
Comparison of Distance and Angular Analysis for Measurement of Hamstring Flexibility in Preschoolers

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject
2.2. Procedures
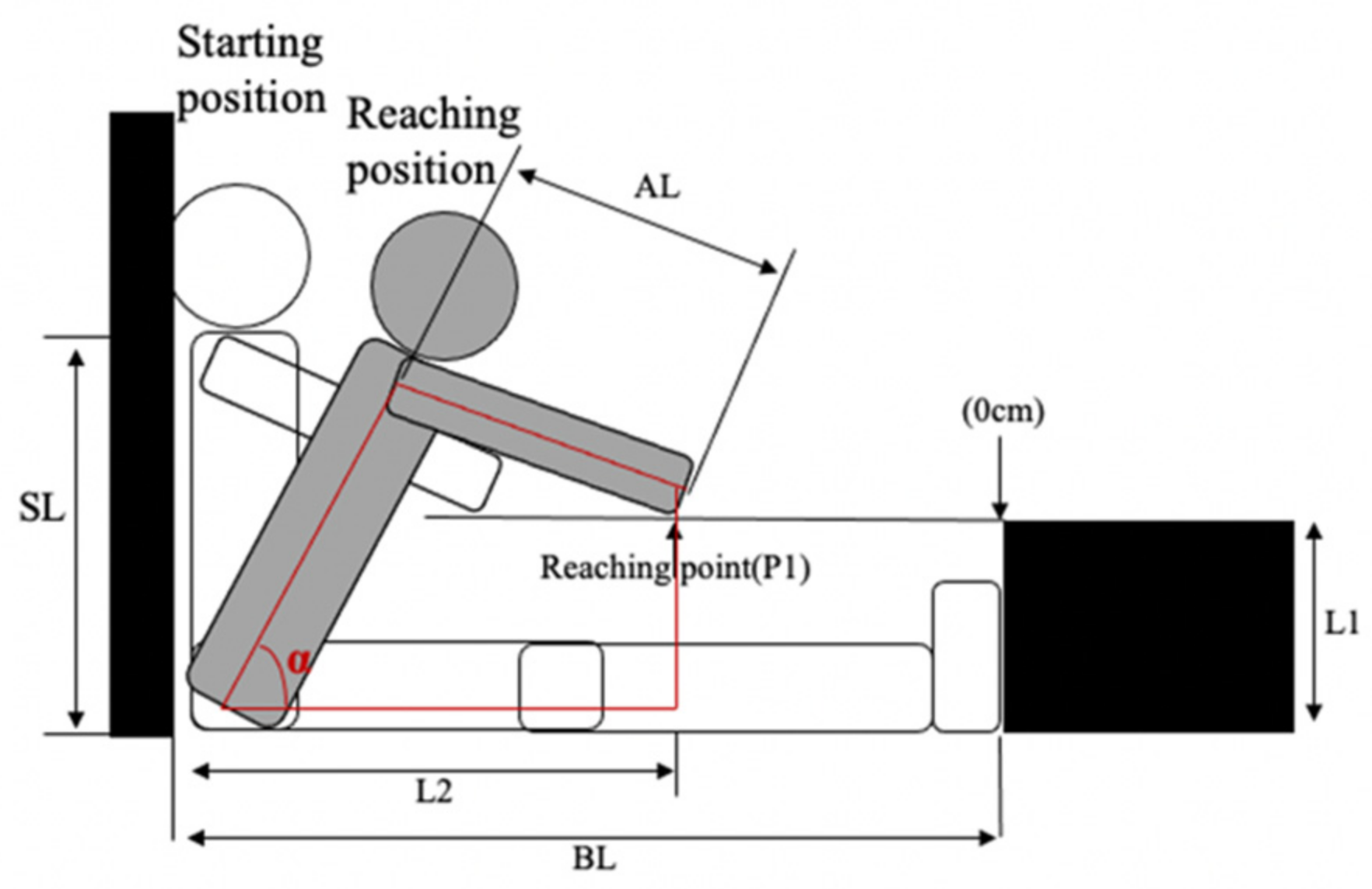
2.3. MSR Angle Calculation
2.4. MSR Distance Calculation
2.5. Statistical Analyses
3. Results
4. Discussion
4.1. Reliability and Usefulness
4.2. Elimination of the Concern of Limb-Length Bias
4.3. Practical Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Baltaci, G.; Un, N.; Tunay, V.; Besler, A.; Gerçeker, S. Comparison of three different sit and reach tests for measurement of hamstring flexibility in female university students. Br. J. Sports Med. 2003, 37, 59–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, K.F.; Dillon, E.K. The sit and reach—A test of back and leg flexibility. Res. Q. Am. Assoc. Health Phys. Educ. Recreat. 1952, 23, 115–118. [Google Scholar] [CrossRef]
- Bandy, W.D.; Irion, J.M.; Briggler, M. The effect of static stretch and dynamic range of motion training on the flexibility of the hamstring muscles. J. Orthop. Sports Phys. Ther. 1998, 27, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornbleet, S.L.; Woolsey, N.B. Assessment of hamstring muscle length in school-aged children using the sit-and-reach test and the inclinometer measure of hip joint angle. Phys. Ther. 1996, 76, 850–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeger, W.W.K.; Hopkins, D.R.; Button, S.; Palmer, T.A. Comparing the sit and reach with the modified sit and reach in measuring flexibility in adolescents. Pediatr. Exerc. Sci. 1990, 2, 156–162. [Google Scholar] [CrossRef]
- Hoeger, W.W.K.; Hopkins, D.R. A comparison of the sit and reach and the modified sit and reach in the measurement of flexibility in women. Res. Q. Exerc. Sport 1992, 63, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Castro-Piñero, J.; Chillón, P.; Ortega, F.B.; Montesinos, J.L.; Sjöström, M.; Ruiz, J.R. Criterion-related validity of sit-and-reach and modified sit-and-reach test for estimating hamstring flexibility in children and adolescents aged 6–17 years. Int. J. Sports Med. 2009, 30, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Hemmatinezhad, M.A.; Afsharnezhad, T.; Nateghi, N.; Damirchi, A. The relationship between limb length with classical and modified back saver sit-and-reach tests in student boys. Int. J. Fit. 2009, 5, 69–78. [Google Scholar]
