
Bilateral Multiple Tarsal Coalitions (Talonavicular and Talocalcaneal Coalitions) with Recurrent Ankle Sprain in an Adolescent


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
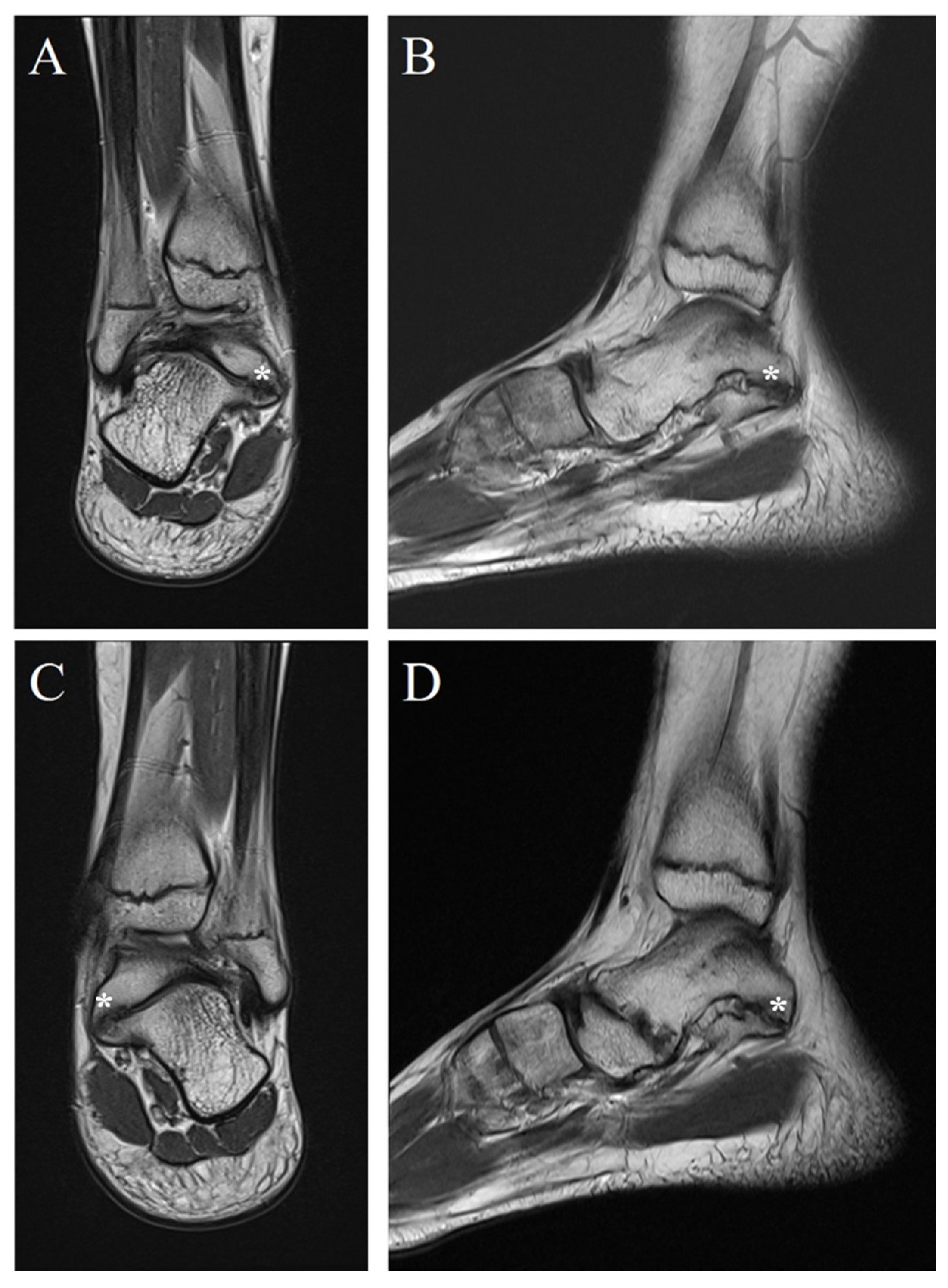
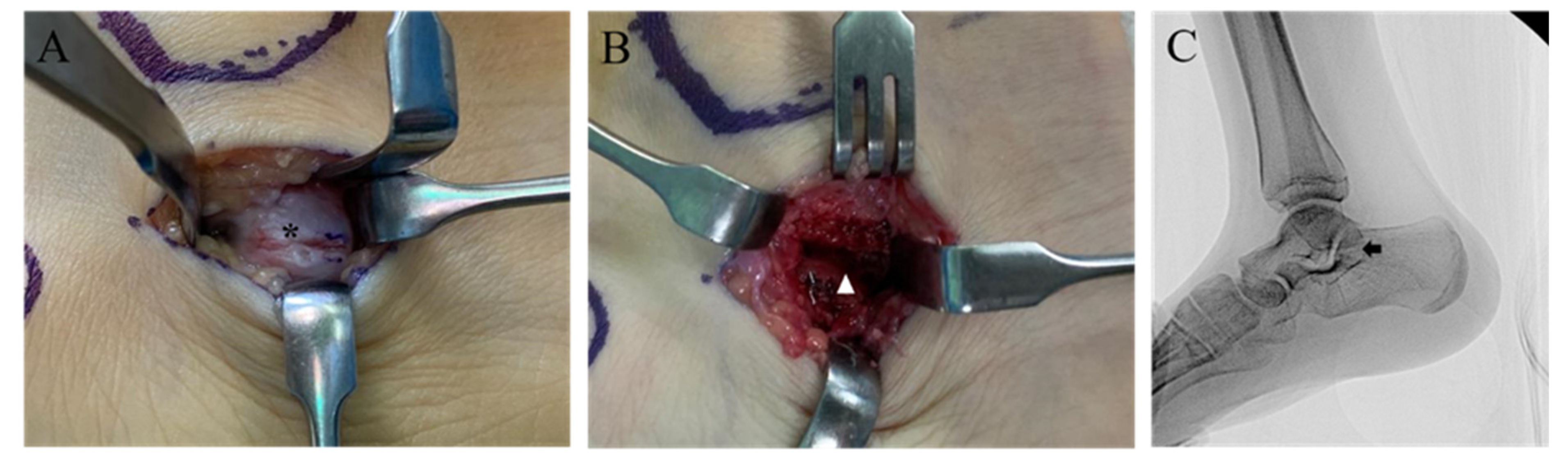
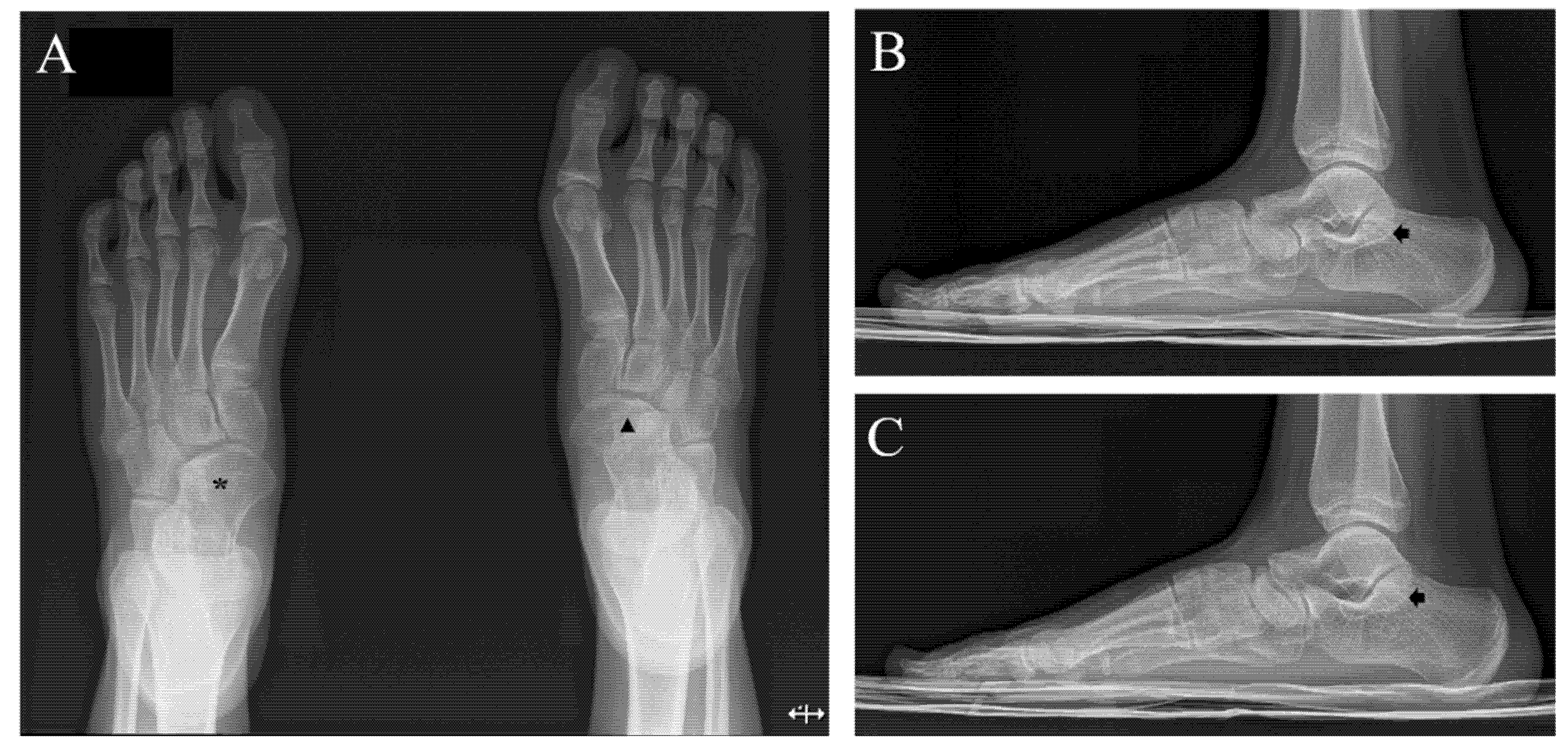
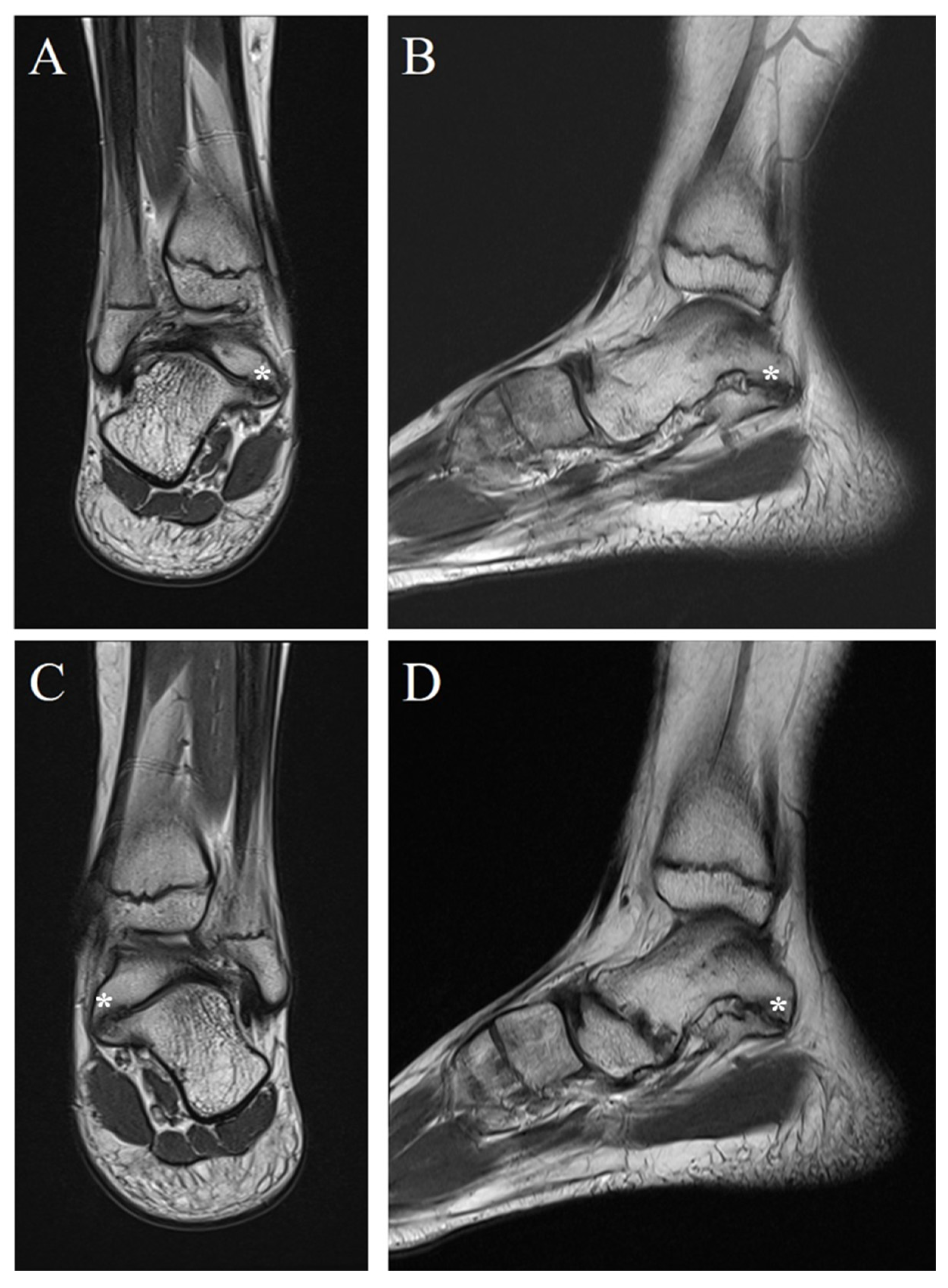
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crim, J.R.; Kjeldsberg, K.M. Radiographic Diagnosis of Tarsal Coalition. AJR Am. J. Roentgenol. 2004, 182, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Stormont, D.M.; Peterson, H.A. The Relative Incidence of Tarsal Coalition. Clin. Orthop. Relat. Res. 1983, 181, 28–36. [Google Scholar] [CrossRef]
- Zaw, H.; Calder, J.D. Tarsal Coalitions. Foot Ankle Clin. 2010, 15, 349–364. [Google Scholar] [CrossRef] [PubMed]
