
Creatinine Trends and Patterns in Neonates Undergoing Whole Body Hypothermia: A Systematic Review

 , and
, and 
Abstract
:1. Introduction: Perinatal Asphyxia, Whole Body Hypothermia, and Renal Impairment
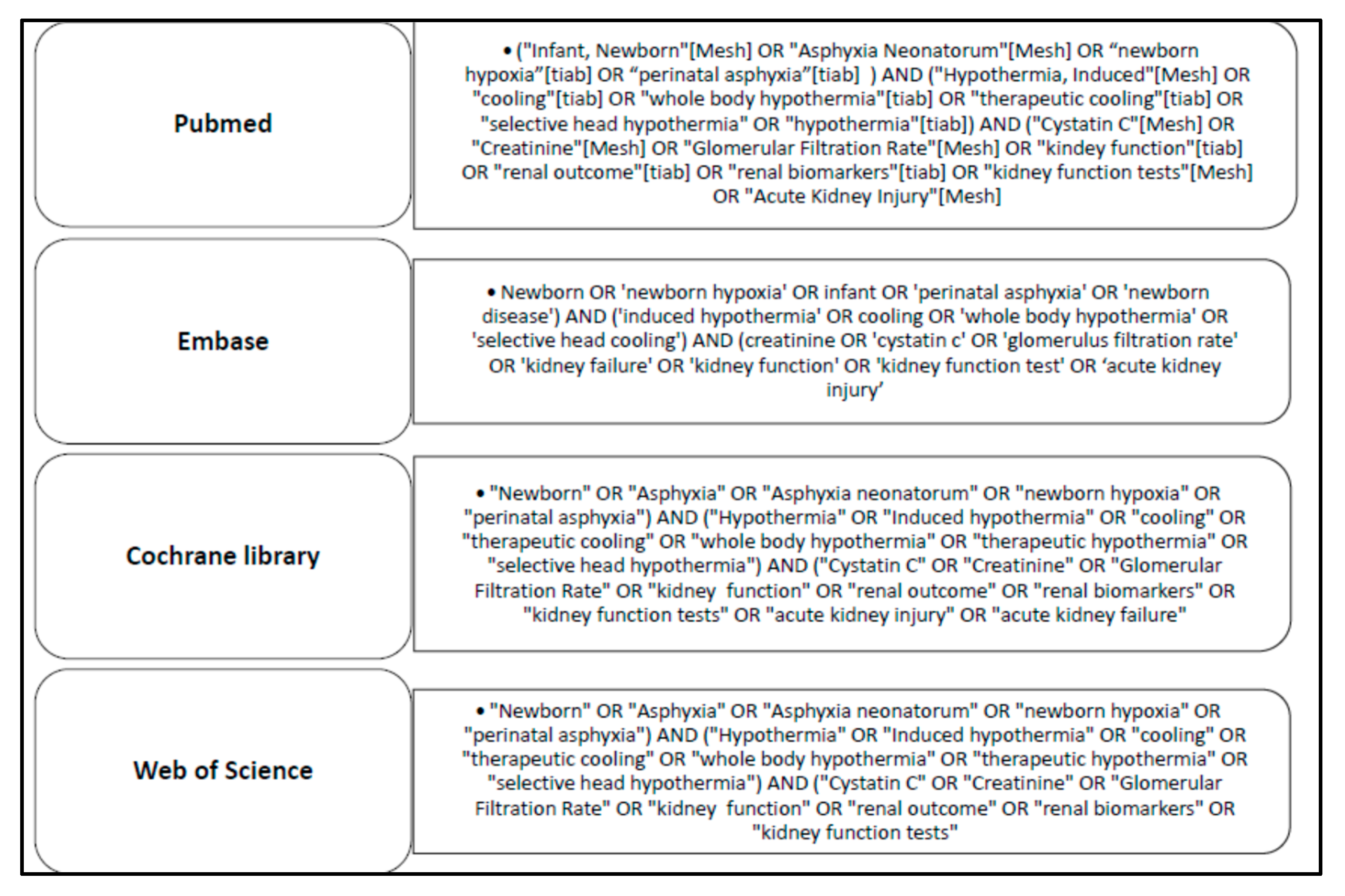
2. Materials and Methods
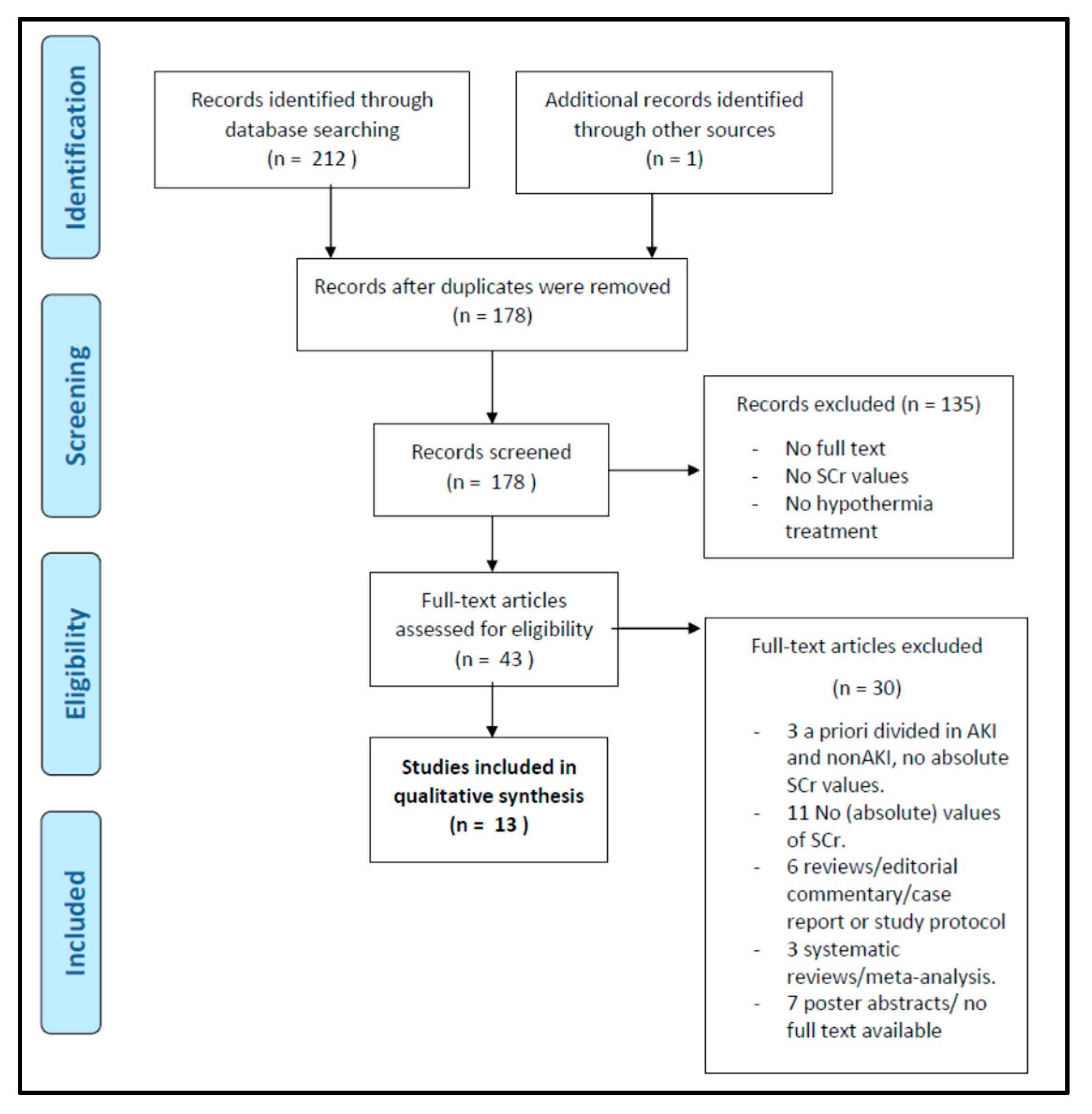
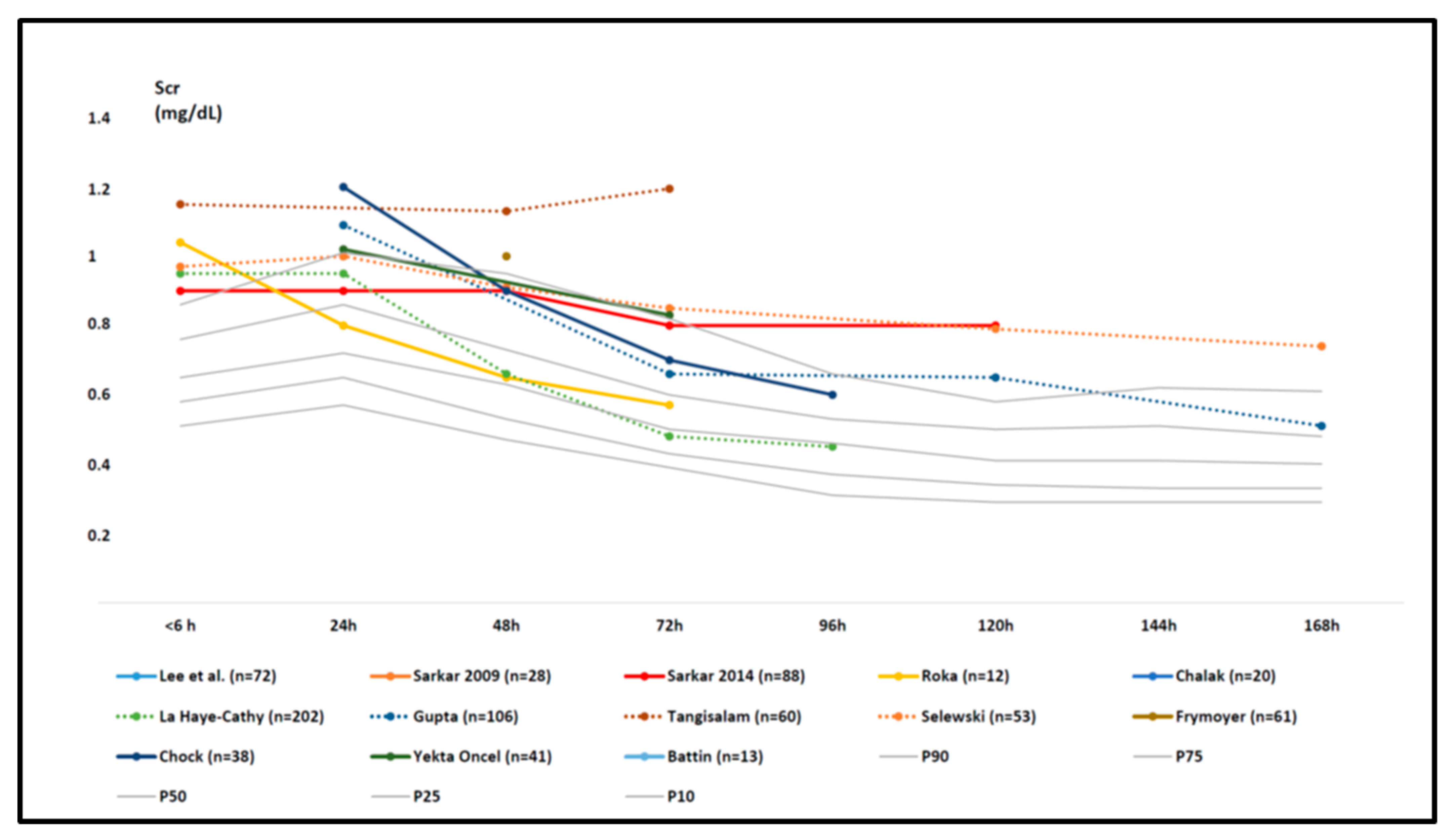
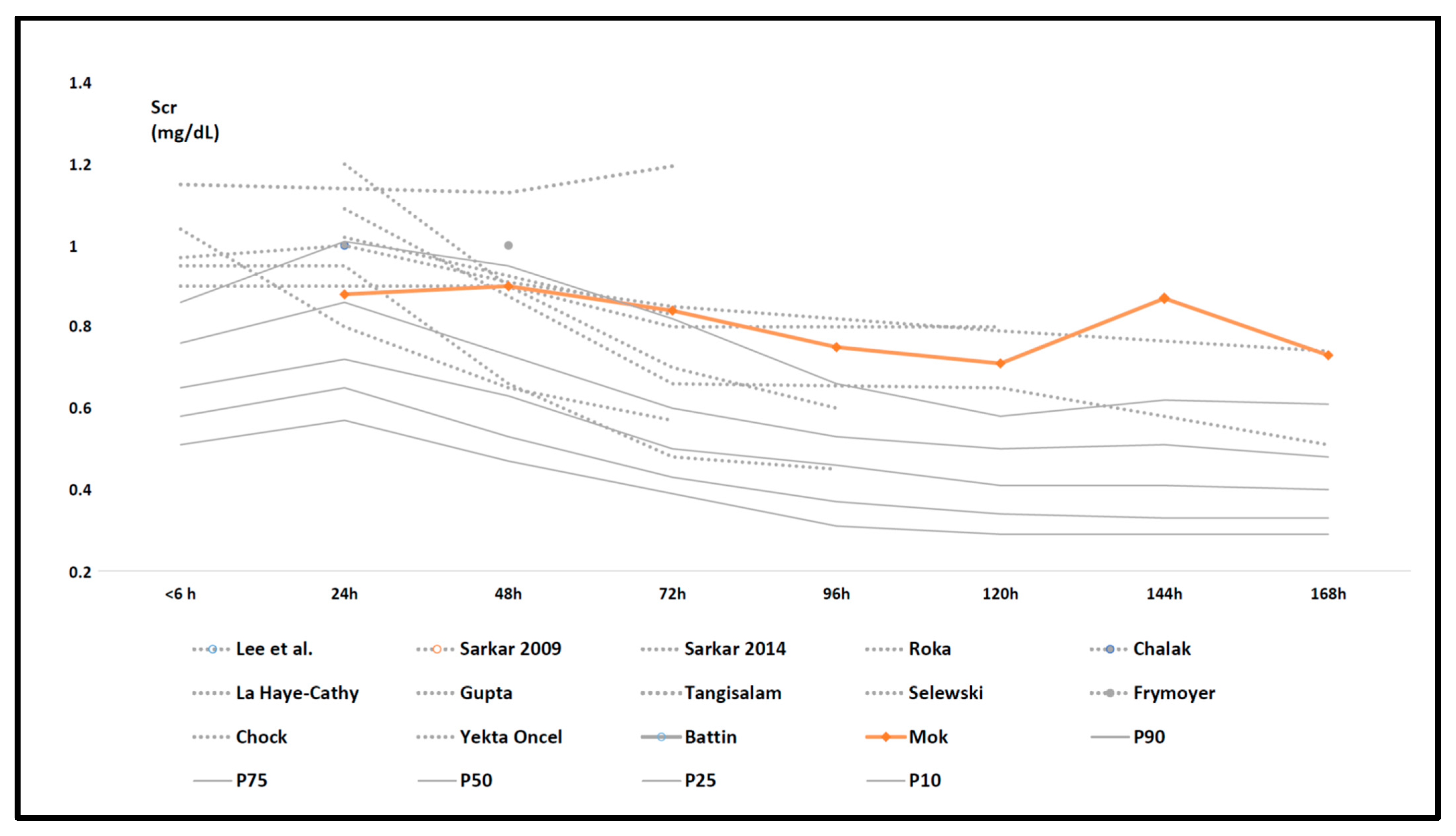
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Greco, P.; Nencini, G.; Piva, I.; Scioscia, M.; Volta, C.A.; Spadaro, S.; Neri, M.; Bonaccorsi, G.; Greco, F.; Cocco, I.; et al. Pathophysiology of hypoxic-ischemic encephalopathy: A review of the past and a view on the future. Acta Neurol. Belg. 2020, 120, 277–288. [Google Scholar] [CrossRef]
- Nair, J.; Kumar, V.H.S. Current and emerging therapies in the management of hypoxic ischemic encephalopathy in neonates. Children 2018, 5, 99. [Google Scholar] [CrossRef] [Green Version]
- Michniewicz, B.; Szpecht, D.; Sowińska, A.; Sibiak, R.; Szymankiewicz, M.; Gadzinowski, J. Biomarkers in newborns with hypoxic-ischemic encephalopathy treated with therapeutic hypothermia. Childs Nerv. Syst. 2020, 36, 2981–2988. [Google Scholar] [CrossRef]
- Niermeyer, S. Improving global newborn survival: Building upon helping babies breathe. Neonatology 2020, 117, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Abate, B.B.; Bimerew, M.; Gebremichael, B.; Mengesha Kassie, A.; Kassaw, M.; Gebremeskel, T.; Bayih, W.A. Effects of therapeutic hypothermia on death among asphyxiated neonates with hypoxic-ischemic encephalopathy: A systematic review and meta-analysis of randomized control trials. PLoS ONE 2021, 16, e0247229. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-J.; Zhang, Z.-Y.; Fan, B.; Li, G.-Y. Neuroprotection by therapeutic hypothermia. Front. Neurosci. 2019, 13, 586. [Google Scholar] [CrossRef]
- Walas, W.; Wilińska, M.; Bekiesińska-Figatowska, M.; Halaba, Z.; Śmigiel, R. Methods for assessing the severity of perinatal asphyxia and early prognostic tools in neonates with hypoxic—ischemic encephalopathy treated with therapeutic hypothermia. Adv. Clin. Exp. Med. 2020, 29, 1011–1016. [Google Scholar] [CrossRef]
- Solevåg, A.L.; Schmölzer, G.M.; Cheung, P.-Y. Novel interventions to reduce oxidative-stress related brain injury in neonatal asphyxia. Free Radic. Biol. Med. 2019, 142, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Kleuskens, D.G.; Gonçalves Costa, F.; Annink, K.V.; van den Hoogen, A.; Alderliesten, T.; Groenendaal, F.; Benders, M.J.N.; Dudink, J. Pathophysiology of cerebral hyperperfusion in term neonates with hypoxic-ischemic encephalopathy: A systematic review for future research. Front. Pediatr. 2021, 9, 631258. [Google Scholar] [CrossRef] [PubMed]
- Danladi, J.; Sabir, H. Perinatal infection: A major contributor to efficacy of cooling in newborns following birth asphyxia. Int. J. Mol. Sci. 2021, 22, 707. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, M.; Sweetman, D.; Bonifacio, S.L.; El-Dib, M.; Austin, T.; Molloy, E.J. Management of multi organ dysfunction in neonatal encephalopathy. Front. Pediatr. 2020, 8, 239. [Google Scholar] [CrossRef]