- Kawano, M.M.; Ambar, G.; Oliveira, B.I.R.; Boer, M.C.; Cardoso, A.P.R.G.; Cardoso, J.R. Influence of the gastrocnemius muscle on the sit-and-reach test assessed by angular kinematic analysis. Braz. J. Phys. Ther. 2010, 14, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHugh, M.P.; Kremenic, I.J.; Fox, M.B.; Gleim, G.W. The role of mechanical and neural restraints to joint range of motion during passive stretch. Med. Sci. Sports Exerc. 1998, 30, 928–932. [Google Scholar] [PubMed]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, W.G. How to Interpret Changes in an Athletic Performance Test. Sportscience 2004, 8, 1–7. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence Earlbaum Associates: Hillside, NJ, USA, 1988. [Google Scholar]
- Salkind, N. Encyclopedia of Measurement and Statistics; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2012. [Google Scholar] [CrossRef]
- Ayala, F.; de Baranda, P.S.; de Ste Croix, M.; Santonja, F. Absolute reliability of five clinical tests for assessing hamstring flexibility in professional futsal players. J. Sci. Med. Sport 2012, 15, 142–147. [Google Scholar] [CrossRef] [PubMed]
- López-Miñarro, P.A.; de Baranda Andújar, P.S.; Rodríguez-García, P.L. A comparison of the sit-and-reach test and the back-saver sit-and-reach test in university students. J. Sports Sci. Med. 2009, 8, 116–122. [Google Scholar] [PubMed]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, D.R.; Hoeger, W.W.K. A comparison of the sit-and-reach test and the modified sit-and-reach test in the measurement of flexibility for males. J. Strength Cond. Res. 1992, 6, 7–10. [Google Scholar]
- López-Miñarro, P.A.; de Baranda, P.S.; Rodríguez-García, P.L.; Yuste, J.L. Comparison between sit-and-reach test and V sit-and-reach test in young adults. Gazz. Med. Ital. 2008, 167, 135–142. [Google Scholar]
- Akkurt, L.; Gürbüz, I.A.; Karaduman, A.; Yilmaz, Ö.T. Lower limb flexibility in children with Duchenne muscular dystrophy: Effects on functional performance. Pediatr. Exerc. Sci. 2019, 31, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Martos, I.; Valenza, M.C.; Valenza-Demet, G.; Benítez-Feliponi, Á.; Robles-Vizcaíno, C.; Ruiz-Extremera, Á. Repercussions of plagiocephaly on posture, muscle flexibility and balance in children aged 3–5 years old. J. Paediatr. Child Health 2016, 52, 541–546. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Age Group | N | Gender (M/F) | Height (cm) | Weight (kg) |
