
Mindfulness-Based Stress Reduction (MBSR) and Self Compassion (SC) Training for Parents of Children with Autism Spectrum Disorders: A Pilot Trial in Community Services in Spain

 ,
,  ,
, 
Abstract
1. Introduction
2. Methods
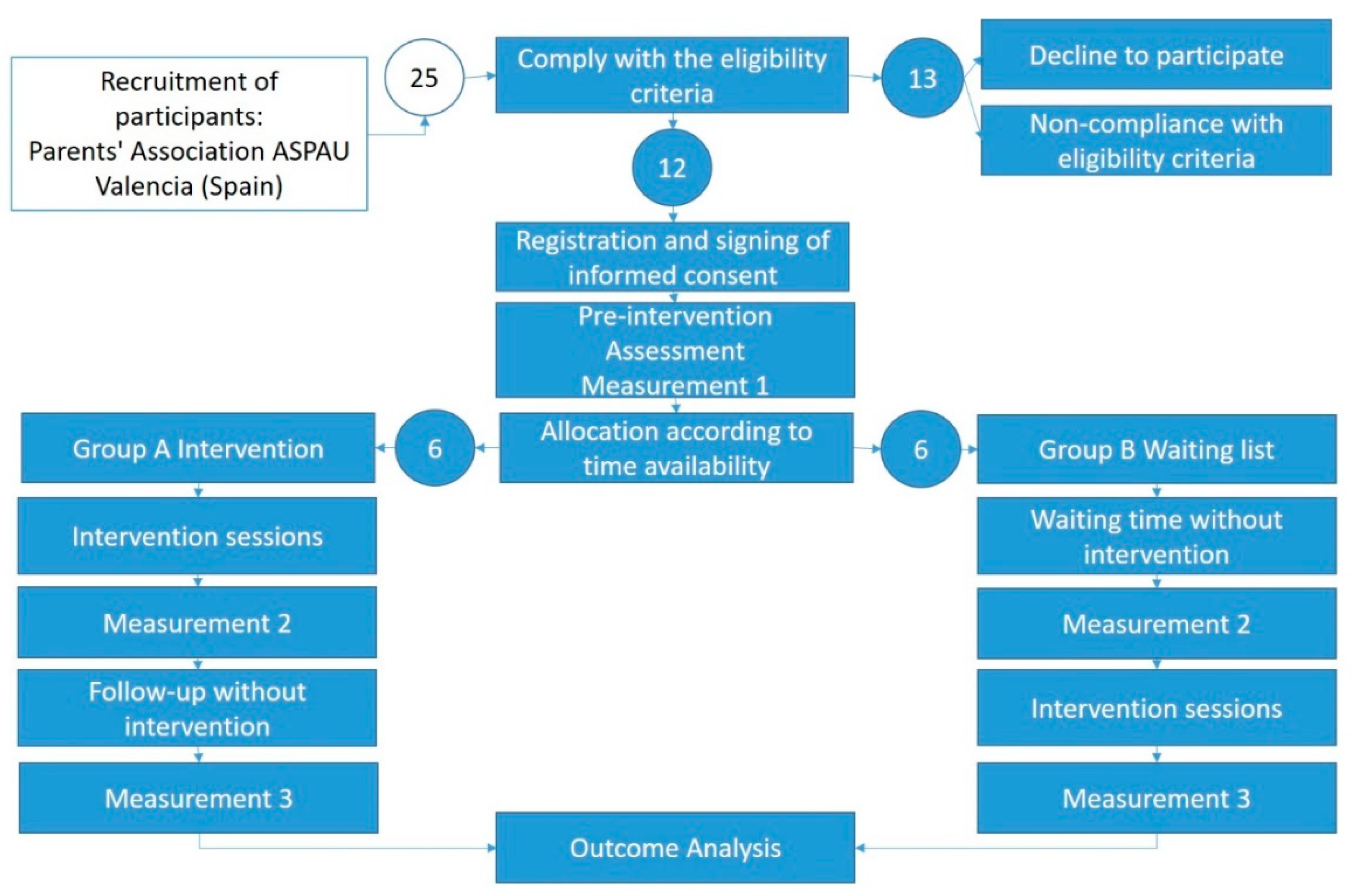
2.1. Procedure
2.2. Participants
2.3. Characteristics of Children
2.4. Measures
2.5. Mindfulness and Self-Compasion-Based Intervention Program
2.6. Weekly/Daily Qualitative Assessment
2.7. Support Materials
2.8. Adherence to Treatment
2.9. Design and Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, K.W.; Creswell, J.D.; Ryan, R.R.M. Handbook of Mindfulness: Theory, Research, and Practice; Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Toniolo-Barrios, M.; Brasil, A.; Pitt, L.F. Nine Prolific Years: An Analysis of Publications in Mindfulness. Mindfulness 2020, 11, 1077–1089. [Google Scholar] [CrossRef]
- Vallejo-Pareja, M.A. Mindfulness. Pap. Psicól. 2006, 27, 92–99. Available online: http://www.papelesdelpsicologo.es/pdf/1340.pdf (accessed on 16 May 2020).