- David, D.R.; Clark, N.E.; Bier, J.A. Congenital Talonavicular Coalition. Review of the Literature, Case Report, and Orthotic Management. J. Am. Podiatr. Med. Assoc. 1998, 88, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Migues, A.; Slullitel, G.A.; Suárez, E.; Galán, H.L. Case Reports: Symptomatic Bilateral Talonavicular Coalition. Clin. Orthop. Relat. Res. 2009, 467, 288–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Docquier, P.L.; Maldaque, P.; Bouchard, M. Tarsal Coalition in Paediatric Patients. Orthop. Traumatol. Surg. Res. 2019, 105, S123–S131. [Google Scholar] [CrossRef] [PubMed]
- Denning, J.R. Tarsal Coalition in Children. Pediatr. Ann. 2016, 45, e139–e143. [Google Scholar] [CrossRef] [PubMed]
- Mosier, K.M.; Asher, M. Tarsal Coalitions and Peroneal Spastic Flat Foot. A Review. J. Bone Jt. Surg. Am. 1984, 66, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Brennan, S.A.; Kiernan, C.; Maleki, F.; Bergin, D.; Kearns, S.R. Talonavicular Synostosis with Lateral Ankle Instability—A Case Report and Review of the Literature. Foot Ankle Surg. 2012, 18, e34–e36. [Google Scholar] [CrossRef]