|---|---|---|---|---|
| 3 years | 48 | 28/20 | 102.99 ± 4.73 | 16.48 ± 2.48 |
| 4 years | 70 | 44/26 | 109.40 ± 4.67 | 18.48 ± 3.09 |
| 5 years | 76 | 47/29 | 114.49 ± 4.53 | 20.02 ± 2.67 |
| 3 Years | 4 Years | 5 Years | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | ICC (95% CI) | CV% | TE | SWC0.5 | Mean (SD) | ICC (95% CI) | CV% | TE | SWC0.5 | Mean (SD) | ICC | CV% | TE | SWC0.5 | |
| Angle (°) | 46.29 (10.33) | 0.91 (0.79–0.95) | 8.21 | 3.80 | 5.17 | 48.52 (8.45) | 0.82 (0.70–0.89) | 9.23 | 4.48 | 4.22 | 47.35 (10.89) | 0.89 (0.82–0.93) | 9.40 | 4.45 | 5.44 |
| Trial 1 | 44.90 (10.03) | 47.52 (8.27) | 46.16 (11.25) | ||||||||||||
| Trial 2 | 47.69 (10.54) | 49.52 (8.56) | 48.54 (10.44) | ||||||||||||
| Distance (cm) | 19.05 (3.96) | 0.86 (0.69–0.93) | 9.29 | 1.77 | 1.98 | 20.65 (4.94) | 0.91 (0.86–0.94) | 9.30 | 1.92 | 2.47 | 21.44 (4.37) | 0.84 (0.75–0.89) | 10.63 | 2.28 | 2.18 |
| Trial 1 | 18.85 (4.22) | 20.30 (4.96) | 21.20 (4.44) | ||||||||||||
| Trial 2 | 20.15 (3.61) | 21.01 (4.94) | 21.69 (4.31) | ||||||||||||
| MSR Angle | MSR Distance | Height | Arm Length | Sitting Height | |
|---|---|---|---|---|---|
| MSR angle | 0.430 *** | 0.041 | −0.005 | −50.006 | |
| MSR distance | 0.127 | 0.209 ** | 0.339 *** | ||
| Height | 0.841 *** | 0.637 *** | |||
| Arm length | 0.719 *** |
| Variables | 3 Years | 4 Years | 5 Years | |||
|---|---|---|---|---|---|---|
| Boys | Girls | Boys | Girls | Boys | Girls | |
| Angle (°) | 46.37 (10.12) | 46.19 (9.41) | 47.39 (7.64) | 50.42 (7.53) | 45.28 (11.69) | 50.72 (6.28) * |
| Distance (cm) | 18.90 (2.96) | 20.33 (4.37) | 20.12 (4.79) | 21.54 (4.47) | 20.62 (3.92) | 22.78 (3.87) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hua, A.; Bai, J.; Fan, Y.; Wang, J. Comparison of Distance and Angular Analysis for Measurement of Hamstring Flexibility in Preschoolers. Children 2022, 9, 39. https://doi.org/10.3390/children9010039
Hua A, Bai J, Fan Y, Wang J. Comparison of Distance and Angular Analysis for Measurement of Hamstring Flexibility in Preschoolers. Children. 2022; 9(1):39. https://doi.org/10.3390/children9010039
Chicago/Turabian StyleHua, Anke, Jingyuan Bai, Yong Fan, and Jian Wang. 2022. "Comparison of Distance and Angular Analysis for Measurement of Hamstring Flexibility in Preschoolers" Children 9, no. 1: 39. https://doi.org/10.3390/children9010039