- Chiesa, A.; Serretti, A. Mindfulness-Based Stress Reduction for Stress Management in Healthy People: A Review and Meta-Analysis. J. Altern. Complement. Med. 2009, 15, 593–600. [Google Scholar] [CrossRef]
- Chu, S.T.-W.; Mak, W.W.S. How Mindfulness Enhances Meaning in Life: A Meta-Analysis of Correlational Studies and Randomized Controlled Trials. Mindfulness 2020, 11, 177–193. [Google Scholar] [CrossRef]
- Keng, S.-L.; Smoski, M.J.; Robins, C.J. Effects of mindfulness on psychological health: A review of empirical studies. Clin. Psychol. Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef]
- Khoury, B.; Sharma, M.; Rush, S.E.; Fournier, C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J. Psychosom. Res. 2015, 78, 519–528. [Google Scholar] [CrossRef]
- Wilson, A.C.; Mackintosh, K.; Power, K.; Chan, S.W.Y. Effectiveness of Self-Compassion Related Therapies: A Systematic Review and Meta-analysis. Mindfulness 2019, 10, 979–995. [Google Scholar] [CrossRef]
- Falcone, G.; Jerram, M. Brain Activity in Mindfulness Depends on Experience: A Meta-Analysis of fMRI Studies. Mindfulness 2018, 9, 1319–1329. [Google Scholar] [CrossRef]
- Wang, Y.; Fan, L.; Zhu, Y.; Yang, J.; Wang, C.; Gu, L.; Zhong, S.; Huang, Y.; Xie, X.; Zhou, H.; et al. Neurogenetic Mechanisms of Self-Compassionate Mindfulness: The Role of Oxytocin-Receptor Genes. Mindfulness 2019, 10, 1792–1802. [Google Scholar] [CrossRef]
- Costa, M.D.A.; De Oliveira, G.S.D.; Tatton-Ramos, T.; Manfro, G.G.; Salum, G.A. Anxiety and Stress-Related Disorders and Mindfulness-Based Interventions: A Systematic Review and Multilevel Meta-analysis and Meta-Regression of Multiple Outcomes. Mindfulness 2019, 10, 996–1005. [Google Scholar] [CrossRef]
- Beck, K.B.; Greco, C.M.; Terhorst, L.A.; Skidmore, E.R.; Kulzer, J.L.; McCue, M.P. Mindfulness-Based Stress Reduction for Adults with Autism Spectrum Disorder: Feasibility and Estimated Effects. Mindfulness 2020, 11, 1286–1297. [Google Scholar] [CrossRef]
- Eisendrath, S.J. Mindfulness-Based Cognitive Therapy: Innovative Applications; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Kabat-Zinn, J.; Lipworth, L.; Burney, R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J. Behav. Med. 1985, 8, 163–190. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness for Beginners: Reclaiming the Present Moment and Your Life; Sounds True, Inc.: Boulder, CO, USA, 2012. [Google Scholar]
- Shapiro, S.L.; Astin, J.A.; Bishop, S.R.; Cordova, M. Mindfulness-Based Stress Reduction for Health Care Professionals: Results from a Randomized Trial. Int. J. Stress Manag. 2005, 12, 164–176. [Google Scholar] [CrossRef]
- Harvey, P. Mindfulness in Theravada Samatha and Vipassana Meditations, and in Secular Mindfulness, in Buddhist Foundations of Mindfulness; Springer: New York, NY, USA, 2015; pp. 115–135. [Google Scholar]
- Linehan, M.M. Cognitive Behavioral Tratment of Borderline Personality Disorder; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Chadwick, P. Person-Based Cognitive Therapy for Distressing Psychosis; Wiley: Chichester, UK, 2006. [Google Scholar]
- Dannahy, L.; Hayward, M.; Strauss, C.; Turton, W.; Harding, E.; Chadwick, P. Group person-based cognitive therapy for distressing voices: Pilot data from nine groups. J. Behav. Ther. Exp. Psychiatry 2011, 42, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; Hayes, S.C.; Walser, R.D. Learning ACT: An Acceptance; New Harbinger Publications: Oakland, CA, USA, 2007. [Google Scholar]
- Cayoun, B.A. Mindfulness-Integrated CBT: Principles and Practive; John Wiley & Sons Limited: Chichester, UK, 2011. [Google Scholar]
- Mikolajczak, M.; Gross, J.J.; Roskam, I. Parental Burnout: What Is It, and Why Does It Matter? Clin. Psychol. Sci. 2019, 7, 1319–1329. [Google Scholar] [CrossRef]
- Newacheck, P.W. Health Services Use and Health Care Expenditures for Children with Disabilities. Pediatrics 2004, 114, 79–85. [Google Scholar] [CrossRef]
- Sen, E.; Yurtsever, S. Difficulties Experienced by Families with Disabled Children. J. Spéc. Pediatr. Nurs. 2007, 12, 238–252. [Google Scholar] [CrossRef]
- Hartley, S.L.; Barker, E.T.; Seltzer, M.M.; Floyd, F.; Greenberg, J.; Orsmond, G.; Bolt, D. The relative risk and timing of divorce in families of children with an autism spectrum disorder. J. Fam. Psychol. 2010, 24, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Cachia, R.L.; Anderson, A.; Moore, D.W. Mindfulness, Stress and Well-Being in Parents of Children with Autism Spectrum Disorder: A Systematic Review. J. Child Fam. Stud. 2016, 25, 1–14. [Google Scholar] [CrossRef]
- Falk, N.H.; Norris, K.; Quinn, M.G. The Factors Predicting Stress, Anxiety and Depression in the Parents of Children with Autism. J. Autism Dev. Disord. 2014, 44, 3185–3203. [Google Scholar] [CrossRef]
- Firth, I.; Dryer, R. The predictors of distress in parents of children with autism spectrum disorder. J. Intellect. Dev. Disabil. 2013, 38, 163–171. [Google Scholar] [CrossRef]
- Merkaj, V.; Kika, M.; Simaku, A. Symptoms of Stress, Depression and Anxiety between Parents of Autistic Children and Parents of Tipically Developing Children. Acad. J. Interdiscip. Stud. 2013, 2, 345. [Google Scholar] [CrossRef]
- Almansour, M.A.; Alateeq, M.A.; Alzahrani, M.K.; Algeffari, M.A.; Alhomaifan, H.T. Depression and anxiety among parents and caregivers of autistic spectral disorder children. Neurosciences 2013, 18, 58–63. Available online: www.neurosciencesjournal.org (accessed on 29 December 2017).