- Nestaas, E.; Walsh, B.H. Hypothermia and cardiovascular instability. Clin. Perinatol. 2020, 47, 575–592. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.J.; da Costa, C.S.; Austin, T.; Brady, K.M.; Czosnyka, M.; Lee, J.K. Neonatal cerebrovascular autoregulation. Pediatr. Res. 2018, 84, 602–610. [Google Scholar] [CrossRef]
- Kirkley, M.J.; Boohaker, L.; Griffin, R.; Soranno, D.E.; Gien, J.; Askenazi, D.; Gist, K.M.; On behalf of the Neonatal Kidney Collaborative (NKC). Acute kidney injury in neonatal encephalopathy: An evaluation of the AWAKEN database. Pediatr. Nephrol. 2019, 34, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Gallo, D.; de Bijl-Marcus, K.A.; Alderliesten, T.; Lilien, M.; Groenendaal, F. Early acute kidney injury in preterm and term neonates: Incidence, outcome, and associated clinical features. Neonatology 2021. [Google Scholar] [CrossRef] [PubMed]
- Charlton, J.R.; Boohaker, L.; Askenazi, D.; Brophy, P.D.; D’Angio, C.; Fuloria, M.; Gien, J.; Griffin, R.; Hingorani, S.; Ingraham, S.; et al. Incidence and risk factors of early onset neonatal AKI. Clin. J. Am. Soc. Nephrol. 2019, 14, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Cavallin, F.; Rubin, G.; Vidal, E.; Cainelli, E.; Bonadies, L.; Suppiej, A.; Trevisanuto, D. Prognostic role of acute kidney injury on long-term outcome in infants with hypoxic-ischemic encephalopathy. Pediatr. Nephrol. 2020, 35, 477–483. [Google Scholar] [CrossRef]
- Ottolini, K.M.; Basu, S.K.; Herrera, N.; Govindan, V.; Mashat, S.; Vezina, G.; Ridore, M.; Bost, J.; Chang, T.; Massaro, A.N. Positive fluid balance is associated with death and severity of brain injury in neonates with hypoxic-ischemic encephalopathy. J. Perinatol. 2021. [Google Scholar] [CrossRef]
- Jacobs, S.E.; Berg, M.; Hunt, R.; Tarnow-Mordi, W.O.; Inder, T.E.; Davis, P.G. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst. Rev. 2013, 2013, CD003311. [Google Scholar] [CrossRef] [PubMed]
- Benninger, K.L.; Inder, T.E.; Goodman, A.M.; Cotten, C.M.; Nordli, D.R.; Shah, T.A.; Slaughter, J.C.; Maitre, N.L. Perspectives from the Society for Pediatric Research. Neonatal encephalopathy clinical trials: Developing the future. Pediatr. Res. 2021, 89, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Van Wincoop, M.; de Bijl-Marcus, K.; Lilien, M.; van den Hoogen, A.; Groenendaal, F. Effect of therapeutic hypothermia on renal and myocardial function in asphyxiated (near)term neonates: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0247403. [Google Scholar] [CrossRef]
- Cristea, S.; Smits, A.; Kulo, A.; Knibbe, C.A.J.; van Weissenbruch, M.; Krekels, E.H.J.; Allegaert, K. Amikacin pharmacokinetics to optimize dosing in neonates with perinatal asphyxia treated with hypothermia. Antimicrob. Agents Chemother. 2017, 61, e01282-17. [Google Scholar] [CrossRef] [Green Version]
- Favié, L.M.A.; de Haan, T.R.; Bijleveld, Y.A.; Rademaker, C.M.A.; Egberts, T.C.G.; Nuytemans, D.H.G.M.; Mathôt, R.A.A.; Groenendaal, F.; Huitema, A.D.R. Prediction of drug exposure in critically ill encephalopathic neonates treated with therapeutic hypothermia based on a pooled population pharmacokinetic analysis of seven drugs and five metabolites. Clin. Pharmacol. Ther. 2020, 108, 1098–1106. [Google Scholar] [CrossRef]
