büttner, A.; Däbritz, J.; Hauenstein, C.; Bahn, E.; Spang, C.; Reuter, D.; et al. Acute Disseminated Encephalomyelitis with Seizures and Myocarditis: A Fatal Triad. Medicina 2020, 56, 277. [Google Scholar] [CrossRef]
- Pohl, D.; Alper, G.; Van Haren, K.; Kornberg, A.J.; Lucchinetti, C.F.; Tenembaum, S.; Belman, A.L. Acute disseminated encephalomyelitis. Neurology 2016, 87, S38–S45. [Google Scholar] [CrossRef] [PubMed]
- Repić-Buličić, A.; Filipović-Grčić, P.; Jadrijević, E.; Jurinović, P.; Titlić, M. Successful Treatment of Acute Disseminated Encephalomyelitis (ADEM) by Prompt Usage of Immunoglobulins—Case Report and Review of the Literature. Acta Clin. Croat. 2019, 58, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Alexander, M.; Murthy, J.M.K. Acute disseminated encephalomyelitis: Treatment guidelines. Ann. Indian Acad. Neurol. 2011, 14, 60–64. [Google Scholar] [CrossRef]
- Gray, M.P.; Gorelick, M.H. Acute Disseminated Encephalomyelitis. Pediatr. Emerg. Care 2016, 32, 395–400. [Google Scholar] [CrossRef]
- Waldman, A.T.; Gorman, M.P.; Rensel, M.R.; Austin, T.E.; Hertz, D.P.; Kuntz, N.L.; Network of Pediatric Multiple Sclerosis Centers of Excellence of National Multiple Sclerosis Society. Management of pediatric central nervous system demyelinating disorders: Consensus of United States neurologists. J. Child. Neurol. 2011, 26, 675–682. [Google Scholar] [CrossRef]
- Tenembaum, S.; Chamoles, N.; Fejerman, N. Acute disseminated encephalomyelitis: A long-term follow-up study of 84 pediatric patients. Neurology 2002, 59, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Dale, R.C.; De Sousa, C.; Chong, W.K.; Cox, T.C.S.; Harding, B.; Neville, B.G.R. Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children. Brain 2000, 123, 2407–2422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anlar, B.; Guven, A.; Haspolat, S.; Yakut, A.; Serdaroglu, A.; Senbil, N.; Karaagaoglu, E.; Oguz, K.K.; Basaran, C.; Köse, G.; et al. Acute Disseminated Encephalomyelitis in Children: Outcome and Prognosis. Neuropediatrics 2003, 34, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Gupte, G.; Stonehouse, M.; Wassmer, E.; Coad, N.; Whitehouse, W. Acute disseminated encephalomyelitis: A review of 18 cases in childhood. J. Paediatr. Child. Health 2003, 39, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Leake, J.A.D.; Albani, S.; Kao, A.S.; Senac, M.O.; Billman, G.F.; Nespeca, M.P.; Paulino, A.D.; Quintela, E.R.; Sawyer, M.H.; Bradley, J.S. Acute Disseminated Encephalomyelitis in Childhood: Epidemiologic, Clinical and Laboratory Features. Pediatr. Infect. Dis. J. 2004, 23, 756–764. [Google Scholar] [CrossRef]
- Feasby, T.; Banwell, B.; Benstead, T.; Bril, V.; Brouwers, M.; Freedman, M.; Hahn, A.; Hume, H.; Freedman, J.; Pi, D.; et al. Guidelines on the Use of Intravenous Immune Globulin for Neurologic Conditions. Transfus. Med. Rev. 2007, 21, S57–S107. [Google Scholar] [CrossRef]
- Elovaara, I.; Apostolski, S.; Van Doorn, P.; Gilhus, N.E.; Hietaharju, A.; Honkaniemi, J.; Van Schaik, I.N.; Scolding, N.; Sørensen, P.S.; Udd, B. EFNS guidelines for the use of intravenous immunoglobulin in treatment of neurological diseases. Eur. J. Neurol. 2008, 15, 893–908. [Google Scholar] [CrossRef]
- Imataka, G.; Arisaka, O. An infant with steroid-refractory cytomegalovirus-associated ADEM who responded to immuno-globulin therapy. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 2148–2151. [Google Scholar] [PubMed]