- Hayes, S.A.; Watson, S.L. The Impact of Parenting Stress: A Meta-analysis of Studies Comparing the Experience of Parenting Stress in Parents of Children with and without Autism Spectrum Disorder. J. Autism Dev. Disord. 2013, 43, 629–642. [Google Scholar] [CrossRef]
- Pons-Salvador, G.; Cerezo, M.A.; Bernabé, G. Cambio y estabilidad en los factores que afectan negativamente a la parentalidad. Psicothema 2005, 17, 31–36. Available online: http://www.psicothema.com/pdf/3060.pdf (accessed on 27 December 2017).
- Osborne, L.A.; McHugh, L.; Saunders, J.; Reed, P. Parenting Stress Reduces the Effectiveness of Early Teaching Interventions for Autistic Spectrum Disorders. J. Autism Dev. Disord. 2008, 38, 1092–1103. [Google Scholar] [CrossRef]
- Bluth, K.; Roberson, P.N.E.; Billen, R.M.; Sams, J.M. A Stress Model for Couples Parenting Children with Autism Spectrum Disorders and the Introduction of a Mindfulness Intervention. J. Fam. Theory Rev. 2013, 5, 194–213. [Google Scholar] [CrossRef] [PubMed]
- Benn, R.; Akiva, T.; Arel, S.; Roeser, R. Mindfulness Training Effects for Parents and Educators of Children with Special Needs. Dev. Psychol. 2012, 48, 1476–1487. [Google Scholar] [CrossRef] [PubMed]
- Boekhorst, M.G.B.M.; Potharst, E.S.; Beerthuizen, A.; Hulsbosch, L.P.; Bergink, V.; Pop, V.J.M.; Nyklíček, I. Mindfulness During Pregnancy and Parental Stress in Mothers Raising Toddlers. Mindfulness 2020, 11, 1747–1761. [Google Scholar] [CrossRef]
- Gammer, I.; Hartley-Jones, C.; Jones, F.W. A Randomized Controlled Trial of an Online, Compassion-Based Intervention for Maternal Psychological Well-Being in the First Year Postpartum. Mindfulness 2020, 11, 928–939. [Google Scholar] [CrossRef]
- Eyberg, S. Parent-Child Interaction Therapy: Integration of Traditional and Behavior Concerns. Child Fam. Behav. Ther. 1988, 10, 33–46. [Google Scholar] [CrossRef]
- Green, J.; Charman, T.; McConachie, H.; Aldred, C.; Slonims, V.; Howlin, P.; Le Couteur, A.; Leadbitter, K.; Hudry, K.; Byford, S.; et al. Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. Lancet 2010, 375, 2152–2160. [Google Scholar] [CrossRef]
- Sanders, M.R. Triple P-Positive Parenting Program: Towards an Empirically Validated Multilevel Parenting and Family Support Strategy for the Prevention of Behavior and Emotional Problems in Children. Clin. Child Fam. Psychol. Rev. 1999, 2, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.R.; Markie-Dadds, C.; Turner, K.M.T. Practitioner’s Manual for Standard Triple P; Families International Publishing Pty Ltd.: Brisbane, Australia, 2001. [Google Scholar]
- Bögels, S.; Hoogstad, B.; Van Dun, L.; De Schutter, S.; Restifo, K. Mindfulness Training for Adolescents with Externalizing Disorders and their Parents. Behav. Cogn. Psychother. 2008, 36, 193–209. [Google Scholar] [CrossRef]
- De Bruin, E.; Blom, R.; Smit, F.M.; Van Steensel, F.J.; Bögels, S.M. MYmind: Mindfulness training for Youngsters with autism spectrum disorders and their parents. Autism 2014, 19, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Ridderinkhof, A.; De Bruin, E.I.; Blom, R.; Singh, N.N.; Bögels, S.M. Mindfulness-Based Program for Autism Spectrum Disorder: A Qualitative Study of the Experiences of Children and Parents. Mindfulness 2019, 10, 1936–1951. [Google Scholar] [CrossRef]
- Salem-Guirgis, S.; Albaum, C.; Tablon, P.; Riosa, P.B.; Nicholas, D.B.; Drmic, I.E.; Weiss, J.A. MYmind: A Concurrent Group-Based Mindfulness Intervention for Youth with Autism and Their Parents. Mindfulness 2019, 10, 1730–1743. [Google Scholar] [CrossRef]
- Ferraioli, S.J.; Harris, S.L. Comparative Effects of Mindfulness and Skills-Based Parent Training Programs for Parents of Children with Autism: Feasibility and Preliminary Outcome Data. Mindfulness 2013, 4, 89–101. [Google Scholar] [CrossRef]
- Singh, N.N.; Lancioni, G.E.; Medvedev, O.N.; Hwang, Y.-S.; Myers, R.E. A Component Analysis of the Mindfulness-Based Positive Behavior Support (MBPBS) Program for Mindful Parenting by Mothers of Children with Autism Spectrum Disorder. Mindfulness 2021, 12, 463–475. [Google Scholar] [CrossRef]
- Cheung, R.Y.M.; Leung, S.S.W.; Mak, W.W.S. Role of Mindful Parenting, Affiliate Stigma, and Parents’ Well-being in the Behavioral Adjustment of Children with Autism Spectrum Disorder: Testing Parenting Stress as a Mediator. Mindfulness 2019, 10, 2352–2362. [Google Scholar] [CrossRef]
