
Evaluation of the Erosive and Cariogenic Potential of Over-the-Counter Pediatric Liquid Analgesics and Antipyretics


Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Samples
2.2. Measurement of Acidity
2.3. Measurement of the Buffering Capacity
2.4. Evaluation of Dental Erosion Potential Using the International Organization for Standardization (ISO) Method
2.5. Measurement of Sugar Content
2.6. Statistical Analysis
3. Results
3.1. Acidity of Experimental Groups
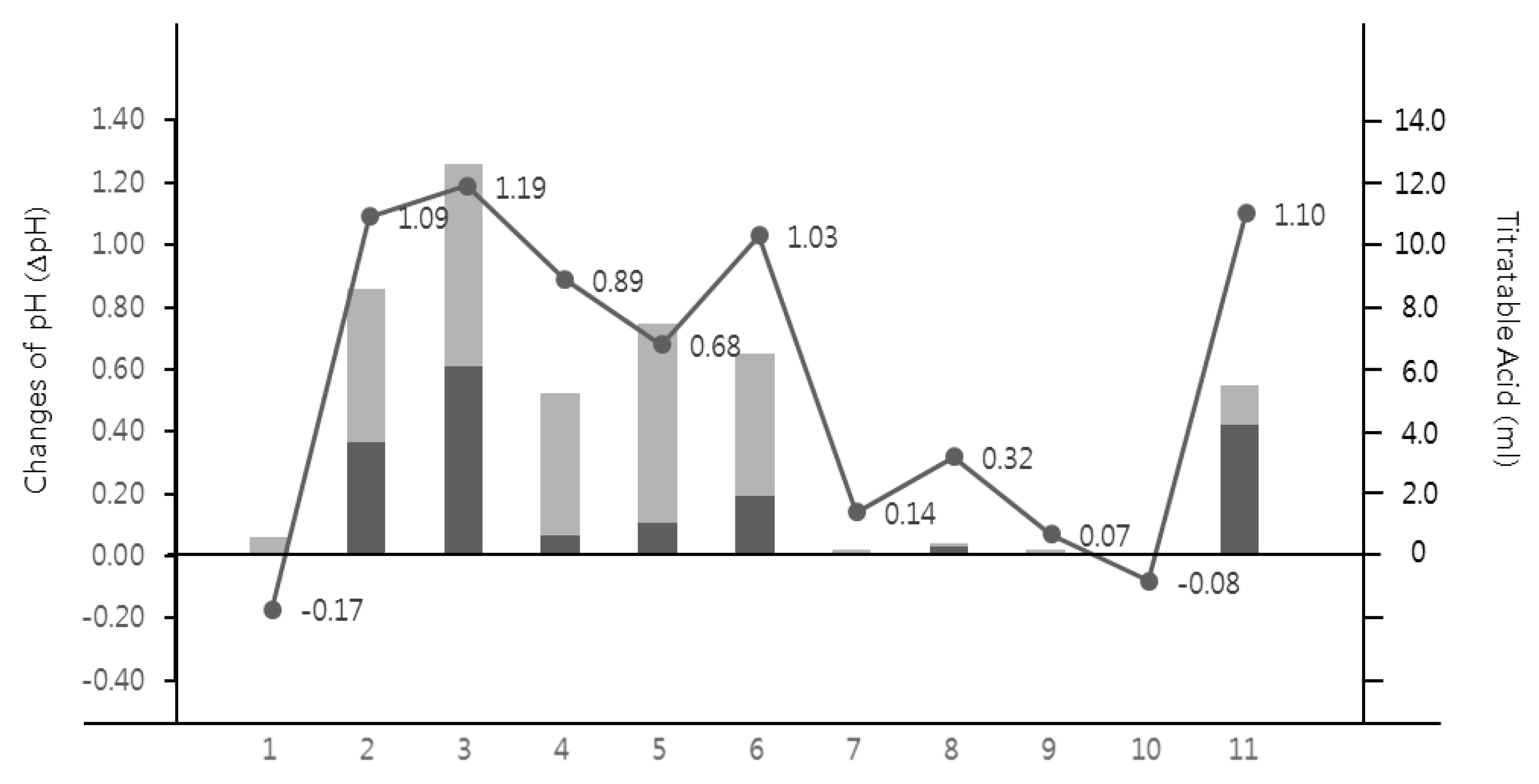
3.2. TA of Experimental Groups
3.3. Evaluation of Erosive Potential According to the ISO Method
3.4. Sugar Content for Liquid Analgesics and Antipyretics
3.5. Relationship between pH and Erosive Potentials
3.6. Relationship between Buffer Capacity and Dental Erosion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jarvinen, V.; Rytomaa, I.; Heinonen, O. Risk factors in dental erosion. J. Dent. Res. 1991, 70, 942–947. [Google Scholar] [CrossRef] [Green Version]
- Scheutzel, P. Etiology of dental erosion–intrinsic factors. Eur. J. Oral Sci. 1996, 104, 178–190. [Google Scholar] [CrossRef]
- Lussi, A.; Schlüter, N.; Rakhmatullina, E.; Ganss, C. Dental erosion–an overview with emphasis on chemical and histopathological aspects. Caries Res. 2011, 45, 2–12. [Google Scholar] [CrossRef]
- Dawes, C. What is the critical pH and why does a tooth dissolve in acid? J. Can. Dent. Assoc. 2003, 69, 722–725. [Google Scholar] [PubMed]
- Alves, L.S.; Brusius, C.D.; Damé-Teixeira, N.; Maltz, M.; Susin, C. Dental erosion among 12-year-old schoolchildren: A population-based cross-sectional study in South Brazil. Int. Dent. J. 2015, 65, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Chau, A.M.; Lo, E.C.; Chu, C.-H. Dental caries and erosion status of 12-year-old Hong Kong children. BMC Public Health 2014, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Mantonanaki, M.; Koletsi-Kounari, H.; Mamai-Homata, E.; Papaioannou, W. Dental erosion prevalence and associated risk indicators among preschool children in Athens, Greece. Clin. Oral Investig. 2013, 17, 585–593. [Google Scholar] [CrossRef]
- Scatena, C.; Galafassi, D.; Gomes-Silva, J.M.; Borsatto, M.C.; Serra, M.C. In vitro erosive effect of pediatric medicines on deciduous tooth enamel. Braz. Dent. J. 2014, 25, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennella, J.A.; Spector, A.C.; Reed, D.R.; Coldwell, S.E. The bad taste of medicines: Overview of basic research on bitter taste. Clin. Ther. 2013, 35, 1225–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durward, C.; Thou, T. Dental caries and sugar-containing liquid medicines for children in New Zealand. N. Z. Dent. J. 1997, 93, 124–129. [Google Scholar]
- Nishida, C.; Uauy, R.; Kumanyika, S.; Shetty, P. The joint WHO/FAO expert consultation on diet, nutrition and the prevention of chronic diseases: Process, product and policy implications. Public Health Nutr. 2004, 7, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B.; Ave, H. The Revised Nutrition Facts Label A Step Forward and More Room for Improvement. JAMA 2016, 316, 583–584. [Google Scholar]
