
Impact of Propofol Bolus Administration on the Nociceptive Flexion Reflex Threshold and Bispectral Index in Children—A Case Series

 ,
,  ,
,
Abstract
:
1. Introduction
1.1. Clinical Assessment of Pain and Sedation
1.2. Objective Monitoring of Pain and Sedation
2. Materials and Methods
2.1. Patients
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
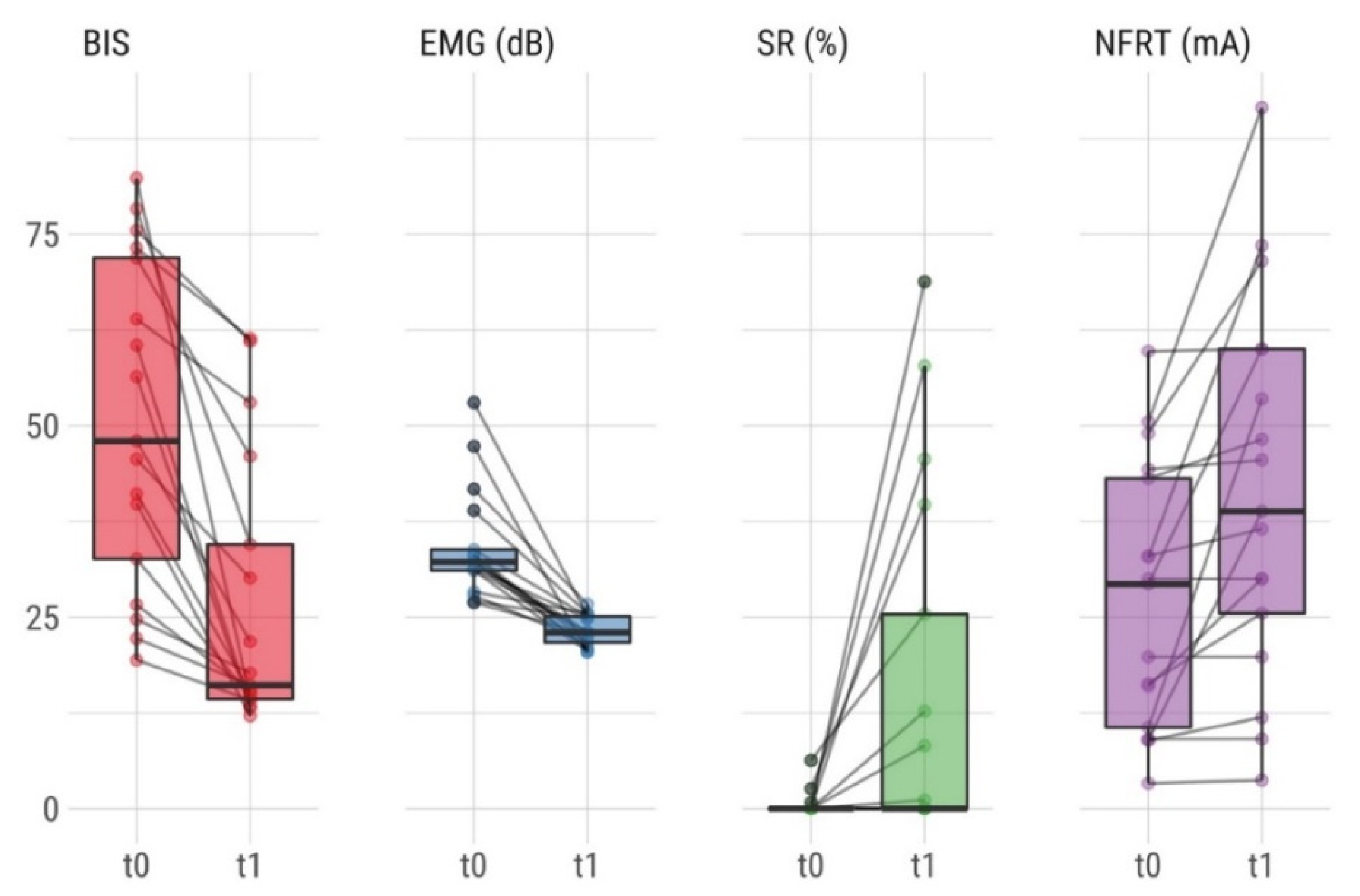
3.2. Impact of Propofol on BIS and NFRT
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stevens, B.J.; Abbott, L.K.; Yamada, J.; Harrison, D.; Stinson, J.; Taddio, A.; Barwick, M.; Latimer, M.; Scott, S.D.; Rashotte, J.; et al. Epidemiology and Management of Painful Procedures in Children in Canadian Hospitals. Can. Med. Assoc. J. 2011, 183, E403–E410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhalala, U.S.; Patel, A.; Thangavelu, M.; Sauter, M.; Appachi, E. Propofol Infusion Is a Feasible Bridge to Extubation in General Pediatric Intensive Care Unit. Front. Pediatr. 2020, 8, 255. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.K.; Trujillo-Rivera, E.; Faruqe, F.; Heneghan, J.A.; Workman, T.E.; Zeng-Treitler, Q.; Chamberlain, J.; Morizono, H.; Kim, D.; Bost, J.E.; et al. Sedation, Analgesia, and Neuromuscular Blockade: An Assessment of Practices From 2009 to 2016 in a National Sample of 66,443 Pediatric Patients Cared for in the ICU. Pediatr. Crit. Care Med. 2020, 21, e599–e609. [Google Scholar] [CrossRef]
- Kruessell, M.A.; Udink Ten Cate, F.E.; Kraus, A.-J.; Roth, B.; Trieschmann, U. Use of Propofol in Pediatric Intensive Care Units. Pediatr. Crit. Care Med. 2012, 13, e150–e154. [Google Scholar] [CrossRef]
- Harris, J.; Ramelet, A.-S.; Van Dijk, M.; Pokorna, P.; Wielenga, J.; Tume, L.; Tibboel, D.; Ista, E. Clinical Recommendations for Pain, Sedation, Withdrawal and Delirium Assessment in Critically Ill Infants and Children: An ESPNIC Position Statement for Healthcare Professionals. Intensive Care Med. 2016, 42, 972–986. [Google Scholar] [CrossRef] [Green Version]
- Playfor, S.; Jenkins, I.; Boyles, C.; Choonara, I.; Davies, G.; Haywood, T.; Hinson, G.; Mayer, A.; Morton, N.; Ralph, T.; et al. Consensus Guidelines on Sedation and Analgesia in Critically Ill Children. Intensive Care Med. 2006, 32, 1125–1136. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The Revised International Association for the Study of Pain Definition of Pain: Concepts, Challenges, and Compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Laures, E.; LaFond, C.; Hanrahan, K.; Pierce, N.; Min, H.; McCarthy, A.M. Pain Assessment Practices in the Pediatric Intensive Care Unit. J. Pediatr. Nurs. 2019, 48, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Hsu, L.; Tang, Y.; Van Dijk, M. Validation of the COMFORT Behavior Scale and the FLACC Scale for Pain Assessment in Chinese Children after Cardiac Surgery. Pain Manag. Nurs. 2012, 13, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.; Kokinsky, E. The COMFORT Behavioural Scale and the Modified FLACC Scale in Paediatric Intensive Care. Nurs. Crit. Care 2009, 14, 122–130. [Google Scholar] [CrossRef]