- Singh, N.N.; Lancioni, G.E.; Karazsia, B.T.; Myers, R.E.; Hwang, Y.-S.; Anālayo, B. Effects of Mindfulness-Based Positive Behavior Support (MBPBS) Training Are Equally Beneficial for Mothers and Their Children with Autism Spectrum Disorder or With Intellectual Disabilities. Front. Psychol. 2019, 10, 385. [Google Scholar] [CrossRef]
- Torbet, S.; Proeve, M.; Roberts, R.M. Self-Compassion: A Protective Factor for Parents of Children with Autism Spectrum Disorder. Mindfulness 2019, 10, 2492–2506. [Google Scholar] [CrossRef]
- Blackledge, J.T.; Hayes, S.C. Using Acceptance and Commitment Training in the Support of Parents of Children Diagnosed with Autism. Child Fam. Behav. Ther. 2006, 28, 1–18. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Koizumi, H. The concept of ‘developing the brain’: A new natural science for learning and education. Brain Dev. 2004, 26, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Rafferty, D.; Tidman, L.; Ekas, N.V. Parenting experiences of fathers of children with autism spectrum disorder with or without intellectual disability. J. Intellect. Disabil. Res. 2020, 64, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Palomo, R. Autismo: Teorías Explicativas Actuales; Alianza Editorial: Madrid, Spain, 2017. [Google Scholar]
- Rogers, S.J.; Pennington, B.F. A theoretical approach to the deficits in infantile autism. Dev. Psychopathol. 1991, 3, 137–162. [Google Scholar] [CrossRef]
- Thomas, M.S.C.; Annaz, D.; Ansari, D.; Scerif, G.; Jarrold, C.; Karmiloff-Smith, A. Using Developmental Trajectories to Understand Developmental Disorders. J. Speech Lang. Hear. Res. 2009, 52, 336–358. [Google Scholar] [CrossRef]
- BakerDaniel, J.K.; Messinger, D.S.; Lyons, K.K.; Grantz, C.J. A Pilot Study of Maternal Sensitivity in the Context of Emergent Autism. J. Autism Dev. Disord. 2010, 40, 988–999. [Google Scholar] [CrossRef]
- APA. Diagnóstic and Statistical Manual of Mental Disorders, 4th Revised ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Bergomi, C.; Tschacher, W.; Kupper, Z. The Assessment of Mindfulness with Self-Report Measures: Existing Scales and Open Issues. Mindfulness 2013, 4, 191–202. [Google Scholar] [CrossRef]
- Sauer, S.; Walach, H.; Schmidt, S.; Hinterberger, T.; Lynch, S.; Büssing, A.; Kohls, N. Assessment of Mindfulness: Review on State of the Art. Mindfulness 2012, 4, 3–17. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef]
- Soler, J.; Tejedor, R.; Feliu-Soler, A.; Pascual, J.; Cebolla, A.; Soriano, E.; Alvarez, E.; Perez, V. Proiedades Pscométricas de la versión española de la escala Minful Attention Awareness Scale (MASS). Actas Españolas Psiquiatr. 2012, 40, 18–25. Available online: https://www.actaspsiquiatria.es/repositorio/14/75/ESP/14-75-ESP-19-26-544515.pdf (accessed on 15 December 2017).
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation: Sidney, Australia, 1995. [Google Scholar]
- Román, F.; Santibáñez, P.; Vinet, E.V. Use of the Depression Anxiety Stress Scales (DASS-21) as Screening Tests in Clinical Youngsters. Acta Investig. Psicol. 2016, 6, 2325–2336. Available online: http://www.redalyc.org/articulo.oa?id=358945983008 (accessed on 15 December 2017). [CrossRef]
- Daza, P.; Novy, D.M.; Stanley, M.A.; Averill, P. The Depression Anxiety Stress Scale-21: Spanish Translation and Validation with a Hispanic Sample. J. Psychopathol. Behav. Assess. 2002, 24, 195–205. [Google Scholar] [CrossRef]
- Bados, A.; Solanas, A.; Andrés, R. Psychometric properties of the Spanish version of Depression, Anxiety and Stress Scales (DASS). Psicothema 2005, 17, 679–683. Available online: http://www.psicothema.com/pdf/3165.pdf (accessed on 17 December 2017).
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Larsen, R.J.; Diener, E.; Emmons, R.A. An evaluation of subjective well-being measures. Soc. Indic. Res. 1985, 17, 1–17. [Google Scholar] [CrossRef]
- Lucas, R.E.; Diener, E.; Suh, E. Discriminant validity of well-being measures. J. Pers. Soc. Psychol. 1996, 71, 616–628. [Google Scholar] [CrossRef] [PubMed]
- Atienza, F.L.; Pons, D.; Balaguer, I.; Garcia-Merita, M. Propiedades psicométricas de la escala de satisfacción con la vida en adolescents. Psicothema 2000, 12, 314–319. Available online: http://www.psicothema.com/pdf/296.pdf (accessed on 16 December 2017).