- Donaldson, M.; Goodchild, J.H.; Epstein, J.B. Sugar content, cariogenicity, and dental concerns with commonly used medications. J. Am. Dent. Assoc. 2015, 146, 129–133. [Google Scholar] [CrossRef]
- Kim, S.K.; Park, S.W.; Kang, S.M.; Kwon, H.K.; Kim, B.I. Assessment of the erosive potential of carbonated waters. J. Korean Acad. Oral Health 2015, 39, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y. Evidence-based upper respiratory infection prescription. J. Korean Med Assoc. 2003, 46, 851–857. [Google Scholar] [CrossRef] [Green Version]
- Fialkowski, A.; Gernez, Y.; Arya, P.; Weinacht, K.G.; Kinane, T.B.; Yonker, L.M. Insight into the pediatric and adult dichotomy of COVID-19: Age-related differences in the immune response to SARS-CoV-2 infection. Pediatric Pulmonol. 2020, 55, 2556–2564. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.E.; Farrar, H.C. Fever and antipyretic use in children. Pediatrics 2011, 127, 580–587. [Google Scholar] [CrossRef] [Green Version]
- Babu, K.G.; Doddamani, G.M.; Naik, L.K.; Jagadeesh, K. Pediatric liquid medicaments–are they cariogenic? An in vitro study. J. Int. Soc. Prev. Community Dent. 2014, 4, 108. [Google Scholar] [CrossRef] [Green Version]
- Cavalcanti, A.L.; Fernandes, L.V.; Barbosa, A.S.; Vieira, F.F. pH, Titratable Acidity and Total Soluble Solid Content of Pediatric Antitussive Medicines. Acta Stomatol. Croat. 2008, 42, 164–170. [Google Scholar]
- Tupalli, A.R.; Satish, B.; Shetty, B.R.; Battu, S.; Kumar, J.P.; Nagaraju, B. Evaluation of the erosive potential of various pediatric liquid medicaments: An in-vitro study. J. Int. Oral Health 2014, 6, 59. [Google Scholar] [PubMed]
- Saeed, S.; Bshara, N.; Trak, J.; Mahmoud, G. Effect of dietary combinations on plaque pH recovery after the intake of pediatric liquid analgesics. Eur. J. Dent. 2015, 9, 340. [Google Scholar] [CrossRef]
- Reddy, A.; Norris, D.F.; Momeni, S.S.; Waldo, B.; Ruby, J.D. The pH of beverages available to the American consumer. J. Am. Dent. Assoc. 2016, 147, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meurman, J.; Ten Gate, J. Pathogenesis and modifying factors of dental erosion. Eur. J. Oral Sci. 1996, 104, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, S.; Kirchner, G.; Bizhang, M.; Benedix, M. Influence of various acidic beverages on tooth erosion. Evaluation by a new method. PLoS ONE 2015, 10, e0129462. [Google Scholar] [CrossRef] [PubMed]
- Benjakul, P.; Chuenarrom, C. Association of dental enamel loss with the pH and titratable acidity of beverages. J. Dent. Sci. 2011, 6, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Hunter, L.; Patel, S.; Rees, J. The in vitro erosive potential of a range of baby drinks. Int. J. Paediatr. Dent. 2009, 19, 325–329. [Google Scholar] [CrossRef]
- Lee, K.-S.; Kim, N.-J.; Lee, E.-H.; Cho, J.-W. Cariogenic potential index of fruits according to their viscosity and sugar content. Int. J. Clin. Prev. Dent. 2014, 10, 255–258. [Google Scholar] [CrossRef]