- Wright, D.G.; Desai, S.M.; Henderson, W.H. Action of the Subtalar and Ankle-Joint Complex during the Stance Phase of Walking. J. Bone Joint Surg. Am. 1964, 46, 361–382. [Google Scholar] [CrossRef]
- Doyle, S.M.; Kumar, S.J. Symptomatic Talonavicular Coalition. J. Pediatr. Orthop. 1999, 19, 508–510. [Google Scholar] [CrossRef]
- Challis, J. Hereditary Transmission of Talonavicular Coalition in Association with Anomaly of the Little Finger. J. Bone Joint Surg. Am. 1974, 56, 1273–1276. [Google Scholar] [CrossRef]
- Zeide, M.S.; Wiesel, S.W.; Terry, R.L. Talonavicular Coalition. Clin. Orthop. Relat. Res. 1977, 126, 225–227. [Google Scholar]
- Shtofmakher, G.; Rozenstrauch, A.; Cohen, R. An Incidental Talonavicular Coalition in a Diabetic Patient: A Podiatric Perspective. Case Rep. 2014, 2014, bcr2014204510. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, C.; Chu, Y.-Y. Bilateral Multiple Tarsal Coalitions (Talonavicular and Talocalcaneal Coalitions) with Recurrent Ankle Sprain in an Adolescent. Children 2022, 9, 100. https://doi.org/10.3390/children9010100
Lim C, Chu Y-Y. Bilateral Multiple Tarsal Coalitions (Talonavicular and Talocalcaneal Coalitions) with Recurrent Ankle Sprain in an Adolescent. Children. 2022; 9(1):100. https://doi.org/10.3390/children9010100
Chicago/Turabian StyleLim, Chaemoon, and Yong-Yeon Chu. 2022. "Bilateral Multiple Tarsal Coalitions (Talonavicular and Talocalcaneal Coalitions) with Recurrent Ankle Sprain in an Adolescent" Children 9, no. 1: 100. https://doi.org/10.3390/children9010100
APA StyleLim, C., & Chu, Y.-Y. (2022). Bilateral Multiple Tarsal Coalitions (Talonavicular and Talocalcaneal Coalitions) with Recurrent Ankle Sprain in an Adolescent. Children, 9(1), 100. https://doi.org/10.3390/children9010100