- Burgess, D.J.; Beach, M.C.; Saha, S. Mindfulness practice: A promising approach to reducing the effects of clinician implicit bias on patients. Patient Educ. Couns. 2017, 100, 372–376. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; de Torrijos, F.; Skillings, A.H.; Blacker, M.; Mumford, G.T.; Alvares, D.L.; Santorelli, S.; Rosal, M.C. Delivery and Effectiveness of a Dual Language (English/Spanish) Mindfulness-Based Stress Reduction (MBSR). Mindfulness Compassion 2016, 1, 2–13. [Google Scholar] [CrossRef]
- Germer, C.K. The Mindful Path to Self-Compassion: Freeing Yourself from Destructive Thoughts and Emotions; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Neff, K.D. Self-Compassion; William Morrow: New York, NY, USA, 2011. [Google Scholar]
- Neff, K.D.; Tirch, D. Self-compassion and ACT. In The Context Press Mindfulness and Acceptance Practica Series. Mindfulness, Acceptance, and Positive Psychology: The Seven Foundations of Well-Being; New Harbinger Publications Inc.: Oakland, CA, USA, 2013; pp. 78–106. [Google Scholar]
- Abdollahi, A.; Allen, K.A.; Taheri, A. Moderating the Role of Self-Compassion in the Relationship between Perfectionism and Depression. J. Ration. Cogn. Ther. 2020, 38, 459–471. [Google Scholar] [CrossRef]
- Neff, K.D.; Faso, D.J. Self-Compassion and Well-Being in Parents of Children with Autism. Mindfulness 2015, 6, 938–947. [Google Scholar] [CrossRef]
- Davidson, R.J.; Kaszniak, A.W. Conceptual and methodological issues in research on mindfulness and meditation. Am. Psychol. 2015, 70, 581–592. [Google Scholar] [CrossRef]
- Robertson, K. Active listening: More than just paying attention. Aust. Fam. Physician 2005, 34, 1053–1055. Available online: https://www.racgp.org.au/afpbackissues/2005/200512/200512robinson.pdf (accessed on 12 January 2018).
- Rogers, C.R.; Farson, R.E. Active Listening; Industrial Relations Center of the University of Chicago: Chicago, IL, USA, 1957. [Google Scholar]
- Mitchell, M.L.; Jolley, J.M. Research Design Explained, 7th ed.; Wadsworth Cengage Learning: Belmont, CA, USA, 2010. [Google Scholar]
- Pérez, J.; Pérez, M.; Montealegre, M.D.P.; Perea, L.P. Estrés Parental, Desarrollo Infantil y Atención Temprana. INFAD Rev. Psicol. 2012, 1, 123–132. [Google Scholar]