- Banerjee, A.; Suthar, R.; Vyas, S.; Singh, M.P. Acute disseminated encephalomyelitis: Complication of a vaccine preventable disease. BMJ Case Rep. 2018, 11, e225710. [Google Scholar] [CrossRef]
- Pradhan, S.; Gupta, R.P.; Shashank, S.; Pandey, N. Intravenous immunoglobulin therapy in acute disseminated encephalomyelitis. J. Neurol. Sci. 1999, 165, 56–61. [Google Scholar] [CrossRef]
- Straussberg, R.; Schonfeld, T.; Weitz, R.; Karmazyn, B.; Harel, L. Improvement of atypical acute disseminated encephalomyelitis with steroids and intravenous immunoglobulins. Pediatr. Neurol. 2001, 24, 139–143. [Google Scholar] [CrossRef]
- Kanaheswari, Y.; Baizura, J.; Paeds, M.; Zulfiqar, A. Intravenous immunoglobulin in the treatment of acute disseminated en-cephalomyelitis. Med. J. Malaysia 2004, 59, 103–117. [Google Scholar] [PubMed]
- Nishikawa, M.; Ichiyama, T.; Hayashi, T.; Ouchi, K.; Furukawa, S. Intravenous immunoglobulin therapy in acute disseminated encephalomyelitis. Pediatr. Neurol. 1999, 21, 583–586. [Google Scholar] [CrossRef]
- Ramachandrannair, R.; Rafeequ, M.; Girija, A.S. Plasmapheresis in childhood acute disseminated encephalomyelitis. Indian Pediatr. 2005, 42, 479–482. [Google Scholar] [PubMed]
- Minagar, A.; Alexander, S.J. Inflammatory Disorders of the Nervous System: Pathogenesis, Immunology, and Clinical Management; Humana Press: Totowa, NJ, USA, 2017. [Google Scholar]
- Pohl, D.; Tenembaum, S. Treatment of Acute Disseminated Encephalomyelitis. Curr. Treat. Options Neurol. 2012, 14, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Balestri, P.; Grosso, S.; Acquaviva, A.; Bernini, M. Plasmapheresis in a child affected by acute disseminated encephalomyelitis. Brain Dev. 2000, 22, 123–126. [Google Scholar] [CrossRef]
- Weinshenker, B.G.; O’Brien, P.C.; Petterson, T.M.; Noseworthy, J.H.; Lucchinetti, C.F.; Dodick, D.W.; Pineda, A.A.; Stevens, L.N.; Rodriguez, M. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann. Neurol. 1999, 46, 878–886. [Google Scholar] [CrossRef]
- Vitaliti, G.; Tabatabaie, O.; Matin, N.; Ledda, C.; Pavone, P.; Lubrano, R.; Serra, A.; Di Mauro, P.; Cocuzza, S.; Falsaperla, R. The usefulness of immunotherapy in pediatric neurodegenerative disorders: A systematic review of literature data. Hum. Vaccines Immunother. 2015, 11, 2749–2763. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Tian, X.; Gu, Y.; Li, F.; Wang, X. Application of Plasma Exchange in Steroid-Responsive Encephalopathy. Front. Immunol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Miyazawa, R.; Hikima, A.; Takano, Y.; Arakawa, H.; Tomomasa, T.; Morikawa, A. Plasmapheresis in fulminant acute disseminated encephalomyelitis. Brain Dev. 2001, 23, 424–426. [Google Scholar] [CrossRef]
- Koziolek, M.; Mühlhausen, J.; Friede, T.; Ellenberger, D.; Sigler, M.; Huppke, B.; Gärtner, J.; Müller, G.-A.; Huppke, P. Therapeutic Apheresis in Pediatric Patients with Acute CNS Inflammatory Demyelinating Disease. Blood Purif. 2013, 36, 92–97. [Google Scholar] [CrossRef]
- Khurana, D.S.; Melvin, J.J.; Kothare, S.V.; Valencia, I.; Hardison, H.H.; Yum, S.; Faerber, E.N.; Legido, A. Acute Disseminated Encephalomyelitis in Children: Discordant Neurologic and Neuroimaging Abnormalities and Response to Plasmapheresis. Pediatrics 2005, 116, 431–436. [Google Scholar] [CrossRef] [Green Version]