- Ista, E.; van Dijk, M.; Tibboel, D.; de Hoog, M. Assessment of Sedation Levels in Pediatric Intensive Care Patients Can Be Improved by Using the COMFORT “Behavior” Scale. Pediatr. Crit. Care Med. 2005, 6, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Kudchadkar, S.R.; Yaster, M.; Punjabi, N.M. Sedation, Sleep Promotion, and Delirium Screening Practices in the Care of Mechanically Ventilated Children. Crit. Care Med. 2014, 42, 1592–1600. [Google Scholar] [CrossRef]
- Jakuscheit, A.; Posch, M.J.; Gkaitatzis, S.; Neumark, L.; Hackbarth, M.; Schneider, M.; Lichtner, G.; Baars, J.H.; Von Dincklage, F. Utility of Nociceptive Flexion Reflex Threshold and Bispectral Index to Predict Movement Responses under Propofol Anaesthesia. Somatosens. Mot. Res. 2017, 34, 1–6. [Google Scholar] [CrossRef]
- Rhudy, J.L.; Green, B.A.; Arnau, R.C.; France, C.R. Taxometric Analysis of Biceps Femoris EMG Following Electrocutaneous Stimulation over the Sural Nerve: Determining the Latent Structure of the Nociceptive Flexion Reflex (NFR). Int. J. Psychophysiol. 2008, 69, 18–26. [Google Scholar] [CrossRef]
- Sandrini, G.; Serrao, M.; Rossi, P.; Romaniello, A.; Cruccu, G.; Willer, J.C. The Lower Limb Flexion Reflex in Humans. Prog. Neurobiol. 2005, 77, 353–395. [Google Scholar] [CrossRef] [PubMed]
- Von Dincklage, F.; Hackbarth, M.; Mager, R.; Rehberg, B.; Baars, J.H. Monitoring of the Responsiveness to Noxious Stimuli during Anaesthesia with Propofol and Remifentanil by Using RIII Reflex Threshold and Bispectral Index. Br. J. Anaesth. 2010, 104, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Von Dincklage, F.; Velten, H.; Rehberg, B.; Baars, J.H. Monitoring of the Responsiveness to Noxious Stimuli during Sevoflurane Mono-Anaesthesia by Using RIII Reflex Threshold and Bispectral Index. Br. J. Anaesth. 2010, 104, 740–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baars, J.H.; Mager, R.; Dankert, K.; Hackbarth, M.; Von Dincklage, F.; Rehberg, B. Effects of Sevoflurane and Propofol on the Nociceptive Withdrawal Reflex and on the H Reflex. Anesthesiology 2009, 111, 72–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadhasivam, S.; Ganesh, A.; Robison, A.; Kaye, R.; Watcha, M.F. Validation of the Bispectral Index Monitor for Measuring the Depth of Sedation in Children. Anesth. Analg. 2006, 102, 383–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, V.; Deindl, P.; Goeral, K.; Czaba, C.; Weninger, M.; Berger, A.; Olischar, M.; Werther, T. The Power of N-PASS, AEEG, and BIS in Detecting Different Levels of Sedation in Neonates: A Preliminary Study. Paediatr. Anaesth. 2018, 28, 1096–1104. [Google Scholar] [CrossRef]
- Lamas, A.; López-Herce, J.; Sancho, L.; Mencía, S.; Carrillo, Á.; Santiago, M.J.; Martínez, V. Responsiveness to Stimuli of Bispectral Index, Middle Latency Auditory Evoked Potentials and Clinical Scales in Critically Ill Children. Anaesthesia 2008, 63, 1296–1301. [Google Scholar] [CrossRef] [PubMed]