- Bijleveld, Y.A.; de Haan, T.R.; van der Lee, H.J.; Groenendaal, F.; Dijk, P.H.; van Heijst, A.; de Jonge, R.C.; Dijkman, K.P.; van Straaten, H.L.; Rijken, M.; et al. Altered gentamicin pharmacokinetics in term neonates undergoing controlled hypothermia. Br. J. Clin. Pharmacol. 2016, 81, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Deferm, N.; Annink, K.V.; Faelens, R.; Schroth, M.; Maiwald, C.A.; el Bakkali, L.; van Bel, F.; Benders, M.J.N.L.; van Weissenbruch, M.M.; Hagen, A.; et al. Glomerular filtration rate in asphyxiated neonates under therapeutic whole-body hypothermia, quantified by mannitol clearance. Clin. Pharmacokinet. 2021. [Google Scholar] [CrossRef]
- Lutz, I.C.; Allegaert, K.; de Hoon, J.N.; Marynissen, H. Pharmacokinetics during therapeutic hypothermia for neonatal hypoxic ischaemic encephalopathy: A literature review. BMJ. Paediatr. Open 2020, 4, e000685. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K.; Smits, A.; van Donge, T.; van den Anker, J.; Sarafidis, K.; Levtchenko, E.; Mekahli, D. Renal precision medicine in neonates and acute kidney injury: How to convert a cloud of creatinine observations to support clinical decisions. Front. Pediatr. 2020, 8, 366. [Google Scholar] [CrossRef]
- Filler, G.; Bhayana, V.; Schott, C.; Díaz-González de Ferris, M.E. How should we assess renal function in neonates and infants? Acta Paediatr. 2021, 110, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Iacobelli, S.; Guignard, J.P. Maturation of glomerular filtration rate in neonates and infants: An overview. Pediatr. Nephrol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Muhari-Stark, E.; Burckart, G.J. Glomerular filtration rate estimation formulas for pediatric and neonatal use. J. Pediatr. Pharmacol. Ther. 2018, 23, 424–431. [Google Scholar] [CrossRef]
- Go, H.; Momoi, N.; Kashiwabara, N.; Haneda, K.; Chishiki, M.; Imamura, T.; Sato, M.; Goto, A.; Kawasaki, Y.; Hosoya, M. Neonatal and maternal serum creatinine levels during the early postnatal period in preterm and term infants. PLoS ONE 2018, 13, e0196721. [Google Scholar] [CrossRef] [Green Version]
- Allegaert, K.; Pauwels, S.; Smits, A.; Crèvecoeur, K.; van den Anker, J.; Mekahli, D.; Vermeersch, P. Enzymatic isotope dilution mass spectrometry (IDMS) traceable serum creatinine is preferable over Jaffe in neonates and young infants. Clin. Chem. Lab. Med. 2014, 52, e107–e109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohatgi, A. Available online: https://automeris.io/WebPlotDigitizer (accessed on 18 April 2021).
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the reporting of observational studies in epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.K.; Perin, J.; Parkinson, C.; O’Connor, M.; Gilmore, M.M.; Reyes, M.; Armstrong, J.; Jennings, J.M.; Northington, F.J.; Chavez-Valdez, R. Relationships between cerebral autoregulation and markers of kidney and liver injury in neonatal encephalopathy and therapeutic hypothermia. J. Perinatol. 2017, 37, 938–942. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, S.; Barks, J.D.; Bhagat, I.; Donn, S.M. Effects of therapeutic hypothermia on multiorgan dysfunction in asphyxiated newborns: Whole-body cooling versus selective head cooling. J. Perinatol. 