- Suárez, M.; Rodríguez, M.D.C.; Castro, A. La discapacidad auditiva: Impacto en la familia e importancia del apoyo social. Qurriculum Rev. Teoría Investig. Práct. Educ. 2006, 19, 221–232. [Google Scholar]
- Basa, J.A. Estrés Parental con Hijos Autistas: Un Estudio Comparativo; Biblioteca Digital de la Universidad Católica Argentina: Buenos Aires, Argentina, 2010. [Google Scholar]
- Giné, C. Familia e intervención precoz. Orientaciones para la intervención del psicopedagogo. In Presente y Futuro del Trabajo del Psicopedagogo; Editorial Ariel: Barcelona, Spain, 2001. [Google Scholar]
- Hamilton, L.M. Facing Autism: Giving Parents Reasons for Hope and Guidance for Help; Ramdom House Digital, Inc.: New York, NY, USA, 2008. [Google Scholar]
- Whitaker, P. Supporting Families of Preschool Children with Autism. Autism 2002, 6, 411–426. [Google Scholar] [CrossRef]
- Singh, N.N.; Lancioni, G.E.; Winton, A.S.W.; Karazsia, B.T.; Myers, R.E.; Latham, L.L.; Singh, J. Mindfulness-Based Positive Behavior Support (MBPBS) for Mothers of Adolescents with Autism Spectrum Disorder: Effects on Adolescents’ Behavior and Parental Stress. Mindfulness 2014, 5, 646–657. [Google Scholar] [CrossRef]
- Ruiz-Robledillo, N.; Sariñana-González, P.; Pérez-Blasco, J.; González-Bono, E.; Moya-Albiol, L. A Mindfulness-Based Program Improves Health in Caregivers of People with Autism Spectrum Disorder: A Pilot Study. Mindfulness 2014, 6, 767–777. [Google Scholar] [CrossRef]
- Orue, I.; Calvete, E.; Fernández-González, L.; Gómez-Odriozola, J.; Royuela-Colomer, E.; Cortázar, N. A spanish adapta-tion of the Mindfulness in parenting questionnaire. Psicothema 2020, 32, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Abidin, R.R. Parenting Stress Index, 4th ed.; PSI-4; Psychological Assessment Resources: Lutz, FL, USA, 2012. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fathers | Mothers | Children | Level Severity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Age | Mean (SD) | Age | Mean (SD) | Age | Mean (SD) | 1 | 2 | 3 | |
| Group A | 5 | 40–45 | 43.33 (1.75) | 37–43 | 39.83 (2.48) | 3–12 | 5.33 (0.63) | 4 | 1 | 0 |
| Group B | 5 | 37–48 | 42.25 (4.14) | 33–46 | 40.00 (5.10) | 4–10 | 6.90 (3.10) | 4 | 1 | 0 |
| WEEK N | Part 1: Mindfulness Session | Part 2: Psychoeducational |