- Malviya, S.; Voepel-Lewis, T.; Tait, A.R.; Watcha, M.F.; Sadhasivam, S.; Friesen, R.H. Effect of Age and Sedative Agent on the Accuracy of Bispectral Index in Detecting Depth of Sedation in Children. Pediatrics 2007, 120, e461–e470. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.M.; Bellini, A.; Wijayatilake, D.S.; Hamilton, M.A.; Jain, R.; Karanth, S.; Namachivayam, A. BIS Monitoring versus Clinical Assessment for Sedation in Mechanically Ventilated Adults in the Intensive Care Unit and Its Impact on Clinical Outcomes and Resource Utilization. Cochrane Database Syst. Rev. 2018, 2, CD011240. [Google Scholar] [CrossRef]
- Mauritz, M.D.; Uhlenberg, F.; Bashir-Elahi, D.; Werther, T.; Gottschalk, U.; Ebenebe, C.U.; Bergers, M.; Giordano, V.; Vettorazzi, E.; Singer, D.; et al. Prediction of Nociception in Children Using the Nociceptive Flexion Reflex Threshold and the Bispectral Index—A Prospective Exploratory Observational Study. Pediatr. Crit. Care Med. 2021. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Merkel, S.I.; Voepel-Lewis, T.; Shayevitz, J.R.; Malviya, S. The FLACC: A Behavioral Scale for Scoring Postoperative Pain in Young Children. Pediatr. Nurs. 1997, 23, 293–297. [Google Scholar]
- Carnevale, F.A.; Razack, S. An Item Analysis of the COMFORT Scale in a Pediatric Intensive Care Unit. Pediatr. Crit. Care Med. 2002, 3, 177–180. [Google Scholar] [CrossRef]
- Ambuel, B.; Hamlett, K.W.; Marx, C.M.; Blumer, J.L. Assessing Distress in Pediatric Intensive Care Environments: The COMFORT Scale. J. Pediatr. Psychol. 1992, 17, 95–109. [Google Scholar] [CrossRef]
- Von Dincklage, F.; Hackbarth, M.; Schneider, M.; Baars, J.H.; Rehberg, B. Introduction of a Continual RIII Reflex Threshold Tracking Algorithm. Brain Res. 2009, 1260, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Willer, J.C. Comparative Study of Perceived Pain and Nociceptive Flexion Reflex in Man. Pain 1977, 3, 69–80. [Google Scholar] [CrossRef]
- Giordano, V.; Edobor, J.; Deindl, P.; Wildner, B.; Goeral, K.; Steinbauer, P.; Werther, T.; Berger, A.; Olischar, M. Pain and Sedation Scales for Neonatal and Pediatric Patients in a Preverbal Stage of Development. JAMA Pediatr. 2019, 173, 1186–1197. [Google Scholar] [CrossRef]
- Vet, N.J.; Ista, E.; De Wildt, S.N.; Van Dijk, M.; Tibboel, D.; De Hoog, M. Optimal Sedation in Pediatric Intensive Care Patients: A Systematic Review. Intensive Care Med. 2013, 39, 1524–1534. [Google Scholar] [CrossRef] [PubMed]
- Von Dincklage, F.; Send, K.; Hackbarth, M.; Rehberg, B.; Baars, J.H. Comparison of the Nociceptive Flexion Reflex Threshold and the Bispectral Index as Monitors of Movement Responses to Noxious Stimuli under Propofol Mono-Anaesthesia. Br. J. Anaesth. 2009, 102, 244–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamat, P.P.; McCracken, C.E.; Gillespie, S.E.; Fortenberry, J.D.; Stockwell, J.A.; Cravero, J.P.; Hebbar, K.B. Pediatric Critical Care Physician-Administered Procedural Sedation Using Propofol. Pediatr. Crit. Care Med. 2015, 16, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Playfor, S.D.; Venkatesh, K. Current Patterns of Propofol Use in PICU in the United Kingdom and North America. Pediatr. Anaesth. 2004, 14, 501–504. [Google Scholar] [CrossRef]