- Xavier, A.F.C.; Moura, E.F.; Azevedo, W.F.; Vieira, F.F.; Abreu, M.H.; Cavalcanti, A.L. Erosive and cariogenicity potential of pediatric drugs: Study of physicochemical parameters. BMC Oral Health 2013, 13, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jun, M.-K.; Lee, D.-H.; Lee, S.-M. Assessment of nutrient and sugar content and ph of some commercial beverages. J. Dent. Hyg. Sci. 2016, 16, 464–471. [Google Scholar] [CrossRef] [Green Version]
- Paglia, L. The sweet danger of added sugars. Eur. J. Paediatr. Dent 2019, 20, 89. [Google Scholar]


{kind=link}
| Brand Name | Manufacturer | Clinical Composition | ||
|---|---|---|---|---|
| Sweetening Agent | Others | |||
| Experimental group | Maxibookids Syrup a | Hanmi Pharm. Co., Ltd. (Seoul, Korea) | Sugar, high fructose corn syrup | Xanthan gum, citric acid hydrate, polysorbate 80, propyl p-hydroxybenzoate, betadex, D-sorbitol solution, methyl p-hydroxybenzoate, sodium citrate hydrate, sodium benzoate, magnesium aluminosilicate, agar |
| Greenfen Easy Syrup a | Mcnulty Pharmaceutical (Chungcheongnam-do, Korea) | Sucralose, high fructose corn syrup, acesulfame potassium | Xanthan gum, citric acid hydrate, polysorbate 80, propyl p-hydroxybenzoate, concentrated glycerin, methyl p-hydroxybenzoate, sodium citrate hydrate, mixed fruit flavor, sodium benzoate, agar | |
| Cokidsfen Syrup a | Kolon Pharmaceuticals, Inc. (Seoul, Korea) | Sugar, sucralose | Xanthan gum, citric acid hydrate, sodium benzoate, cellulose microcrystalline and carboxymethylcellulose, propyl p-hydroxybenzoate, concentrated glycerin, sodium citrate hydrate, D-sorbitol solution, polysorbate 80, methyl p-hydroxybenzoate, kaolin light | |
| Champ Ibufen Syrup b | Dong A Pharmaceutical Co., Ltd. (Seoul, Korea) | Sugar, sucralose | D-sorbitol solution, concentrated glycerin, cellulose microcrystalline and carboxymethylcellulose, citric acid, xanthan gum, polysorbate 80, propylene glycol | |
| Greenfen Syrup b | GC Pharma Korea (Gyeonggi-do, Korea) | Xylitol, steviol glycoside | Orange essence, sodium chloride, citric acid hydrate, propyl p-hydroxybenzoate, carboxymethylcellulose, agar, glycerin, sodium citrate hydrate, magnesium aluminum silicate, polysorbate 80, methyl p-hydroxybenzoate | |
| Children’s Brufen Syrup b | Samil Pharmaceutical Co., Ltd. (Seoul, Korea) | Sugar | Citric acid hydrate, propyl p-hydroxybenzoate, concentrated glycerin, polysorbate 80, methyl p-hydroxybenzoate, sodium benzoate, kaolin, sodium citrate hydrate, agar, D-sorbitol solution | |
| Champ Syrup c | Dong-A Pharmaceutical Co., Ltd. (Seoul, Korea) | Sugar, sucralose | D-sorbitol solution, citric acid, propylene glycol, xanthan gum, cellulose microcrystalline and carboxymethylcellulose, concentrated glycerin | |
| Coldaewon Kidsfen Syrup c | Daewon Pharmaceutical Co., Ltd. (Seoul, Korea) | Sugar, sucralose | Cellulose microcrystalline and carboxymethylcellulose, xanthan gum, povidone, citric acid, propylene glycol, concentrated glycerin, citrus flavor, D-sorbitol solution | |