- Yae, Y.; Kawano, G.; Yokochi, T.; Imagi, T.; Akita, Y.; Ohbu, K.; Matsuishi, T. Fulminant acute disseminated encephalomyelitis in children. Brain Dev. 2019, 41, 373–377. [Google Scholar] [CrossRef]
- Takata, T.; Hirakawa, M.; Sakurai, M.; Kanazawa, I. Fulminant form of acute disseminated encephalomyelitis: Successful treatment with hypothermia. J. Neurol. Sci. 1999, 165, 94–97. [Google Scholar] [CrossRef]
- Granget, E.; Milh, M.; Pech-Gourg, G.; Paut, O.; Girard, N.; Lena, G.; Scavarda, D. Life-saving decompressive craniectomy for acute disseminated encephalomyelitis in a child: A case report. Childs Nerv. Syst. 2012, 28, 1121–1124. [Google Scholar] [CrossRef]
- Sadek, A.A.; Mohamed, M.A.; Abou-Taleb, A.; Mohammed, M.I. Pattern and Outcome of Acute Disseminated Encephalomyelitis (ADEM) in Children: Experience in a Tertiary Center, Upper Egypt. Electron. Physician 2016, 8, 2679–2685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, G.; Ramos, E. Chronic Sequelae of Acute Disseminated Encephalomyelitis in a Child. PMR 2010, 2, 868–871. [Google Scholar] [CrossRef] [PubMed]
- Bruijstens, A.L.; Wendel, E.-M.; Lechner, C.; Bartels, F.; Finke, C.; Breu, M.; Flet-Berliac, L.; de Chalus, A.; Adamsbaum, C.; Capobianco, M.; et al. E.U. paediatric MOG consortium consensus: Part 5—Treatment of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders. Eur. J. Paediatr. Neurol. 2020, 29, 41–53. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Bacteria | Viruses | Parasites |
|---|---|---|
| Mycoplasma pneumoniae Campylobacter jejuni Chlamydia pneumoniae Borrelia burgdorferi Legionella pneumoniae Leptospira spp. Haemophilus influenzae type b Streptococcus pyogenes Rickettsia sp. | Cytomegalovirus Epstein–Barr virus Herpes simplex virus Human herpesvirus 6 Influenza Hepatitis A and C HIV Enterovirus Coronavirus Mumps Measles Rubella Coxsackie B Varicella zoster virus Dengue | Toxoplasma gondii Plasmodium falciparum Cryptococcus neoformans |
| Symptoms/Signs of Acute Phase | Prevalence (%) |
|---|---|
| Encephalopathy | 100% by definition |
| Fever | 12–68% |
| Headache | 6–64% |
| Seizures | 12–50% |
| Cranial nerve deficits | 18–39% |
| Speech disturbance | 7–44% |
| Pyramidal signs | 18–60% |
| Sensory deficits | 0–9% |
| Cerebellar signs/ataxia | 36–47% |
| Optic neuritis | 1–15% |
| Urinary disturbance | 6–25% |
| Pediatric ADEM (All Are Required) |
|---|
| A first polyfocal, clinical central nervous system event with presumed inflammatory demyelinating cause; Encephalopathy that cannot be explained by fever; No new clinical and MRI findings emerging three months or more after the onset; Brain MRI is abnormal during the acute (three months) phase. Typically, on brain MRI: Diffuse, poorly demarcated, large (>1–2 cm) lesions involving predominantly the cerebral white matter; T1 hypointense lesions in the white matter are rare; Deep grey matter lesion (e.g., thalamus or basal ganglia) can be present. |