2009, 29, 558–563. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, S.; Askenazi, D.J.; Jordan, B.K.; Bhagat, I.; Bapuraj, J.R.; Dechert, R.E.; Selewski, D.T. Relationship between acute kidney injury and brain MRI findings in asphyxiated newborns after therapeutic hypothermia. Pediatr. Res. 2014, 75, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Róka, A.; Vásárhelyi, B.; Bodrogi, E.; Machay, T.; Szabó, M. Changes in laboratory parameters indicating cell necrosis and organ dysfunction in asphyxiated neonates on moderate systemic hypothermia. Acta Paediatr. 2007, 96, 1118–1121. [Google Scholar] [CrossRef]
- Chalak, L.F.; Sánchez, P.J.; Adams-Huet, B.; Laptook, A.R.; Heyne, R.J.; Rosenfeld, C.R. Biomarkers for severity of neonatal hypoxic-ischemic encephalopathy and outcomes in newborns receiving hypothermia therapy. J. Pediatr. 2014, 164, 468–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Haye-Caty, N.; Barbosa Vargas, S.; Maluorni, J.; Rampakakis, E.; Zappitelli, M.; Wintermark, P. Impact of restricting fluid and sodium intake in term asphyxiated newborns treated with hypothermia. J. Matern. Fetal Neonatal Med. 2020, 33, 3521–3528. [Google Scholar] [CrossRef]
- Gupta, C.; Massaro, A.N.; Ray, P.E. A new approach to define acute kidney injury in term newborns with hypoxic ischemic encephalopathy. Pediatr. Nephrol. 2016, 31, 1167–1178. [Google Scholar] [CrossRef] [PubMed]
- Tanigasalam, V.; Bhat, V.; Adhisivam, B.; Sridhar, M.G. Does therapeutic hypothermia reduce acute kidney injury among term neonates with perinatal asphyxia? --a randomized controlled trial. J. Matern. Fetal Neonatal Med. 2016, 29, 2544–2547. [Google Scholar] [CrossRef] [PubMed]
- Selewski, D.T.; Jordan, B.K.; Askenazi, D.J.; Dechert, R.E.; Sarkar, S. Acute kidney injury in asphyxiated newborns treated with therapeutic hypothermia. J. Pediatr. 2013, 162, 725–729. [Google Scholar] [CrossRef]
- Frymoyer, A.; Lee, S.; Bonifacio, S.L.; Meng, L.; Lucas, S.S.; Guglielmo, B.J.; Sun, Y.; Verotta, D. Every 36-h gentamicin dosing in neonates with hypoxic-ischemic encephalopathy receiving hypothermia. J. Perinatol. 2013, 33, 778–782. [Google Scholar] [CrossRef] [Green Version]
- Chock, V.Y.; Frymoyer, A.; Yeh, C.G.; Van Meurs, K.P. Renal saturation and acute kidney injury in neonates with hypoxic ischemic encephalopathy undergoing therapeutic hypothermia. J. Pediatr. 2018, 200, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Oncel, M.Y.; Canpolat, F.E.; Arayici, S.; Alyamac Dizdar, E.; Uras, N.; Oguz, S.S. Urinary markers of acute kidney injury in newborns with perinatal asphyxia. Ren Fail. 2016, 38, 882–888. [Google Scholar] [CrossRef] [Green Version]
- Battin, M.R.; Penrice, J.; Gunn, T.R.; Gunn, A.J. Treatment of term infants with head cooling and mild systemic hypothermia (35.0 ℃ and 34.5 ℃) after perinatal asphyxia. Pediatrics 2003, 111, 244–251. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Wyatt, J.S.; Azzopardi, D.; Ballard, R.; Edwards, A.D.; Ferriero, D.M.; Polin, R.A.; Robertson, C.M.; Thoresen, M.; Whitelaw, A.; et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: Multicentre randomised trial. Lancet 2005, 365, 663–670. [Google Scholar] [CrossRef]