|---|---|---|
| 1 | Topic: Introduction to Mindfulness Practice: “Grape meditation” | What is autism? |
| 2 | Topic: Basic awareness Practice: Introduction to body mapping technique | Causes of autism |
| 3 | Topic: The importance of mindfulness to “change” our brain. Practice: Sitting Meditation | Intervention Methods in ASD |
| 4 | Topic: Self-control of thoughts. Practice: Introduction to yoga as a technique of mind-body integration. | Intensity or quality of the intervention in ASD. How and who? |
| 5 | Topic: How to “own” our own stress. Practice: Intermediation of automatic reactions through mindfulness | Primary and secondary school for ASD patients and parents |
| 6 | Topic: How to be aware of our difficult emotions or sensations before they generate consequences? Practice: Meditation to Calm, Allow and Accept | ASD Adolescence |
| 7 | Topic: Mindfulness and improving our communication Practice: meditation on conscious and present communication | Access to Work for ASD |
| 8 | Topic: Mindfulness and Self-Compassion Empathy Practice: Meditation on empathy and compassion to reduce the consequences of self-centeredness in stress | Autonomy Development and Self-Determination in ASD |
| Assessment Time | ||||
|---|---|---|---|---|
| Measure 1 | Measure 2 | Measure 3 | ||
| Mean (SD) | Mean (SD) | Mean (SD) | ||
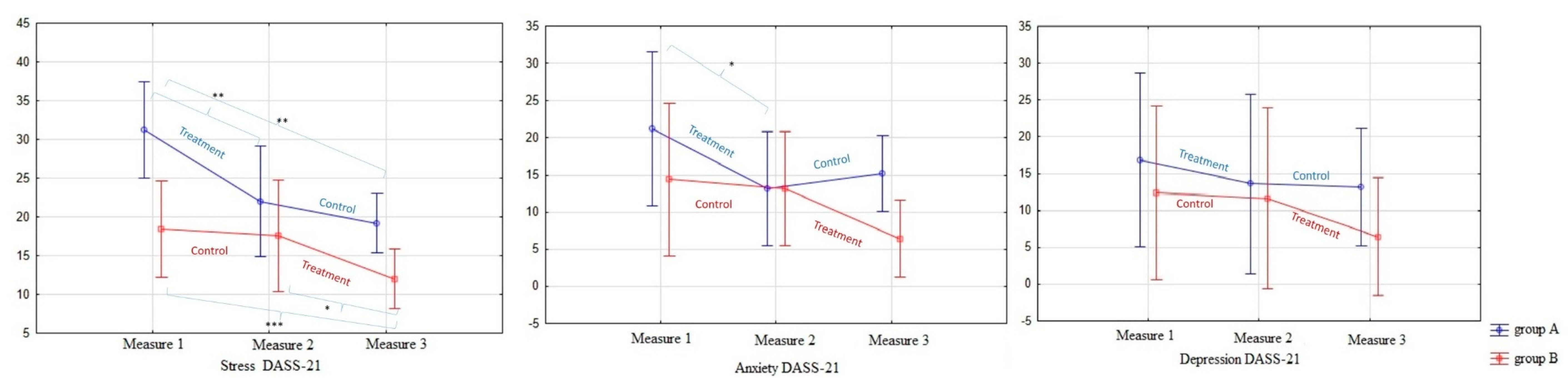
| DASS-Stress | Group A | 31.2 (4.1) | 22.0 (4.0) | 19.2 (4.1) |
| Group B | 18.4 (7.4) | 17.6 (9.0) | 12.0 (3.2) | |
| DASS-Anxiety | Group A | 21.2 (6.4) | 13.0 (6.4) | 15.2 (4.8) |
| Group B | 14.4 (12.6) | 13.2 (8.3) | 6.4 (5.2) | |
| DASS-Depression | Group A | 16.8 (6.9) | 13.6 (9.7) | 13.2 (9.7) |
| Group B | 12.4 (14.6) | 11.6 (13.7) | 6.4 (5.2) | |
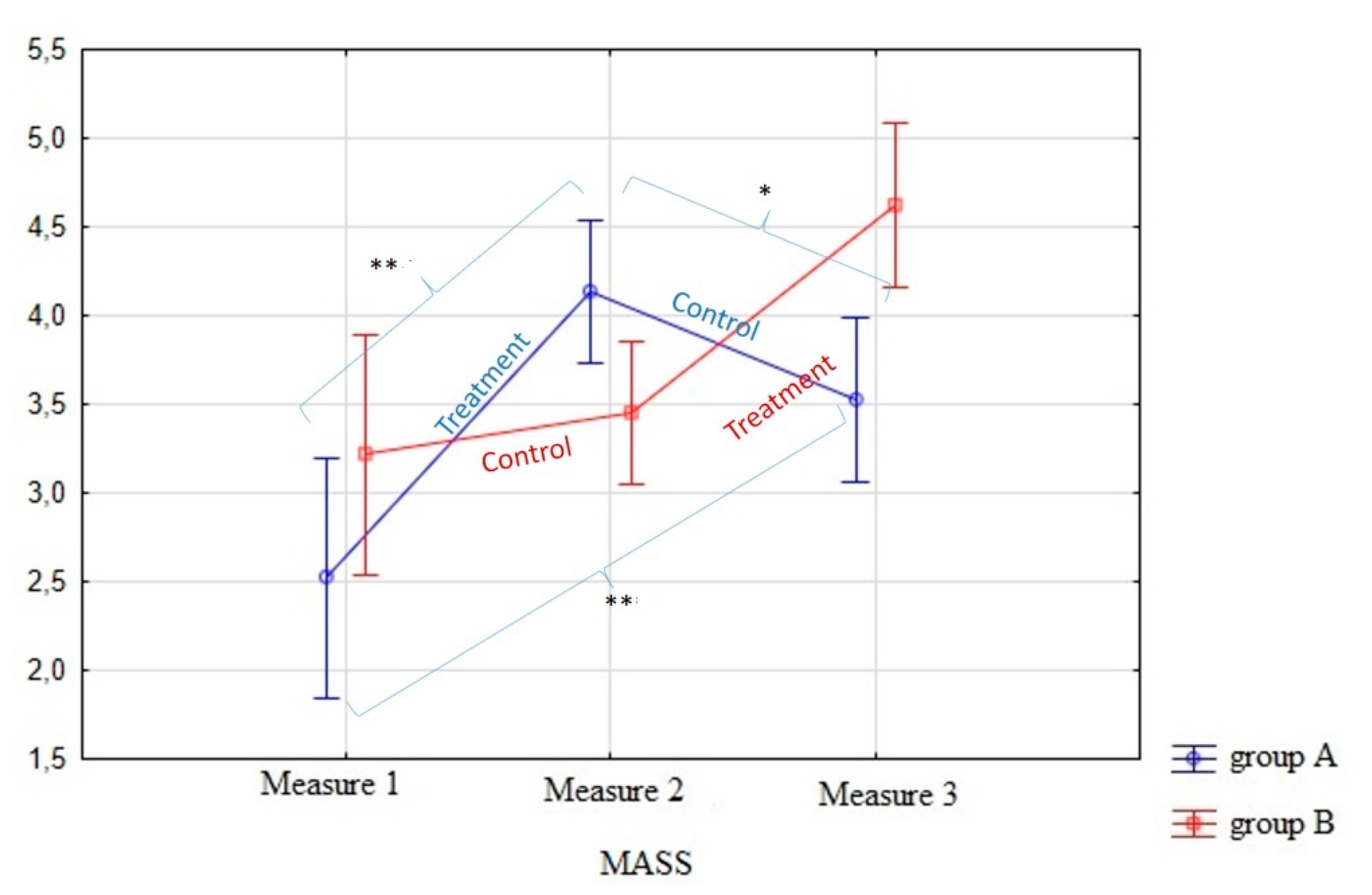
| MASS | Group A | 2.5 (0.86) | 4.1 (0.43) | 3.5 (0.61) |
| Group B | 3.2 (0.35) | 3.5 (0.35) | 4.6 (0.19) | |
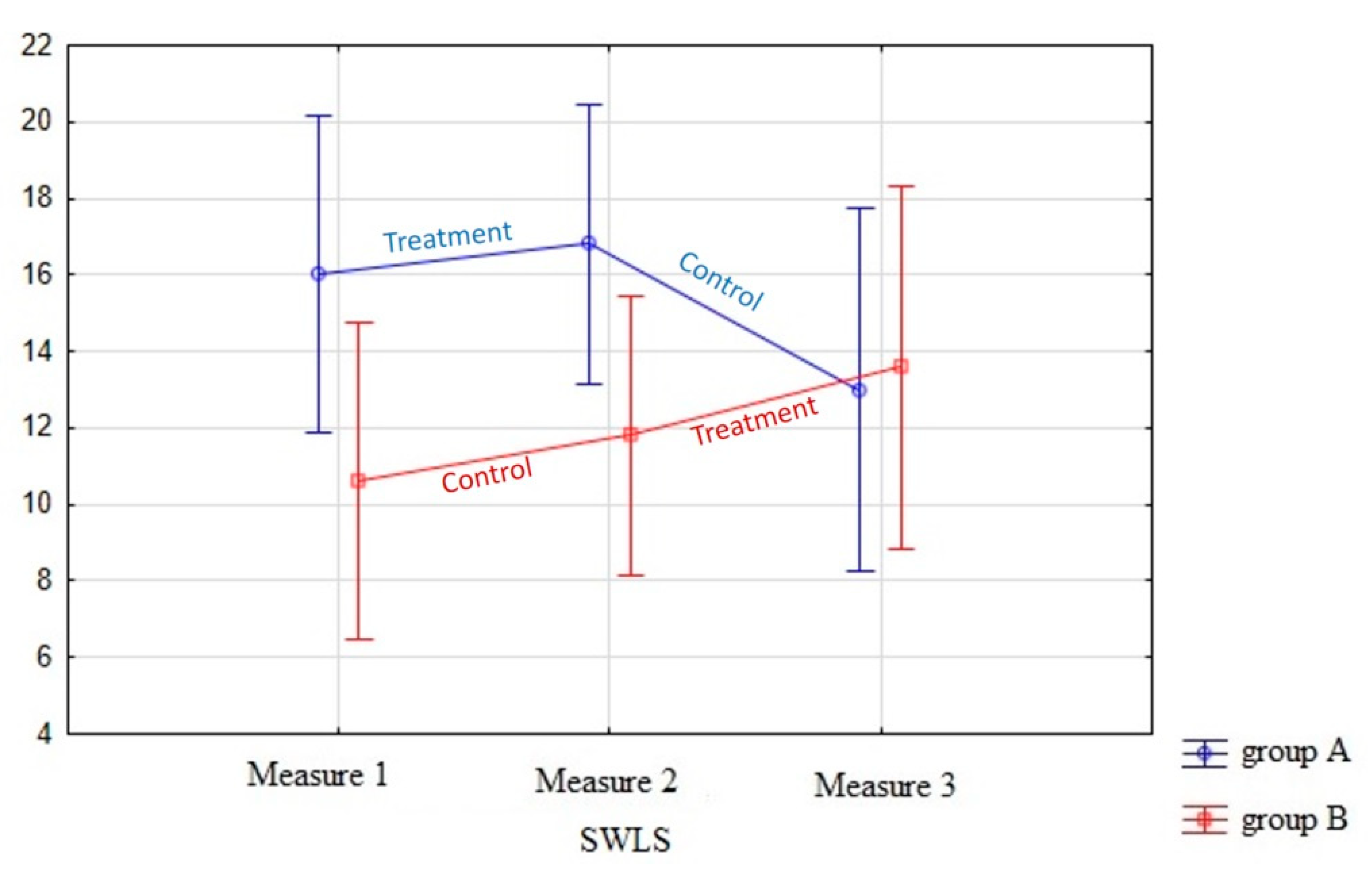
| SWLS | Group A | 16.0 (3.7) | 16.8 (3.1) | 13.0 (3.9) |
| Group B | 10.6 (4.3) | 11.8 (3.9) | 13.6 (5.2) | |
| ANOVA Reapeated Measures | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | Assessment Time | Assessment Time × Group | |||||||
| F | p | η 2 | F | p | η 2 | F | p | η 2 | |
| DASS-Stress | 7.21 | 0.03 * | 0.47 | 14.5 | 0.00 ** | 0.64 | 3.1 | 0.07 | 0.28 |