| References | Authors/Year | Type of Study | Population | Treatment | Oral Taper | Additional Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| Acute disseminated encephalomyelitis: a long-term follow-up study of 84 pediatric patients [33] | Tenembaum et al., Neurology, 2002 | Prospective study | 84 patients (0.4–16 years) with ADEM | 80 children treated with CSs: -43 patients treated with IV DEX 1 mg/kg/day for 10 days -21 patients IV MP 30 mg/kg/day if weight ≤30 kg, 1 g/day if weight ≥30 kg for 3 to 5 days followed by PO 1 mg/kg/day for 10 days -10 patients treated with PO 2 mg/kg/day for 10 days -6 patients received oral deflazacort 3 mg/kg/day | Steroid oral tapering over 4 to 6 weeks | -29 patients: antiepileptic -58 Acyclovir -36 ICU -14 artificial ventilation | Median EDSS score of 3 (0 to 6.5) for 25 patients treated with IV DEX Median EDSS score of 1 (0 to 3) for 21 patients treated with IV MP (all patients with similar clinical involvement) (p = 0.029) No steroid dependency |
| Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children [34] | Dale et al., Brain, 2000 | Prospective study | 48 children: 28 with ADEM, 7 with MDEM, 13 with MS (3–16 years) | 25 patients with ADEM/MDEM treated with IV MP 30 mg/kg/day for 5 days | PO | -Antibiotics/antivirals (66%) | Comparison of mean length of steroid treatment: -relapsing MDEM group (n = 6) ->only 3.17 w (range 0.5–8 weeks) -non-relapsing ADEM group (n = 19) ->6.3 weeks (range 0.5–16 weeks) |
| Acute disseminated encephalomyelitis in children: outcome and prognosis [35] | Anlar et al., Neuropediatrics, 2003 | Multicenter prospective study | 46 patients (13 mo–15 years) with ADEM | 40 patients treated with CSs at the first attack: 28 patients received IV MP 20–30 mg/kg/day for 5 days 2 patients not treated | 18 patients PO 2–6 weeks | -12 patients Acyclovir -3 patients antibiotics -3 patients IVIG | High-dose MP associated with fewer complications (p = 0.02) Relapses in 2/8 (25%) of patients treated with high-dose MP within 7 days during first attack Relapses in 11/31 (35%) of patients who did not receive MP treatment within 7 d at the first attack. (outcome evaluated in 39 patients with follow-up >12 m) Tapering steroids over 3 w or longer associated with a lower relapse rate (difference statistically insignificant) |
| Acute disseminated encephalomyelitis: a review of 18 cases in childhood [36] | Gupte et al., J. Paediatrics Child Health, 2003 | Retrospective study | 18 children (3.5 months- 17 years) with ADEM | -8 patients: IV MP 20 mg/kg/day for 3–5 days -2 patients: IV DEX for 3–10 days -2 patients: only PO for 6 weeks -5 patients: no treatment | After IV CSs (n=10): PO 2 mg/kg/day, tapering over 4–6 weeks | -2 children with early relapses:sec ond pulse of CSs -1 patient: IVIG | Follow-up of 3 months–4 years: -good outcomes -two relapses after the cessation of steroids, complete recovery after second pulse of steroid -five children with ongoing disabilities |
| Acute disseminated encephalomyelitis in childhood: epidemiologic, clinical and laboratory features [37] | Leake et al., Pediatric Infectious Diseases Journal, 2004 | Prospective and retrospective study | 42 patients (10 months -18 years) with ADEM | -33 patients: IV MP or DEX -9 patients: no treatment | Oral CSs | - 8/33 patients treated with second-line therapy IVIGs 1 g/kg/day | No statistically significant differences between CS-treated and untreated patients regarding the duration of hospitalization (p = 0.43) and hospital readmission (p = 0.67) |