- Azzopardi, D.; Strohm, B.; Marlow, N.; Brocklehurst, P.; Deierl, A.; Eddama, O.; Goodwin, J.; Halliday, H.L.; Juszczak, E.; Kapellou, O.; et al. Effects of hypothermia for perinatal asphyxia on childhood outcomes. N. Engl. J. Med. 2014, 371, 140–149. [Google Scholar] [CrossRef] [Green Version]
- Azzopardi, D.; Brocklehurst, P.; Edwards, D.; Halliday, H.; Levene, M.; Thoresen, M.; Whitelaw, A.; TOBY Study Group. The TOBY Study. Whole body hypothermia for the treatment of perinatal asphyxial encephalopathy: A randomised controlled trial. BMC Pediatr. 2008, 8, 17. [Google Scholar] [CrossRef] [Green Version]
- Allegaert, K.; Smits, A.; Mekahli, D.; van den Anker, J.N. Creatinine at birth correlates with gestational age and birth weight: Another factor of the imbroglio in early neonatal life. Neonatology 2020, 117, 637–640. [Google Scholar] [CrossRef]
- Bueva, A.; Guignard, J.P. Renal function in preterm neonates. Pediatr. Res. 1994, 36, 572–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perazzo, S.; Revenis, M.; Massaro, A.; Short, B.L.; Ray, P.E. A new approach to recognize neonatal impaired kidney function. Kidney Int. Rep. 2020, 5, 2301–2312. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.Y.D.; Tseng, M.-H.; Lee, J.-C.; Chou, Y.-C.; Lien, R.; Lai, M.-Y.; Lee, C.-C.; Lin, J.-J.; Chou, I.-J.; Lin, K.-L.; et al. A retrospective study on the incidence of acute kidney injury and its early prediction using troponin-I in cooled asphyxiated neonates. Sci. Rep. 2020, 10, 15682. [Google Scholar] [CrossRef] [PubMed]
- Jetton, J.G.; Boohaker, L.J.; Sethi, S.K.; Wazir, S.; Rohatgi, S.; Soranno, D.E.; Chishti, A.S.; Woroniecki, R.; Mammen, C.; Swanson, J.R.; et al. Incidence and outcomes of neonatal acute kidney injury (AWAKEN): A multicenter, multinational, observational cohort study. Lancet Child Adolesc. Health 2017, 1, 184–194. [Google Scholar] [CrossRef]
- Kavanaugh, K.J.; Jetton, J.G.; Kent, A.L. Neonatal acute kidney injury: Understanding of the impact on the smallest patients. Crit. Care Clin. 2021, 37, 349–363. [Google Scholar] [CrossRef]
- Kandasamy, Y.; Rudd, D. Cystatin C: A more reliable biomarker of renal function in young infants? A longitudinal cohort study. Acta Paediatr. 2021, 110, 1341–1345. [Google Scholar] [CrossRef]
- Allegaert, K.; Mekahli, D.; van den Anker, J. Cystatin C in newborns: A promising renal biomarker in search for standardization and validation. J. Matern. Fetal Neonatal Med. 2015, 28, 1833–1888. [Google Scholar] [CrossRef] [Green Version]
- Hage, L.; Jeyakumaran, D.; Dorling, J.; Ojha, S.; Sharkey, D.; Longford, N.; Modi, N.; Battersby, C.; Gale, C. Changing clinical characteristics of infants treated for hypoxic-ischaemic encephalopathy in England, Wales and Scotland: A population-based study using the National Neonatal Research Database. Arch. Dis. Child. Fetal Neonatal Ed. 2021. [Google Scholar] [CrossRef]
- Quirke, F.A.; Healy, P.; Bhraonáin, E.N.; Daly, M.; Biesty, L.; Hurley, T.; Walker, K.; Meher, S.; Haas, D.M.; Bloomfield, F.H.; et al. COHESION: Core outcomes in neonatal encephalopathy (protocol). Trials 2021, 22, 125. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| <6 h | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | |
|---|---|---|---|---|---|---|---|---|
| P90 | 0.86 | 1.01 | 0.95 | 0.82 | 0.66 | 0.58 | 0.62 | 0.61 |
| P75 | 0.76 | 0.86 | 0.73 | 0.6 | 0.53 | 0.5 | 0.51 | 0.48 |
| P50 | 0.65 | 0.72 | 0.63 | 0.5 | 0.46 | 0.41 | 0.41 | 0.4 |
| P25 | 0.58 | 0.65 | 0.53 | 0.43 | 0.37 | 0.34 | 0.33 | 0.33 |
| P10 | 0.51 | 0.57 | 0.47 | 0.39 | 0.31 | 0.29 | 0.29 | 0.29 |
| Number | 293 | 239 | 215 | 213 | 160 | 129 | 106 | 101 |
| Author | n | Study Design | HIE Diagnosis | Hypothermia | Control | Time of Scr Sampling | Additional Information |
|---|---|---|---|---|---|---|---|
| Lee et al. 2017 [36] | 72 | Observational, prospective study | (1) Blood gas pH <7.15 or base deficit >10 mmol/L + moderate to severe encephalopathy OR (2) acute perinatal event and 10 min APGAR <5, OR assisted ventilation for 10 min after birth, and moderate to severe encephalopathy | WBH for 72 h (NICHD) | / | Max creatinine measurement between 24 h and 96 h of age | Scr assay: not mentioned Cooling blanket (Mul-T Blanket) |
| Sarkar et al. 2009 [37] | 28 | Observational study | Cool Cap trial | WBH for 72 h (NICHD) (n = 28) | SHC for 72 h (Cool Cap) (n = 31) | 24 h, 48 h, 72 h | Scr assay: not mentioned |
| Sarkar et al. 2014 [38] | 88 | Retrospective, observational review | Cool Cap and NICHD protocol | WBH for 72 h (NICHD) | / | Baseline, 24 h, 48 h, 72 h, d 5/7 | Scr assay: not mentioned |
| Róka, et al. 2007 [39] | 12 | Randomized controlled trial | TOBY study | WBH for 72 h (n = 12) | Normothermia (n = 9) | 6 h, 24 h, 48 h, 72 h | Scr assay: not mentioned Cooling mattress—Core temp 33–34 °C |
| Chalak et al. 2014 [40] | 20 | Prospective cohort pilot study | (1) pH 7.00 or base deficit 16 mEq/L in umbilical arterial cord plasma OR (2) history of an acute perinatal event and either no blood gas available or a pH from cord arterial serum ranging from 7.01 to 7.15 or a base deficit from 10 to 15.9 mEq/L AND (3) 10 min APGAR score <5 OR assisted ventilation at birth, AND moderate or severe encephalopathy | WBH for 72 h (NICHD) | / | Within the first 24 h | Scr assay: not mentioned cooling blanket (Blanketrol II) |
| La Haye-Caty et al. 2020 [41] | 202 | Retrospective review | (1) History of an acute perinatal event, cord pH ≤7.0 or base deficit ≤−16 mEq/L OR (2) evidence of neonatal distress, such as an APGAR score ≤5 at 10 min, postnatal blood gas pH obtained within the first hour of life ≤7.0 or base deficit ≤−16 mEq/L OR (3) a continued need for ventilation initiated at birth and for at least 10 min AND (4) moderate to severe neonatal encephalopathy | WBH for 72 h (NICHD) | / | Scr on admission; highest Scr during hospitalization; difference between both | Scr assay: not mentioned |
| Gupta et al. 2016 [42] | 106 | Retrospective review | (1) Metabolic acidosis OR (2) need for prolonged resuscitation AND moderate to severe encephalopathy | WBH for 72 h (NICHD) | / | Scr assay: Jaffe, Siemens Dimension RXL Chemistry Analyzer | |