| DASS-Anxiety | 1.85 | 0.21 | 0.19 | 3.6 | 0.05 * | 0.31 | 1.5 | 0.25 | 0.16 |
| DASS-Depression | 0.51 | 0.49 | 0.06 | 2.5 | 0.11 | 0.24 | 0.62 | 0.55 | 0.07 |
| MASS | 1.67 | 0.23 | 0.17 | 50.4 | 0.00 ** | 0.86 | 27.6 | 0.00 ** | 0.78 |
| SWLS | 2.12 | 0.18 | 0.21 | 0.55 | 0.58 | 0.06 | 4.7 | 0.02 | 0.37 |
| Measures | 1 | 2 | 3 | |
|---|---|---|---|---|
| 1 | DASS-Stress | 0.00 ** | 0.00 ** | |
| DASS-Anxiety | 0.04 * | 0.08 | ||
| DASS-Depresion | 0.19 | 0.11 | ||
| MASS | 0.00 ** | 0.00 ** | ||
| SWLS | 0.34 | 1.0 | ||
| 2 | DASS-Stress | 0.00 ** | 0.05 * | |
| DASS-Anxiety | 0.04 * | 0.32 | ||
| DASS-Depresion | 0.19 | 0.23 | ||
| MASS | 0.00 ** | 0.05 * | ||
| SWLS | 0.34 | 0.19 | ||
| 3 | DASS-Stress | 0.00 ** | 0.05 * | |
| DASS-Anxiety | 0.08 | 0.32 | ||
| DASS-Depresion | 0.11 | 0.23 | ||
| MASS | 0.00 ** | 0.05 * | ||
| SWLS | 1.0 | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas-Torres, L.P.; Alonso-Esteban, Y.; López-Ramón, M.F.; Alcantud-Marín, F. Mindfulness-Based Stress Reduction (MBSR) and Self Compassion (SC) Training for Parents of Children with Autism Spectrum Disorders: A Pilot Trial in Community Services in Spain. Children 2021, 8, 316. https://doi.org/10.3390/children8050316
Rojas-Torres LP, Alonso-Esteban Y, López-Ramón MF, Alcantud-Marín F. Mindfulness-Based Stress Reduction (MBSR) and Self Compassion (SC) Training for Parents of Children with Autism Spectrum Disorders: A Pilot Trial in Community Services in Spain. Children. 2021; 8(5):316. https://doi.org/10.3390/children8050316
Chicago/Turabian StyleRojas-Torres, Liliana Paulina, Yurena Alonso-Esteban, María Fernanda López-Ramón, and Francisco Alcantud-Marín. 2021. "Mindfulness-Based Stress Reduction (MBSR) and Self Compassion (SC) Training for Parents of Children with Autism Spectrum Disorders: A Pilot Trial in Community Services in Spain" Children 8, no. 5: 316. https://doi.org/10.3390/children8050316
APA StyleRojas-Torres, L. P., Alonso-Esteban, Y., López-Ramón, M. F., & Alcantud-Marín, F. (2021). Mindfulness-Based Stress Reduction (MBSR) and Self Compassion (SC) Training for Parents of Children with Autism Spectrum Disorders: A Pilot Trial in Community Services in Spain. Children, 8(5), 316. https://doi.org/10.3390/children8050316