| Children’s Tylenol Suspension c | Janssen Korea Co., Ltd. (Seoul, Korea) | Sucrose, sucralose, sorbitol solution 70% | Propylene glycol, propyl p-hydroxybenzoate, bitter mask, anhydrous citric acid, glycerin, cellulose microcrystalline and carboxymethylcellulose, butyl paraoxybenzoate, xanthan gum | |
| Negative control group | JeJu Samdasu | Kwang Dong Pharmaceutical Co., Ltd. (Seoul, Korea) | - | Bedrock groundwater |
| Positive control group | Yakult | Korea Yakult Co., Ltd. (Kyeonggi-do, Korea) | Sucralose | Sodium, carbohydrate, saccharide, sugar alcohol, protein, calcium |
| Brand Name | pH | Titratable Acid (mL) | ∆pH | Brix% | |
|---|---|---|---|---|---|
| TA5.5 | TA7.0 | ||||
| Maxibookids Syrup | 5.68 ± 0.02 a | 0.00 ± 0.00 a | 0.59 ± 0.02 a | −0.17 ± 0.04 a | 83.30 ± 2.89 a |
| Greenfen Easy Syrup | 3.40 ± 0.01 b | 3.67 ± 0.29 b | 8.69 ± 0.33 b | 1.09 ± 0.01 b,c | 10.03 ± 0.06 b |
| Cokidsfen Syrup | 3.78 ± 0.01 c | 6.14 ± 0.27 c | 12.75 ± 0.29 c | 1.19 ± 0.02 c | 50.67 ± 0.58 c |
| Champ Ibufen Syrup | 3.80 ± 0.02 c | 0.65 ± 0.01 d,e | 5.29 ± 0.20 d | 0.89 ± 0.04 d | 63.00 ± 0.00 d |
| Greenfen Syrup | 4.52 ± 0.04 d | 1.08 ± 0.04 e | 7.57 ± 0.39 e | 0.68 ± 0.03 e | 51.00 ± 1.00 c |
| Children’s Brufen Syrup | 3.85 ± 0.01 c | 1.96 ± 0.06 f | 6.60 ± 0.26 f | 1.03 ± 0.01 b | 80.00 ± 0.00 a,e |
| Champ Syrup | 4.79 ± 0.02 e | 0.09 ± 0.01 a | 0.19 ± 0.01 a | 0.14 ± 0.03 f | 70.67 ± 0.58 f |
| Coldaewon Kidsfen Syrup | 4.41 ± 0.06 d | 0.28 ± 0.03 a,d | 0.38 ± 0.03 a | 0.32 ± 0.06 g | 79.00 ± 1.00 e |
| Children’s Tylenol Suspension | 5.25 ± 0.00 f | 0.04 ± 0.01 a | 0.16 ± 0.00 a | 0.07 ± 0.01 f | 62.00 ± 1.00 d |
| Water | 7.79 ± 0.05 g | 0.00 ± 0.00 a | 0.00 ± 0.00 a | −0.08 ± 0.03 a | 0.00 ± 0.00 g |
| Korea Yakult | 3.59 ± 0.02 h | 4.27 ± 0.02 g | 5.57 ± 0.02 d | 1.10 ± 0.01 b,c | 18.30 ± 0.00 h |
| pH | Titratable Acid | ∆pH | Brix | |
|---|---|---|---|---|
| TA5.5 | TA7.0 | |||
| r | −0.891 * | −0.752 * | −0.918 * | 0.251 |
| p | <0.0001 | <0.0001 | <0.0001 | 0.158 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, E.-H.; Jun, M.-K. Evaluation of the Erosive and Cariogenic Potential of Over-the-Counter Pediatric Liquid Analgesics and Antipyretics. Children 2021, 8, 611. https://doi.org/10.3390/children8070611
Jung E-H, Jun M-K. Evaluation of the Erosive and Cariogenic Potential of Over-the-Counter Pediatric Liquid Analgesics and Antipyretics. Children. 2021; 8(7):611. https://doi.org/10.3390/children8070611
Chicago/Turabian StyleJung, Eun-Ha, and Mi-Kyoung Jun. 2021. "Evaluation of the Erosive and Cariogenic Potential of Over-the-Counter Pediatric Liquid Analgesics and Antipyretics" Children 8, no. 7: 611. https://doi.org/10.3390/children8070611
APA StyleJung, E.-H., & Jun, M.-K. (2021). Evaluation of the Erosive and Cariogenic Potential of Over-the-Counter Pediatric Liquid Analgesics and Antipyretics. Children, 8(7), 611. https://doi.org/10.3390/children8070611