| Tanigasalam et al. 2016 [43] | 60 | Randomized controlled trial | (1) pH ≤7 or base deficit ≥12 mEq in cord blood (2) AND 2 of the following: APGAR 10 min ≤5, fetal distress, assisted ventilation for at least 10 min after birth, evidence of any organ dysfunction AND encephalopathy. | WBH for 72 h (n = 60) | Standard treatment (n = 60) | 6 h, 36 h, 72 h | Scr assay: not mentioned. Pre-cooled gel packs (±4) to keep core temperature between 33–34 °C (chest, abdomen, back, head, axilla). Continuous rectal and skin temperature monitoring. Every 15 min for the first four h, every 2 h for the next 68 h. After cooling, gel packs were removed and radiant warmer was set at 0.5 °C/h to reach the target temperature of 36.5 °C in the next 6 h. |
| Selewski et al. 2013 [44] | 53 | Retrospective review | Cool Cap trial | WBH (n = 53) (NICHD) | SHC (n = 43) | 6 h, 24 h, 48 h, 72 h, d5, d7, d10 (as clinically indicated) | Scr assay: not mentioned |
| Frymoyer et al. 2013 [45] | 61 | Retrospective chart review | One or more of the following: APGAR score <5 (at 10 min of life), history of prolonged resuscitation at birth, presence of severe acidosis defined as a cord pH or any arterial or venous pH <7 within 60 min of birth, or a base deficit >−12 from cord blood or any arterial blood gas within 60 min of life AND moderate–severe encephalopathy | WBH for 72 h with gentamicin at Q36 (n = 27) OR WBH for 72 h with gentamicin at Q24 (n = 34) | / | d2 | Scr assay: not mentioned. Blanket cooling device (Cincinnati Subzero Blanketrol III). Rectal monitoring keeping core temperature at 33.5 °C. |
| Chock et al. 2018 [46] | 38 | Retrospective review | NICHD criteria | WBH for 72 h (NICHD) | / | d1, d2, d3, d4 | Scr assay: enzymatic (isotope dilution mass spectrometry traceable, IDMS). Cincinnati Sub-Zero Hyper- Hypothermia Blanketrol system (Cincinnati Sub-Zero, Cincinnati, Ohio). |
| Oncel et al. 2016 [47] | 41 | Prospective nested case-control study | TOBY study criteria AND Sarnat stage II or III | WBH (n = 41) | Healthy controls (n = 20) | 24 h, 48 h, 72 h results: d1, d4 | Scr assay: not mentioned Cooling at rectal temperature of 33–34 °C with Tecotherm TS med 200 n (Inspiration Healthcare Ltd., Leicester, UK). After cooling, rewarming with 0.5 °C, reaching normal body temperature within 8 h. |
| Battin et al. 2003 [48] | 13 | Randomized controlled trial | (1) Gestational age >37 w OR (2) 5 min APGAR <6 OR cord/first pH <7.1 AND (3) encephalopathy consisting of lethargy/stupor, hypotonia, and abnormal reflexes including an absent or weak suck | SHC (rectal T 34.5–35 °C, WBH) (n = 13) | SHC + normothermic (n = 13) | Scr assay: not mentioned Cooling cap: Silclear tubing (Degania Silicone Ltd., Degania Bet, Israel) and a commercially made device (Olympic Medical, Seattle, WA). Initial water temperature: 10 °C. Continuous monitoring of rectal, fontanelle and nasopharyngeal temperature and keeping rectal temperature at 34.5 °C ± 0.5 °C–35 °C ± 0.5 °C or normothermic. After cooling, rewarming at 0.5 °C/h until temperature reached the normal range. |
| Lee et al. [36] | Sarkar. et al. 2009 [37] | Sarkar el al. 2014 [38] | Roka et al. [39] | Chalak et al. [40] | La Haye-Cathy et al. [41] | Gupta et al. [42] | Tangi-salam et al. [43] | Selewski et al. [44] | Frymoyer et al. [45] | Chock et al. [46] | Oncel et al. [47] | Battin et al. [48] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| mean gestational age (w) | 38 6/7 ± 1 5/7 | 38.5 ± 1.7 | / | / | 39 ± 2 | 39.15 ± 1.6 | 38.7 | 39.5 ± 1.3 | 39 ± 1.6 | 39.7 ± 1.6 | 38.6 ± 2 | 38.7 ± 1.6 | 40.1 ± 1.6 |