| References | Authors/Year | Type of Study | Population | First-Line Treatment | Second-Line Treatment | Additional Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| An infant with steroid-refractory cytomegalovirus-associated ADEM who responded to immunoglobulin therapy [40] | Imataka et al., European Review for Medical and Pharmacological Sciences, 2014 | Case report | 10-month-old boy with monophasic CMV-related ADEM | IV MP 30 mg/kg/d for 3 day-started at 9 day after onset ->no clinical improvement plus necessity of intubation | ayIVIGs at 400 mg/kg/day for 5 days started at the 15th day after onset | Continuous IV midazolam 0.3 mg/kg/hour | -Improvement in consciousness and general muscle strength since 20th d -MRI normalization 19th day-6th month -No adverse reaction -No neurological sequelae at 4 years |
| Acute disseminated encephalomyelitis: complication of a vaccine preventable disease [41] | Banerjee et al., BMJ Case Reports, 2018 | Case report | 8-year-old girl with mumps-related ADEM | IV MP 30 mg/kg/d for 5 day ->poor neurological recovery (EDSS) | aySecond course of IV MP 30 mg/kg/day for 5 days plus IVIGs 2 g/kg/day | -No residual motor deficits at 6 month of follow-up -Bladder dysfunction | |
| Intravenous immunoglobulin therapy in acute disseminated encephalomyelitis [42] | Pradhan et al., Journal of the Neurological Sciences, 1999 | Case reports | 4 children (1 year–14 years) with severe ADEM (2 patients intubated upon admission) | IV MP 10–15 mg/kg/d for 3–5 days ->no improvement and severe conditions | IVIGs 400 mg/kg/d for 5 days from the next day | 1 patient: oral carbamazepine | -Extubation from day 7–10 -MRI after 2 weeks: considerable resolution -Walk without support in 1–6 months |
| Intravenous immunoglobulin in the treatment of acute disseminated encephalomyelitis [44] | Kanaheswari et al., Medical Journal of Malaysia, 2004 | Case report | 3-year-old Chinese boy with recurrent episodes (3) of ADEM (most likely triggered by S. typhi) | IVIGs 2 g/kg/day over 5 days | None | IV Ampicillin, Cefotaxime, Acyclovir | -Response within 48 hours -No residual neurological symptoms or signs (MRI) on his first year of follow-up |
| Intravenous immunoglobulin therapy in acute disseminated encephalomyelitis [45] | Nishikawa et al., Pediatric Neurology, 1999 | Case reports | 3 children (2–5 years ) with ADEM related to gastroenteritis or mumps | IVIGs 400 mg/kg/d for 5 days | ayNone | IV antibiotic | -Improvement in consciousness in 14 hours –4 days -Complete clinical improvement in 7 days–18 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massa, S.; Fracchiolla, A.; Neglia, C.; Argentiero, A.; Esposito, S. Update on Acute Disseminated Encephalomyelitis in Children and Adolescents. Children 2021, 8, 280. https://doi.org/10.3390/children8040280
Massa S, Fracchiolla A, Neglia C, Argentiero A, Esposito S. Update on Acute Disseminated Encephalomyelitis in Children and Adolescents. Children. 2021; 8(4):280. https://doi.org/10.3390/children8040280
Chicago/Turabian StyleMassa, Serena, Adriana Fracchiolla, Cosimo Neglia, Alberto Argentiero, and Susanna Esposito. 2021. "Update on Acute Disseminated Encephalomyelitis in Children and Adolescents" Children 8, no. 4: 280. https://doi.org/10.3390/children8040280
APA StyleMassa, S., Fracchiolla, A., Neglia, C., Argentiero, A., & Esposito, S. (2021). Update on Acute Disseminated Encephalomyelitis in Children and Adolescents. Children, 8(4), 280. https://doi.org/10.3390/children8040280