- Kim, J.; Yao, A.; Atherley, R.; Carstens, E.; Jinks, S.L.; Antognini, J.F. Neurons in the Ventral Spinal Cord Are More Depressed by Isoflurane, Halothane, and Propofol Than Are Neurons in the Dorsal Spinal Cord. Anesth. Analg. 2007, 105, 1020–1026. [Google Scholar] [CrossRef] [Green Version]
- Lichtner, G.; Auksztulewicz, R.; Kirilina, E.; Velten, H.; Mavrodis, D.; Scheel, M.; Blankenburg, F.; Von Dincklage, F. Effects of Propofol Anesthesia on the Processing of Noxious Stimuli in the Spinal Cord and the Brain. Neuroimage 2018, 172. [Google Scholar] [CrossRef] [PubMed]
- Rampil, I.J.; Kim, J.-S.; Lenhardt, R.; Negishi, C.; Sessler, D.I. Bispectral EEG Index during Nitrous Oxide Administration. Anesthesiology 1998, 89, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhang, J.; Yu, J.; Tian, M.; Cui, X.; Wu, A. Variation of Bispectral Index in Children Aged 1–12 Years under Propofol Anesthesia: An Observational Study. BMC Anesthesiol. 2019, 19, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, P.L.; Shintani, A.K.; Tyson, R.; Pandharipande, P.P.; Pun, B.T.; Ely, E.W. Presence of Electroencephalogram Burst Suppression in Sedated, Critically Ill Patients Is Associated with Increased Mortality. Crit. Care Med. 2008, 36, 3171–3177. [Google Scholar] [CrossRef] [Green Version]
- Koch, S.; Stegherr, A.-M.; Rupp, L.; Kruppa, J.; Prager, C.; Kramer, S.; Fahlenkamp, A.; Spies, C. Emergence Delirium in Children Is Not Related to Intraoperative Burst Suppression—Prospective, Observational Electrography Study. BMC Anesth. 2019, 19, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 8 |
|---|---|
| Male | 5 (62.5) |
| Female | 3 (37.5) |
| Age, years | 8.6 ± 3.5 |
| Bodyweight, kg | 24.0 ± 8.9 |
| Time on mechanical ventilation, days | 7.9 ± 5.5 |
| Length of PICU stay, days | 14.1 ± 9.7 |
| Mode of mechanical ventilation | |
| SIMV | 6 (75) |
| BIPAP | 2 (25) |
| Diagnostic group | |
| Non-cardiac post-operative | 4 (50) |
| Miscellaneous (including injury) | 3 (37.5) |
| Cardiac post-operative | 1 (12.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauritz, M.D.; Uhlenberg, F.; Vettorazzi, E.; Ebenebe, C.U.; Singer, D.; Deindl, P. Impact of Propofol Bolus Administration on the Nociceptive Flexion Reflex Threshold and Bispectral Index in Children—A Case Series. Children 2021, 8, 639. https://doi.org/10.3390/children8080639
Mauritz MD, Uhlenberg F, Vettorazzi E, Ebenebe CU, Singer D, Deindl P. Impact of Propofol Bolus Administration on the Nociceptive Flexion Reflex Threshold and Bispectral Index in Children—A Case Series. Children. 2021; 8(8):639. https://doi.org/10.3390/children8080639
Chicago/Turabian StyleMauritz, Maximilian David, Felix Uhlenberg, Eik Vettorazzi, Chinedu Ulrich Ebenebe, Dominique Singer, and Philipp Deindl. 2021. "Impact of Propofol Bolus Administration on the Nociceptive Flexion Reflex Threshold and Bispectral Index in Children—A Case Series" Children 8, no. 8: 639. https://doi.org/10.3390/children8080639
APA StyleMauritz, M. D., Uhlenberg, F., Vettorazzi, E., Ebenebe, C. U., Singer, D., & Deindl, P. (2021). Impact of Propofol Bolus Administration on the Nociceptive Flexion Reflex Threshold and Bispectral Index in Children—A Case Series. Children, 8(8), 639. https://doi.org/10.3390/children8080639