| mean birth weight (g) | 3161 ± 869 | 3112 ± 755 | / | / | 3156 ± 624 | 3375 ± 626 | 3305 | 2690 ± 340 | 3313 ± 618 | 3340 ± 600 | 3258 ± 653 | 3264 ± 509 | 3634 ± 598 |
| median Apgar 5 min (IQR) | 4 (2–5) | 68%: 0–3, 20%: 4–5, 12%: ≥6 | / | / | 6(5–7) | / | / | / | (Median, SD) 3 ± 2 | 3.4 ± 2 | 4(0–9) | 30% < 5 | 4.5 (0–7) |
| median Apgar 10 min (IQR) | 5 (3–7) | 33%: 0–3, 45%: 4–5, 22%: ≥6 | / | / | / | / | / | 5 (3–6) | / | 5 ± 2 | / | / | / |
| female (%) | 41% | 36% | / | / | 30% | 44% | 41% | / | 43% | / | 44% | 77% | / |
| Study | Outcome Measure | Median Scr (Range) 0–72 h | Maximal Scr | Scr,6 h | Scr, 24 h | Scr, 36 h | Scr, 48 h | Scr, 72 h | Scr, 96 h | Scr, 5 d | Scr, 7 d |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lee et al. 2017 [36] | Scr during HT–NT–RW, (mean, SD) | 0.9 (0.6) | |||||||||
| Sarkar et al. 2009 [37] | Scr, during HT (median, IQR) | 1 (0.8, 1.4) | 1 (0.8, 1.3) | ||||||||
| Sarkar et al. 2014 [38] | Scr, during HT + RW (mean, SEM) | 0.9 ± 0.1 | 0.9 ± 0.2 | 0.9 ± 0.3 | 0.8 ± 0.4 | 0.8 ± 0.4 | |||||
| Róka et al. 2007 [39] | Scr during HT (median, IQR) | 1.04 (0.87–1.15) | 0.8 (0.73–0.99) | 0.65 (0.5–0.74) | 0.57 (0.47–0.69) | ||||||
| Chalak et al. 2014 [40] | Scr (median, IQR) | 1 (0.8–1.5) | |||||||||
| La Haye-Caty, et al. 2019 [41] | Scr (mean, SD, or median, IQR) | 1.02 ± 0.3 | 0.95 ± 0.29 | highest 0.95 (0.79–1.13) | highest 0.66 (0.5–0.92) | highest 0.48 (0.35–0.66) | highest 0.45 (0.36–0.66) | ||||
| Gupta et al. 2016 [42] | Scr (median) | 1.09 | 0.66 | 0.65 | 0.51 | ||||||
| Tanigasalam et al. 2016 [43] | Scr (mean, SD) | 1.15 ± 0.31 | 1.13 ± 0.33 | 1.195 ± 0.55 | |||||||
| Selewski et al. 2013 [44] | Scr (mean, SD) | 0.97 ± 0.26 | 1 ± 0.42 | 0.91 ± 0.57 | 0.85 ± 0.65 | 0.79 ± 0.75 | 0.74 ± 0.88 discharge: 0.49 ± 0.49 | ||||
| Frymoyer et al. 2013 [45] | Scr, range or mean, SD | range (d2): 0.5–1.5 | 1 ± 0.2 | ||||||||
| Chock et al. 2018 [46] | Scr (mean, SD) | 1.2 (0.23) | 0.9 (0.34) | 0.7 (0.37) | 0.6 (0.40) | ||||||
| Oncel et al. 2016 [47] | Scr (mean, SD) | 1.02 ± 0.37 | 0.83 ± 0.5 | ||||||||
| Battin et al. 2003 [48] | Scr (mean, SD) | 1.6 ± 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borloo, N.; Smits, A.; Thewissen, L.; Annaert, P.; Allegaert, K. Creatinine Trends and Patterns in Neonates Undergoing Whole Body Hypothermia: A Systematic Review. Children 2021, 8, 475. https://doi.org/10.3390/children8060475
Borloo N, Smits A, Thewissen L, Annaert P, Allegaert K. Creatinine Trends and Patterns in Neonates Undergoing Whole Body Hypothermia: A Systematic Review. Children. 2021; 8(6):475. https://doi.org/10.3390/children8060475
Chicago/Turabian StyleBorloo, Noor, Anne Smits, Liesbeth Thewissen, Pieter Annaert, and Karel Allegaert. 2021. "Creatinine Trends and Patterns in Neonates Undergoing Whole Body Hypothermia: A Systematic Review" Children 8, no. 6: 475. https://doi.org/10.3390/children8060475
APA StyleBorloo, N., Smits, A., Thewissen, L., Annaert, P., & Allegaert, K. (2021). Creatinine Trends and Patterns in Neonates Undergoing Whole Body Hypothermia: A Systematic Review. Children, 8(6), 475. https://doi.org/10.3390/children8060475